
Abstract
Background:
Anticholinergic medications are associated with adverse outcomes in older adults and should be prescribed cautiously. We describe the Anticholinergic Risk Scale (ARS) scores of older inpatients and associations with outcomes.
Methods:
We included all emergency, first admissions of adults ⩾65 years old admitted to one hospital over 4 years. Demographics, discharge specialty, dementia/history of cognitive concern, illness acuity and medications were retrieved from electronic records. ARS scores were calculated as the sum of anticholinergic potential for each medication (0 = limited/none; 1 = moderate; 2 = strong and 3 = very strong). We categorised patients based on admission ARS score [ARS = 0 (reference); ARS = 1; ARS = 2; ARS ⩾ 3] and change in ARS score from admission to discharge [admission and discharge ARS = 0 (reference); same; decreased; increased]. We described anticholinergic prescribing patterns by discharge specialty and explored multivariable associations between ARS score categories and mortality using logistic regression [odds ratios (ORs), 95% confidence intervals (CIs)].
Results:
From 33,360 patients, 10,183 (31%) were prescribed an anticholinergic medication on admission. Mean admission ARS scores were: Cardiology and Stroke = 0.56; General Medicine = 0.78; Geriatric Medicine = 0.83; Other medicine = 0.81; Trauma and Orthopaedics = 0.66; Other Surgery = 0.65. Mean ARS did not increase from admission to discharge in any specialty but reductions varied significantly, from 4.6% (Other Surgery) to 27.7% (Geriatric Medicine) (p < 0.001). The odds of both 30-day inpatient and 30-day post-discharge mortality increased with admission ARS = 1 (OR = 1.21, 95% CI 1.01–1.44 and OR = 1.44, 1.18–1.74) but not with ARS = 2 or ARS ⩾ 3. The odds of 30-day post-discharge mortality were higher in all ARS change categories, relative to no anticholinergic exposure (same: OR = 1.45, 1.21–1.74, decreased: OR = 1.27, 1.01–1.57, increased: OR = 2.48, 1.98–3.08).
Conclusion:
The inconsistent dose–response associations with mortality may be due to confounding and measurement error which may be addressed by a prospective trial. Definitive evidence for this prevalent modifiable risk factor is required to support clinician behaviour-change, thus reducing variation in anticholinergic deprescribing by inpatient speciality.
Plain language summary
Introduction
Many medications used to treat common conditions such as depression, overactive bladder syndrome and allergy have anticholinergic properties. Anticholinergic medications have a high prevalence in older patient populations 1 and many older adults accumulate anticholinergic burden through polypharmacy. 2 Side effects include visual disturbance, dry mouth, heat intolerance, constipation, urinary retention, cognitive impairment and increased heart rate. 3 These effects are often mild but in older patients their impact can be significant due to reduced ability to metabolise and excrete drugs, and reduction in the number of cholinergic neurones in the brain.4,5
Exposure to anticholinergic medications is linked to a higher risk of incident dementia,6,7 stroke, 8 falls and fractures, 9 and post-operative delirium. 10 Therefore, clinical guidelines increasingly recommend prescribing anticholinergics cautiously in older adults, especially those with multi-morbidity, 11 frailty or dementia.12,13
Older adults are frequent users of emergency hospital services and inpatient admission episodes present an opportunity to deprescribe potentially inappropriate medications. However, deprescribing anticholinergic medications in hospitalised patients has been infrequently described and, if reported, studies are often limited to specific patient groups, for example, patients with cognitive impairment 14 or those admitted to geriatric medicine wards. 15 There is a lack of large-scale studies describing anticholinergic prescribing and deprescribing trends across a diverse group of hospitalised patients, informed by measurement of anticholinergic burden at both admission and discharge. Yet, these trends are important to understand and will help inform future interventions targeting anticholinergic burden reduction in hospitalised older people. This information would also be timely, since a recent systematic review identified only four studies examining interventions to reduce anticholinergic burden in hospitalised patients 16 and future work in this area is needed. Furthermore, associations between anticholinergic medications and mortality are controversial 17 and results have also been mixed with respect to associations with other negative hospital outcomes.18,19
Therefore, we describe the burden of prescribed anticholinergic medication, using the Anticholinergic Risk Scale (ARS), 20 in all older adults admitted as an emergency to any specialty in a large hospital in the United Kingdom. In addition, we describe how ARS scores change from admission to discharge and evaluate associations between both admission ARS and change in ARS score and hospital outcomes, primarily inpatient and post-discharge mortality.
Methods
Setting and sample
This retrospective, observational study was conducted at a National Health Service (NHS) university hospital in England. We included the first emergency admission episode of all older adults (aged ⩾65 years) admitted between 1 October 2014 and 5 November 2018. An on-site clinical informatics team retrieved data from the hospital electronic health record (EHR) system, which provides real-time recording of all aspects of patient care.
Data retrieved
Patient characteristics
Patient demographics, admission weight, laboratory values from Emergency Department (ED) point-of-care blood tests [urea (mmol/L), creatinine (µmol/L), sodium (mmol/L) and potassium (mmol/L)] and primary specialty looking after the patient on hospital discharge were retrieved from the EHR. We also retrieved the Clinical Frailty Scale (CFS) score 21 and whether patients had a history of dementia or cognitive concern. At our centre, adults ⩾75 years old are assessed within 72 h of emergency admission with respect to their frailty and cognitive status. Frailty is assessed using the CFS and patients can score between 1 (robust) and 8 (very severely frail) with a separate category for those not frail but terminally ill (a score of 9) (permission granted for clinical use by the principal investigator at Geriatric Medicine Research, Dalhousie University, Halifax, Canada). Two screening questions are used to identify cognitive impairment on admission: ‘Is there a history of dementia?’ (yes, no) and ‘is there current evidence of acute confusion?’ (yes, no). These questions provide an informative view of healthcare practitioners’ concern about their patients’ cognition, from whatever cause, in a real-world setting.
Illness acuity on admission was assessed using the maximum early warning score recorded in the ED. Until December 2016, patients were assessed using the ED Modified Early Warning Score (ED-MEWS), which ranges from 0 to 15 and quantifies the deviation of heart rate, systolic blood pressure, consciousness level, respiratory rate and temperature from normal. After December 2016, the hospital introduced the National Early Warning Score (first NEWS then NEWS2), which also takes into account requirement for supplemental oxygen and oxygen saturations. A score of ⩾4 on the ED-MEWS and ⩾5 on the NEWS or NEWS2 indicates high illness acuity in our hospital.
Medication exposure
We retrieved admission medications as recorded by the admitting doctor in a medicines reconciliation flowsheet and discharge medications from the electronic discharge summary. Topical medications, for example ointments, were removed due to limited systemic absorption. ARS score was calculated as the sum of the assigned value on a scale of 0–3 according to anticholinergic potential (0, limited or none; 1, moderate; 2, strong; and 3, very strong) of the prescribed drugs on admission and discharge separately. 20 Patients were categorised into one of three categories based on their admission medication: ARS = 0 (taking no anticholinergic medication), ARS = 1 (scoring one point on the ARS), ARS = 2 (scoring two points) and ARS ⩾ 3 (scoring three or more points). ARS score change, for those discharged alive, was categorised as: zero (ARS = 0 at admission and discharge), same (admission ARS = discharge ARS), decrease (admission ARS >discharge ARS) and increase (admission ARS < discharge ARS).
Patient outcomes
We primarily considered death within 30 days of admission and death within 30 days of discharge. Secondary outcome measures considered were prolonged length of hospital stay (⩾10 days), discharge to usual place of residence, and readmission to our hospital within 30 days of discharge.
Statistical analyses
Statistical analyses were performed using R version 3.6.0 (2019-04-26). For all data retrieved, we reported descriptive statistics as count with percentage (%) or mean with standard deviation (SD) as appropriate. In addition to describing mean ARS scores on admission and discharge, we also described the distribution (%) of patients across ARS change categories by discharge specialty. We used Wilcoxon tests (with Bonferroni corrections) to evaluate differences in the mean ARS score at admission compared with discharge within each specialty group and a Kruskal–Wallis test to compare the differences between admission and discharge ARS scores across specialties.
We then used Chi-squared and Kruskal–Wallis tests as appropriate to explore any differences in patient characteristics between ARS and ARS change categories. Associations between ARS exposure and patient outcomes were further evaluated using logistic regression. A priori, we adjusted models for age and sex (Model A), number of non-anticholinergic medications on admission (Model B), discharge specialty (Model C), illness acuity (Model D) and, finally, for history of dementia/cognitive concern (Model E). We restricted analyses to patients with complete co-variable data. We excluded those who died during the inpatient episode from analyses of 30-day readmission and 30-day post-discharge mortality and all analyses with ARS score change as the exposure.
Results
We retrieved 76,826 admission episodes, of which 37,630 were first admission episodes and 33,360 had complete data for age, sex and admission medications (admission medications missing for 1981 patients). On discharge, 3075 patients had missing information for discharge medications and 3142 patients had died during the admission episode, leaving 28,078 patients with information on admission and discharge ARS scores.
Admission ARS score
From 33,360 patients included, 10,183 (30.5%) were prescribed an anticholinergic on admission with 3266 (9.8%), 2479 (7.4%) and 4438 (13.3%) patients scoring 1, 2 or ⩾3 respectively on the ARS. The three commonest medications prescribed in each ARS score category were: ‘0’ – paracetamol, aspirin and omeprazole; ‘1’ – ranitidine, mirtazapine and metoclopramide; ‘2’ – cetirizine, loperamide and prochlorperazine; ‘3’ – amitriptyline, oxybutynin and chlorphenamine. The characteristics of patients by admission ARS score are shown in Table 1. The proportion of women, the number of anticholinergic and non-anticholinergic admission medications, and the proportion of patients re-admitted to hospital within 30 days of discharge increased with increasing ARS score. However, the most notable differences were between patients taking no anticholinergics and those with an ARS of 1, who were older, frailer, more acutely unwell, and had more cognitive impairment and worse hospital outcomes. These findings were also apparent in higher ARS categories but were not as strong and there were no ‘dose–response’ associations. Of note, across ARS categories 1, 2 and ⩾3, 12.4% (n = 1261) of patients were recorded as having dementia or a concern about their cognition.
Patient characteristics by Anticholinergic Risk Scale (ARS) category at admission.
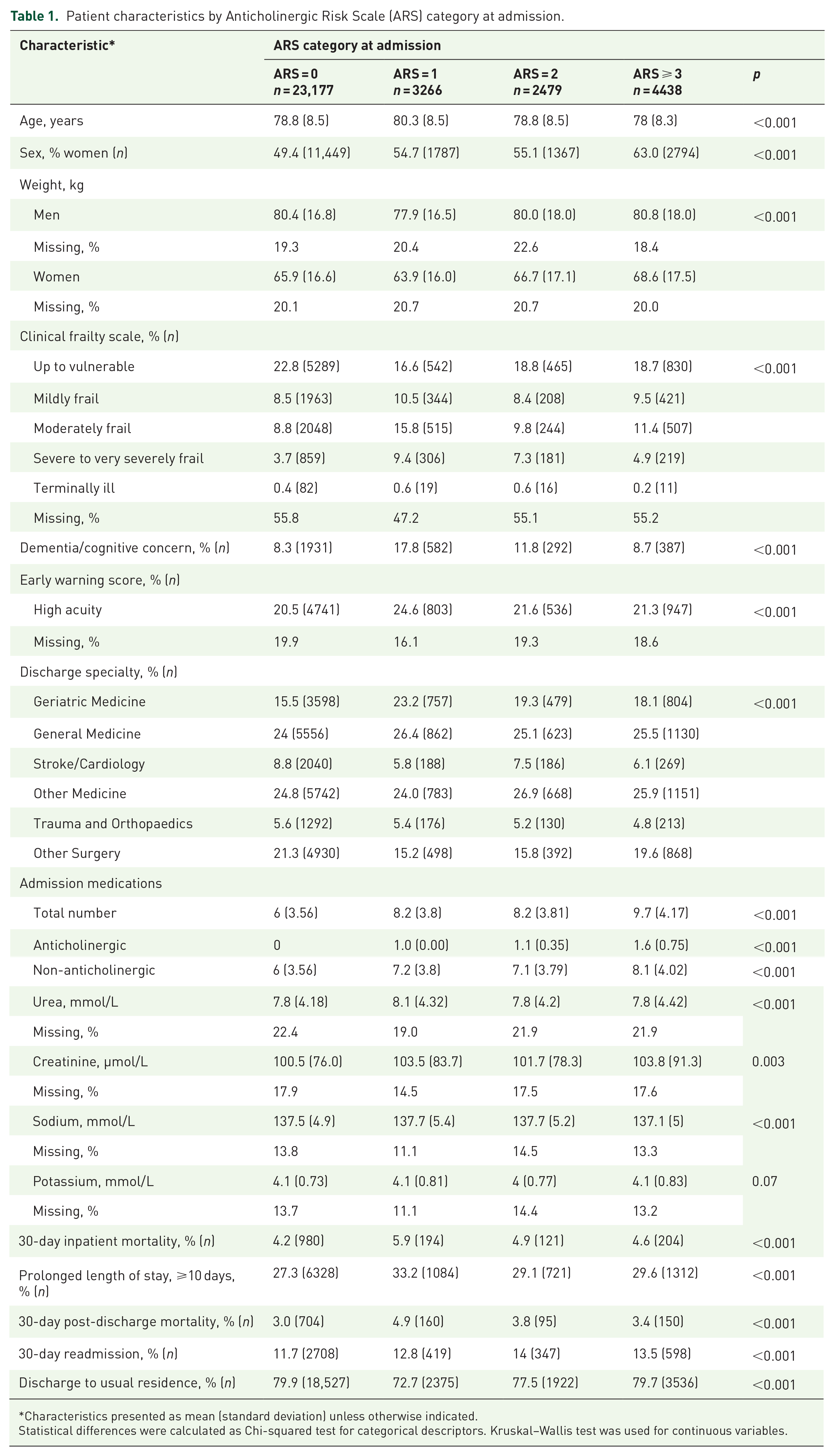
Characteristics presented as mean (standard deviation) unless otherwise indicated.
Statistical differences were calculated as Chi-squared test for categorical descriptors. Kruskal–Wallis test was used for continuous variables.
Associations between admission ARS scores and hospital outcomes were further explored using logistic regression (Table 2). Strong associations were observed between ARS = 1 and higher odds of inpatient mortality, post-discharge mortality and lower odds of discharge to usual residence compared with those taking no anticholinergics. These associations were also seen in those with an ARS score of 2 and ⩾3 but were weaker and attenuated with co-variable adjustment, especially in the highest ARS exposure category. Patients with higher ARS scores also had higher odds of 30-day post-discharge readmission, and these associations did strengthen across higher ARS exposure categories. No strong associations with prolonged hospital stay were observed.
Logistic regression analyses evaluating associations between ARS category at admission (reference category: ARS = 0) and hospital outcomes.

Model A, age, sex; Model B, A + number of non-anticholinergic drugs at admission; Model C, B + discharge specialty; Model D, C + acuity; Model E, D + known dementia or cognitive concern.
ARS, Anticholinergic Risk Scale; CI, confidence interval; OR, odds ratio.
Change in ARS from admission to discharge
Figure 1 describes mean admission and discharge ARS scores by discharging specialty. The mean admission ARS score was highest in patients later discharged by Geriatric Medicine and lowest in those discharged by Cardiology or Stroke Medicine and Surgical specialties. No specialty group showed an increase in mean ARS score from admission to discharge but there was a statistically significant reduction in mean ARS from admission to discharge in all specialties (results from Wilcoxon test adjusted by Bonferroni correction are shown in Figure 1). These differences varied significantly between specialties (p < 0.001) and the largest absolute and relative reductions in mean ARS scores were seen in patients discharged by Geriatric Medicine (Δ0.23, 27.7%) and Trauma and Orthopaedics (Δ0.16, 24.2%) (Figure 1).

Boxplot of mean ARS at admission (black) and discharge (grey) by discharge specialty.
Figure 2 provides the distribution of patients across ARS change categories according to discharge specialty. Patients discharged by Geriatric Medicine, General Medicine or Other Medical Specialties were twice as likely to have their ARS score decreased as increased during their admission episode and patients discharged by Trauma and Orthopaedics were three times as likely to have their ARS score decreased as increased.

Bar plot of patients by ARS change category for each discharge specialty.
The characteristics of patients by change in ARS score category are described in detail in Table 1 of the Supplemental information online. Of note, 11.3% (n = 594) and 12.1% (n = 224) of patients whose ARS score stayed the same or increased, respectively, had dementia or a concern about their cognition. Additionally, all patients with some exposure to anticholinergics, whether their ARS score had remained the same, increased or decreased during the admission, had higher post-discharge mortality (Table 1 in Supplemental information). Exploration of associations between ARS change categories and patient outcomes using multivariable logistic regression confirmed that all ARS score change categories had higher odds of 30-day post-discharge mortality compared with those taking no anticholinergics on admission or discharge, with strongest associations when ARS score increased (Table 3).
Logistic regression analyses evaluating associations between change in ARS from admission to discharge (reference category: admission and discharge ARS = 0) and hospital outcomes.

Model A, age, sex; Model B, A + number of non-anticholinergic drugs at admission; Model C, B + discharge specialty; Model D, C + acuity; Model E, D + known dementia or cognitive concern.
ARS, Anticholinergic Risk Scale; CI, confidence interval; OR, odds ratio.
Patients experiencing either an increase or a decrease in ARS score from admission to discharge were more likely to have a prolonged hospital stay and odds of hospital re-admission were higher in patients whose ARS score decreased. However, no other associations with hospital readmission were observed after multivariable adjustment (Table 3).
Discussion
This large-scale retrospective analysis of prescribing practices is the first, to our knowledge, to examine change in anticholinergic burden from admission to discharge in a large inpatient population and explore relationships with important objective outcomes. Consistent with previous reports, around one-third of all older patients were admitted to hospital with a prescription for at least one anticholinergic medication. 15 More patients experienced a decrease in their ARS score from admission to discharge than an increase, but there was variation between specialties and a significant number of patients with cognitive impairment were still prescribed anticholinergics on discharge. After accounting for important confounders (Model E), exposure to anticholinergic medication was associated with higher inpatient and post-discharge mortality, higher readmission to hospital and lower odds of being discharged back to a patient’s usual residence. However, associations were sometimes inconsistent across exposure categories.
The observed pattern of lower ARS scores on discharge than on admission suggests that clinical teams are implementing clinical guidelines regarding cautious anticholinergic prescribing in older adults. The decrease in ARS was most pronounced in patients discharged by Geriatric Medicine and Trauma and Orthopaedics. In our centre, the Trauma and Orthopaedics service is supported by dedicated ortho-geriatricians, who specialise in the multidisciplinary care of older adults admitted as an emergency with fractures. Thus, the decrease in ARS from admission to discharge observed in these specialties may be due to these clinical teams considering a holistic review of medicines and deprescribing as a core component of their role, rather than focusing on a discrete body system and therapeutic area. However, other specialties will also have a proportion of patients who may benefit from a holistic review and reduction of anticholinergics; 19 our results suggest this happens infrequently. We also observed that a significant proportion of patients prescribed anticholinergics, including patients who experienced an increase in ARS from admission to discharge, had dementia or a concern about their cognition. In some patients, anticholinergics may be prescribed appropriately, for example, patients with delirium sometimes require treatment with antipsychotic medications. However, even in these patient groups anticholinergic burden can be secondary to polypharmacy or poor prescribing practices and has the potential to be reduced.22,23 It is striking that in our patient population it was the specialties who usually care for the highest proportions of patients with dementia and delirium where ARS scores reduced the most from admission to discharge.
The association between anticholinergic burden and mortality in both community and hospital settings is controversial. 17 We observed strong associations between those with an ARS score of 1 and both inpatient and post-discharge mortality. We also observed associations between all ARS change categories and post-discharge mortality, compared with patients with no anticholinergic medication exposure. These findings suggest that there may be an increased mortality risk associated with anticholinergics. However, the lack of a consistent association across all admission ARS score categories raises concerns, especially given the large numbers in each exposure category.
There are many different tools to measure anticholinergic burden,24,25 which vary in medications included and the potency of anticholinergic effect assigned to each medication, and it is possible that not all are equally effective. We used the ARS because it has been well validated in community and hospital populations and only considers medications with known in vivo anticholinergic activity.20,25 It is possible other scoring methods would have given different results although generally different scales have been shown to perform similarly in predicting outcomes. 26 A further consideration is that our assessment of anticholinergic burden did not take into account the dose prescribed. This may be important and has been underexplored in terms of its influence, 27 although some recent studies have utilised methods incorporating dose adjustments. 28 For example, in our cohort a frequently prescribed anticholinergic medication included in the ARS is amitriptyline. 20 This scores three points and places patients in the highest exposure category. However, many older adults are prescribed very low doses of this drug for symptoms such as difficulty sleeping and including these patients in the highest ARS category could ‘dilute’ associations.
It is also possible that our use of inpatient mortality or death in the first 30 days after discharge did not allow sufficient follow-up time. Previous observational work has associated higher anticholinergic medication exposure with mortality and specific disease endpoints such as cardiovascular events. 29 However, in these studies participants are followed up over many years.
Associations with other hospital outcomes were mixed. For example, a dose–response association between higher admission ARS score and higher odds of readmission to our centre was observed but, amongst ARS change categories, only a reduction in ARS from admission to discharge showed this trend. These mixed findings could reflect the complexity of prescribing in older patients who often have frailty, polypharmacy and multimorbidity. Deprescribing is always a balance of risks and benefits and in some patients, the underlying condition cannot be managed well without specific pharmacological intervention. Given the scale of our study, it was not possible to differentiate between appropriate and inappropriate prescribing and deprescribing. Therefore, the inconsistent trends observed across some of our analyses could be explained by the fact that our measurement of anticholinergic burden included all drugs with anticholinergic properties, without considering appropriateness. However, our findings also mirror the mixed results from other studies20,24,30,31 and explanations such as residual confounding or bias from measurement error in the exposure have to be considered.
We were limited to information recorded in the EHR as part of routine clinical care. Therefore, missing data was greater than in traditional research studies and we cannot exclude confounding. For example, we did not have data on long term medical conditions and we do not routinely measure frailty in patients <75 years old. Additionally, given the unique focus of our work on the description of anticholinergic prescribing patterns from admission to discharge in a large inpatient cohort, it was important to explore associations between both admission ARS score and ARS change categories and clinical outcomes. Whilst these analyses provide further evidence of links between anticholinergic exposure and clinical outcomes, other studies are needed to fully untangle relationships between this complex exposure and health. For example, studies examining anticholinergic burden at discharge and health endpoints will be important to further explore the potential benefits of deprescribing in inpatient settings, and future work may also consider appropriate versus inappropriate anticholinergic prescribing. Small scale trials have shown that it is possible to operationalise interventions to specifically reduce inappropriate anticholinergic burden in clinical settings but future work is needed to establish whether such reduction translates to clinical benefit. 16
We should additionally consider that 30-day post-discharge mortality and hospital readmission were perhaps less robust outcome measures because we did not have data on admissions to other hospitals and not all deaths outside of the hospital are reported to our centre. However, such numbers are likely to be small and unlikely to change the direction of associations. The single centre design also limits the generalisability of our results, particularly with regard to deprescribing patterns.
Accepting these limitations, our results provide important, relevant and novel insights with regard to the potential for anticholinergic burden reduction interventions in acute settings, across wide ranging specialties, as well as the potential benefits associated with this approach. We found that inpatients across all specialties were commonly prescribed anticholinergics but there was variation in reduction of anticholinergic burden from admission to discharge by specialty group. This variation supports the need for further work on the development and implementation of deprescribing interventions that can be applied to non-specialist wards. Additionally, in agreement with other work, although exposure to anticholinergics was associated with higher mortality and other negative patient outcomes, associations were sometimes inconsistent. Therefore, it is perhaps time to focus on how clinical translation of this important topic can be achieved. Clinicians are unlikely to change practice unless the challenges and gaps in current knowledge are resolved, yet anticholinergic medication exposure is a potential health risk factor that could be readily modified. Therefore, further work should consider the need for randomised clinical trials to evaluate the potential benefits of anticholinergic deprescribing and robustly address issues such as confounding and appropriate versus inappropriate anticholinergic exposure.
Supplemental Material
sj-pdf-1-taw-10.1177_20420986211012592 – Supplemental material for Anticholinergic burden in older adult inpatients: patterns from admission to discharge and associations with hospital outcomes
Supplemental material, sj-pdf-1-taw-10.1177_20420986211012592 for Anticholinergic burden in older adult inpatients: patterns from admission to discharge and associations with hospital outcomes by Maria Herrero-Zazo, Rachel Berry, Emma Bines, Debi Bhattacharya, Phyo K. Myint and Victoria L. Keevil in Therapeutic Advances in Drug Safety
Footnotes
Acknowledgements
The authors would like to thank the clinical informatics team at Cambridge University’s Hospital for their help in data extraction from the EHR.
Author contributions
All authors listed were responsible for aspects of study design, data collection and analysis and writing of manuscript and meet criteria for authorship. EB, RB, DB, PKM and VLK conceived and initiated the project. MHZ performed the data analysis with additional input from VLK. MHZ and VLK wrote the first draft of the manuscript. All authors contributed to interpreting the data and writing the final paper. All authors read and approved the final manuscript.
Ethics approval
This service evaluation project received no specific funding and was approved by the hospital’s Safety and Quality Support Department (Project register number 6457). The local Research and Development Department confirmed no formal review by a Research Ethics Committee was required.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: VLK is funded by a Medical Research Council (MRC)/National Institute for Health Research (NIHR) Clinical Academic Research Partnership grant (CARP; grant code: MR/T023902/1). MHZ acknowledges support from the NIHR Cambridge Biomedical Research Centre (BRC-1215-20014). The views expressed are those of the authors and not necessarily those of the NIHR or the Department of Health and Social Care or the MRC.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.