
Abstract
Background:
Polypharmacy is a growing phenomenon among elderly individuals. However, there is little information about the frequency of polypharmacy among the elderly population treated in emergency departments (EDs) and its prognostic effect. This study aims to determine the prevalence and short-term prognostic effect of polypharmacy in elderly patients treated in EDs.
Methods:
A retrospective analysis of the Emergency Department Elderly in Needs (EDEN) project’s cohort was performed. This registry included all elderly patients who attended 52 Spanish EDs for any condition. Mild and severe polypharmacy was defined as the use of 5–9 drugs and ⩾10 drugs, respectively. The assessed outcomes were ED revisits, hospital readmissions, and mortality 30 days after discharge. Crude and adjusted logistic regression analyses, including the patient’s comorbidities, were performed.
Results:
A total of 25,557 patients were evaluated [mean age: 78 (IQR: 71–84) years]; 10,534 (41.2%) and 5678 (22.2%) patients presented with mild and severe polypharmacy, respectively. In the adjusted analysis, mild polypharmacy and severe polypharmacy were associated with an increase in ED revisits [odds ratio (OR) 1.13 (95% confidence interval (CI): 1.04–1.23) and 1.38 (95% CI: 1.24–1.51)] and hospital readmissions [OR 1.18 (95% CI: 1.04–1.35) and 1.36 (95% CI: 1.16–1.60)], respectively, compared to non-polypharmacy. Mild and severe polypharmacy were not associated with increased 30-day mortality [OR 1.05 (95% CI: 0.89–2.26) and OR 0.89 (95% CI: 0.72–1.12)], respectively.
Conclusion:
Polypharmacy was common among the elderly treated in EDs and associated with increased risks of ED revisits and hospital readmissions ⩽30 days but not with an increased risk of 30-day mortality. Patients with polypharmacy had a higher risk of ED revisits and hospital readmissions ⩽30 days after discharge.
Plain language summary
Management elderly patients with polypharmacy is becoming a major challenge to the emergency services. The progressive aging of the population is producing a progressive increase in the number of patients treated with multiple comorbidities and chronic medications. It’s well known that polypharmacy is associated with an increase in hospital admissions and health care system costs. However, the impact of polypharmacy over the risk of new visits to the emergency rooms is not well defined. Understanding the impact of polypharmacy on the frequency of new visits to the emergency room and on patient mortality is the first step to establish prevention measures for new visits, proposing improvements in chronic treatment at discharge. This study aimed to determine the prevalence and effect on short-term prognosis of polypharmacy in elderly patients treated in Emergency departments.
The authors used a retrospective multipurpose registry in 52 hospitals in Spain. This study includes 25,557 patients with a mean age of 78 years. On admission, the median number of drugs was 6 (IQR: 3–9), with 10,534 (41.2%) patients taking 5–9 drugs and 5,678 (22.2%) taking ⩾10 drugs. In these patients comorbidities were associated with an increase in the number of drugs. In the patients with severe polypharmacy (⩾10 drugs), diuretics were the most frequently drugs prescribed, followed by antihypertensives and statins. The results obtained indicate that polypharmacy is a frequent phenomenon among the elderly population treated in Emergency departments, being antihypertensives the most frequently used drugs in this population. Those patients who takes ⩾10 drugs have a higher risk of new visits to the emergency room and hospital readmissions in short term period.
Introduction
During the last few decades, emergency departments (EDs) have treated an increasing number of elderly individuals, including an increasing number of patients with multiple chronic pathologies and, consequently, in the number of polymedicated patients.1,2 The number of elderly patients visiting the ED is expected to rise in the next decades. 3
Pharmacological treatment has managed to make a large part of medical pathologies chronic, increasing life expectancy in the population. Nonetheless, the benefits of treatment should outweigh the risks in each patient, particularly in elderly patients with frailty, chronic comorbidity, or those near the end of life.
Polypharmacy is associated with an increase in hospital admissions, ED visits, and health care system costs.3,4 In fact, drug adverse events have been related to a high number of ED visits, especially in the elderly population.5,6 Several studies have found an association between high therapeutic complexity combined with a lack of adherence to treatment and an increase in adverse effects.7–9 Elderly patients are at higher risk of experiencing drug-related adverse events because of their reduced functional reserve and decreased renal and hepatic clearance, with polypharmacy contributing to their frailty.10–13
ED visits can often be for serious and life-threatening conditions that can be complicated by hemodynamic instability, dehydration or acute kidney, and/or hepatic injury. Polypharmacy can contribute to these factors, affecting an individual’s health outcomes. This challenge in ED care also presents an opportunity to reconcile medications, screen for potentially inappropriate medication and drug interactions, avoid the pitfalls of inappropriate medication use, and even deprescribe unnecessary drugs when indicated.
Despite the well-known relationship between polypharmacy and healthcare resource utilization, the effect of polypharmacy on short-term outcomes in elderly patients treated at EDs has not been well established. This study aimed to determine the prevalence and effect on the short-term prognosis of polypharmacy in elderly patients treated in EDs.
Materials and methods
SIESTA network and EDEN project
The main purpose of the Spanish Investigators in Emergency Situations TeAm (SIESTA) research network created in 2020 is to address multidisciplinary research challenges in real clinical practice from the multicentric perspective of a broad representation of Spanish EDs. Although the network has a stable coordinating core membership, participants from individual EDs can be included in new research challenges for which they have an interest and availability. 14
The Emergency Department and Elderly Needs (EDEN) challenge was initiated by the SIESTA network, with a primary objective of increasing knowledge about the sociodemographic, organizational, baseline, clinical care, and evolutionary aspects of the ⩾65-year-old population who visit Spanish EDs for consultation and treatment, if needed.
To this end, a retrospective multipurpose registry was designed. The EDEN cohort included all patients who consulted in 1 of 52 Spanish EDs (17% of EDs of the Spanish public network covering approximately 25% of the Spanish population) between 1st and 7th April 2019 (7 days). There were no exclusion criteria, and the EDs included all patients seen during the study period regardless of the reason for their consultation. Sociodemographic data, comorbidities, functionality, cognitive ability, and treatments at baseline, among other variables, were recorded for each patient by consulting the patient’s medical records. Chronic diseases were obtained from the coded electronic records of the patient’s medical history. Extensive details of the EDEN registry have been previously published in detail. 15 In brief, EDEN included the variables of sociodemographic data, comorbidities, functional status, basal treatments, clinical aspects, consumption of diagnostic, and therapeutic resources, final diagnosis in the ED, patient disposition after ED care, hospitalization (if any), and follow-up after discharge (either directly from the ED or after hospitalization). Follow-up was achieved by consulting each patient’s medical history.
EDEN-32 study design
The EDEN-32 study was specifically designed to evaluate the effect of mild polypharmacy (5–9 drugs) and severe polypharmacy (⩾10 drugs), 2 which is higher in the >80-year-old population,16,17 on short-term prognosis. For this purpose, the number of drugs prescribed in the electronic medical prescription accessible through the shared electronic health records system at ED admission was considered. Three outcomes (dependent variables) were analyzed: ED revisits, hospital readmissions, and mortality 30 days after ED discharge. We included all of the patients in the EDEN registry for whom sex, age, and number of drugs prescribed in their primary care medication plan were available. For hospitalized patients, the number of days until the ED revisit or hospital readmission was counted from the day of hospital discharge. All information was collected retrospectively, based on the information obtained in the databases of the participating centers. Both new emergency visits and hospital readmissions were considered those that occurred in the center where the patient was identified.
As independent variables, we recorded the following baseline patient characteristics: age >80 years, sex, hypertension, ischemic cardiomyopathy, chronic heart failure, chronic obstructive pulmonary disease, moderate–severe chronic renal failure, hepatopathy, non-insulin-dependent diabetes, insulin-dependent diabetes, dementia, onco-hematologic disease, mild and severe polypharmacy, comorbidities (assessed by the Charlson Comorbidity Index, CCI), and dependency level (assessed by the Barthel Index, BI). The calculation of these scores was based on data from the emergency care report and a review of the clinical documents in the patient’s electronic medical records.
Statistical analysis
Quantitative variables are expressed as the median and interquartile range (IQR) and categorical variables as the number of cases and percentages. For comparisons, we performed Student’s t-test, chi-square test, or analysis of variance. We evaluated the effect of polypharmacy, on ED revisits, hospital readmissions, and mortality 30 days after discharge.
Crude and logistically adjusted analyses that incorporated age, sex, comorbidities assessed by the CCI, and baseline status assessed by the BI were performed, and the comorbidities with a value of p < 0.05 in a previous univariate analysis were selected. For all comparisons, statistical significance was accepted for p values <0.05 odds ratio (OR) if the 95% confidence interval (CI) of the risk estimations excluded the value of 1. The Stata v.15.0 (Stata Corp., College Station, TX, USA) statistics program was used for the description of variables and statistical analysis of the results.
Ethics
The EDEN project was approved by the Clinical Research Ethics Committee of the Hospital Clínico San Carlos de Madrid (protocol HCSC/22/005-E). Since the EDEN project had a retrospective and non-interventional design, patient informed consent was waived. This study was conducted in strict compliance with the principles of the Declaration of Helsinki.
Results
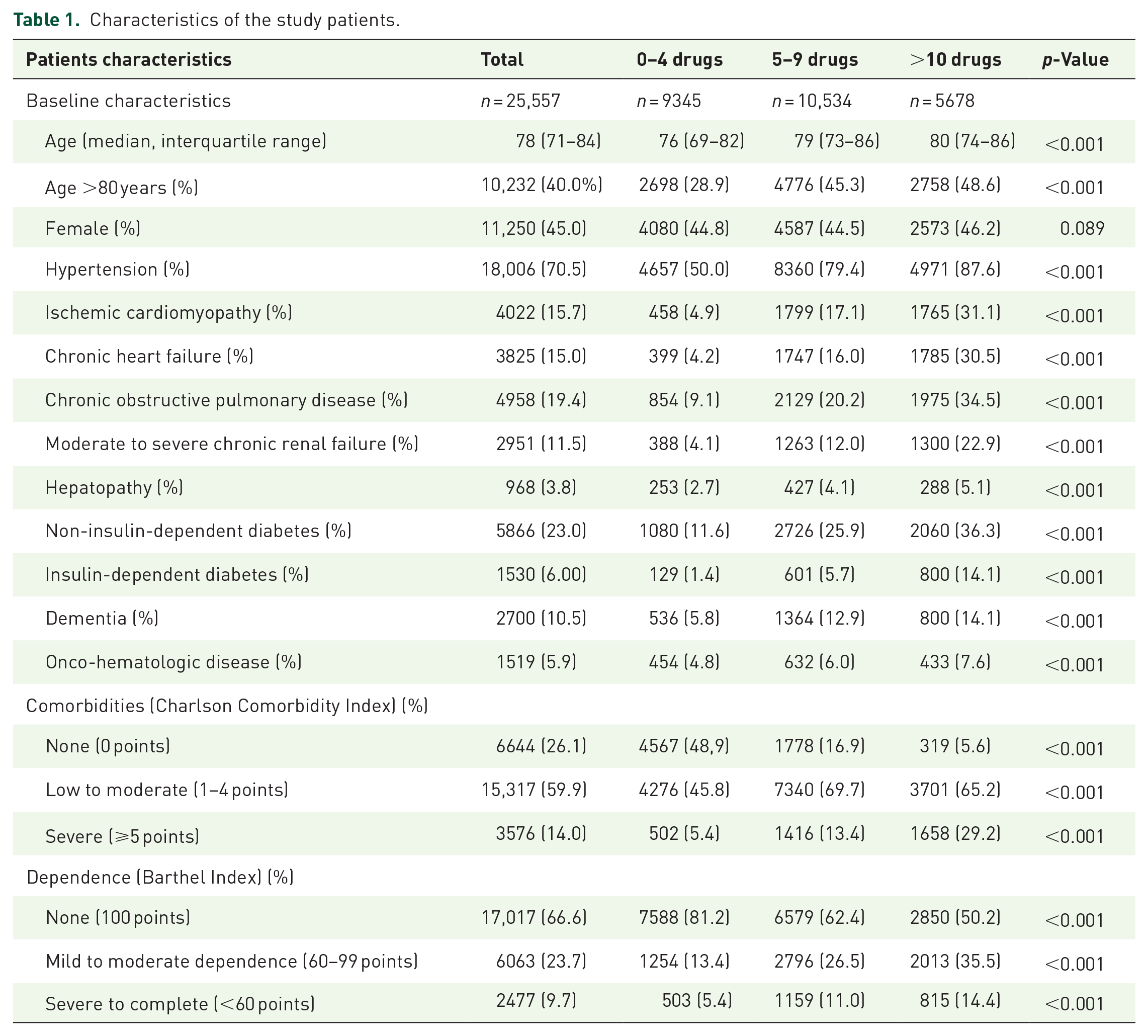
A total of 25,557 patients with a mean age of 78 (IQR: 71–86) years were evaluated. The characteristics of the population included in the study are presented in Table 1. Comorbidities were associated with an increase in the number of drugs. On admission, the median number of drugs was 6 (IQR: 3–9), with 10,534 (41.2%) patients taking 5–9 drugs and 5678 (22.2%) taking ⩾10 drugs (Figure 1). Renin–angiotensin–aldosterone system inhibitors (RAASi) were the most frequent drugs prescribed and taken by 53.3% of patients, followed by statins (44.5%) and diuretics (39.3%). In the patients with severe polypharmacy, diuretics (67.9%) were the most frequent drugs prescribed, followed by RAASi (67.4%) and statins (66.7%) (Figure 2).
Characteristics of the study patients.

Flow chart for patient inclusion in the EDEN-32 study.
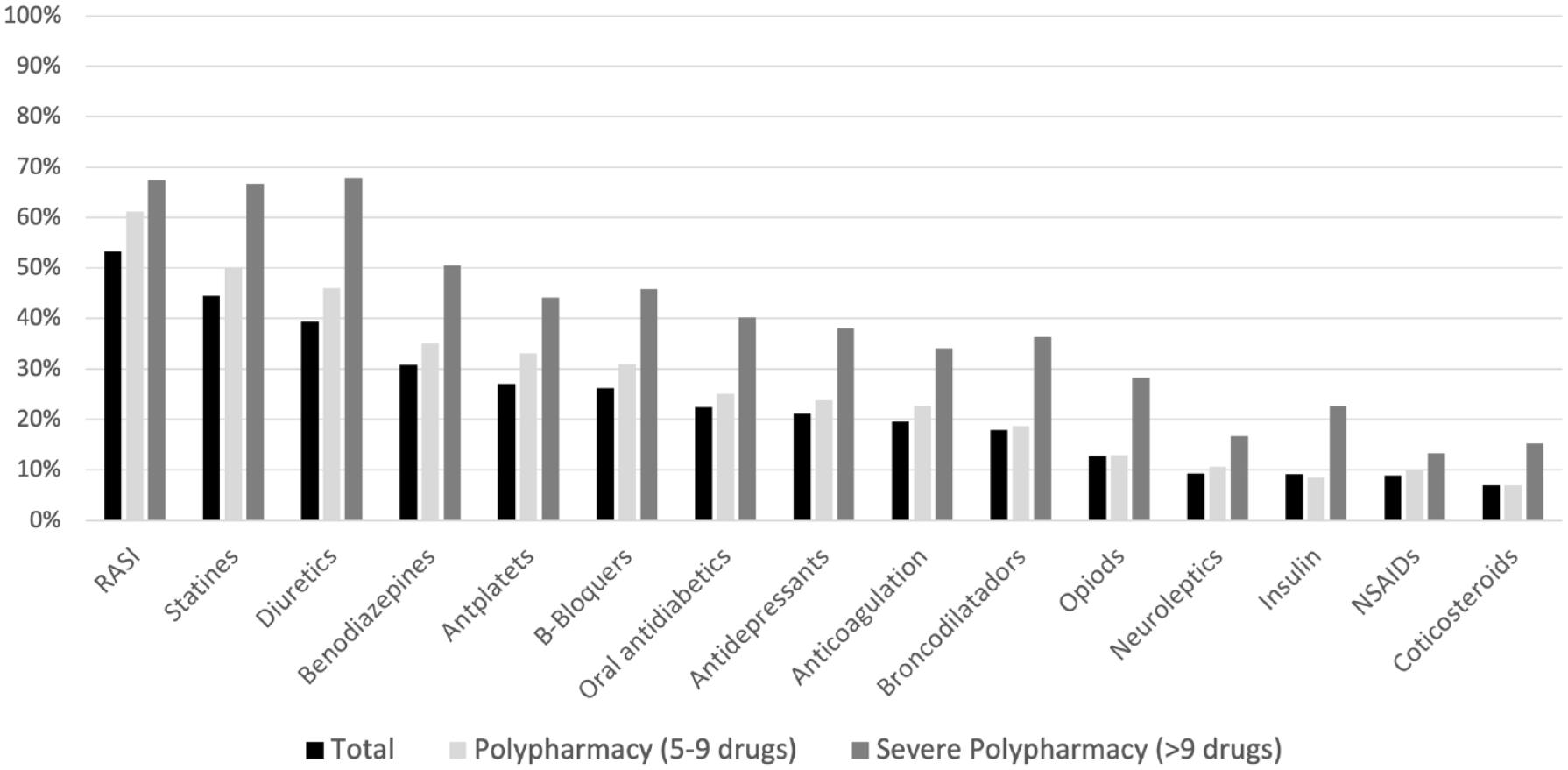
Therapeutic groups included in the usual treatment of the patients analyzed.
Revisits to the ED and hospital readmission
The number of patients who revisited the ED within 30 days of discharge was 4899 (19.2%). The baseline patients’ characteristics according to revisits and hospitalizations are presented in Table 2. In the unadjusted analysis, the OR for 30-day ED revisits ranged from 1.28 (1.19–1.38) in patients with mild polypharmacy to 1.69 (1.57–1.83) in patients with severe polypharmacy. After adjustment for comorbidities, this association persisted for both mild polypharmacy [OR: 1.13 (1.04–1.23)] and severe polypharmacy [OR: 1.38 (1.24–1.51)].
Baseline patient characteristics and polypharmacy according to outcomes.
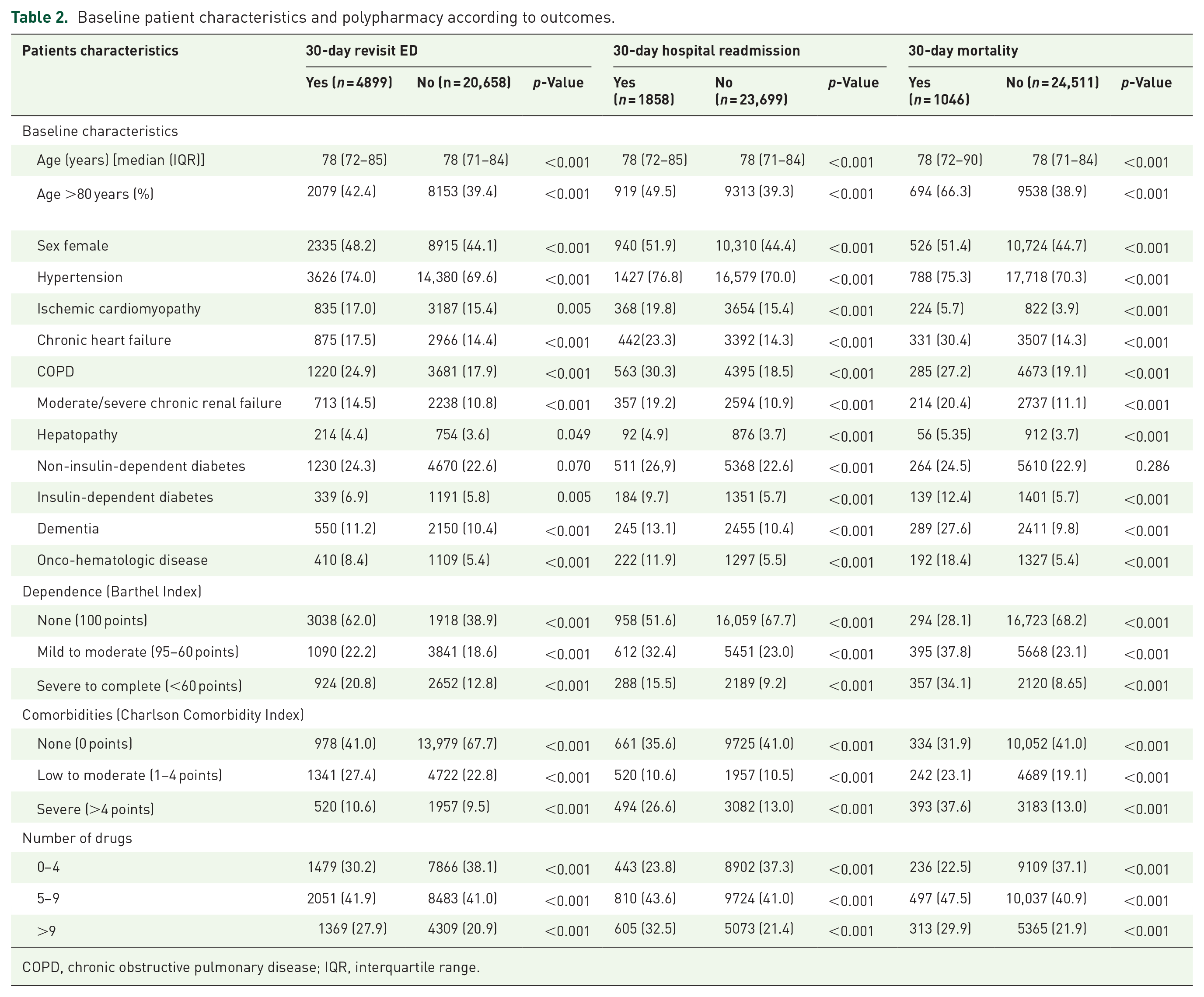
COPD, chronic obstructive pulmonary disease; IQR, interquartile range.
The number of patients who were hospitalized ⩽30 days after ED discharge was 1858 (7.3%). In the unadjusted analysis, mild polypharmacy [OR: 1.67 (1.48–1.88)] and severe polypharmacy [OR: 2.40 (2.10–2.72)] were associated with hospital readmission compared to non-polypharmacy. After adjustment for comorbidities, this association persisted (Table 3).
Results of the multivariate analysis.
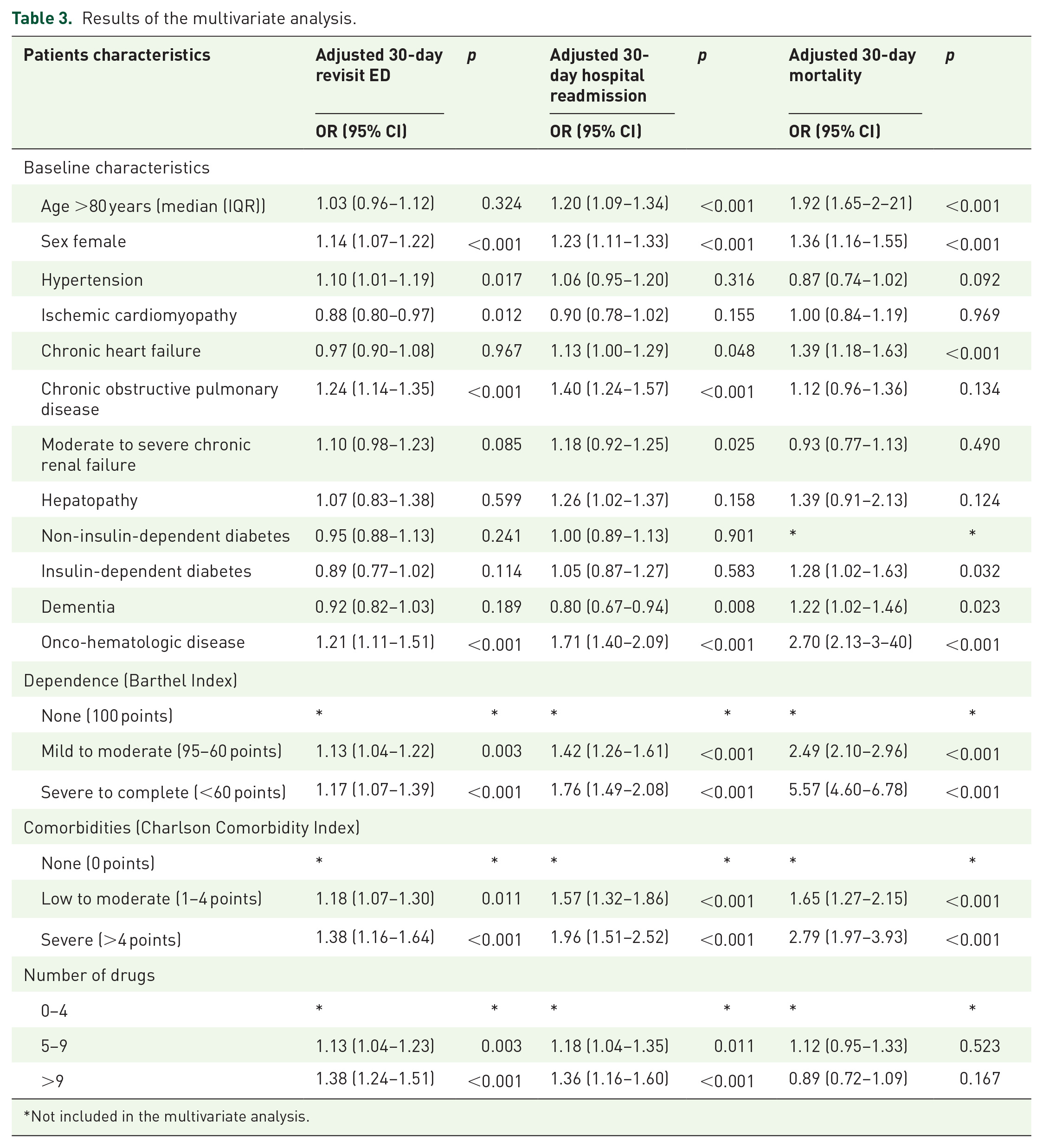
Not included in the multivariate analysis.
Mortality
The number of patients who died ⩽30 days was 1046 (4.1%). In the unadjusted analysis, the OR for 30-day mortality ranged from 1.91 (95% CI: 1.63–2.23) in patients with mild polypharmacy to 2.25 (1.89–2.67) in patients with severe polypharmacy. In the adjusted analysis, mild polypharmacy [OR: 1.12 (0.95–1.33)] and severe polypharmacy [OR: 0.89 (0.72–1.09)] were not associated with higher 30-day mortality (Figure 3).

Associations between polypharmacy and 30-day mortality, 30-day emergency department revisits, and 30-day hospital readmissions.
Discussion
The study results showed that mild polypharmacy and severe polypharmacy were common in elderly patients who visited the ED and were associated with a higher risk of revisits to ED and hospitalization 30 days after discharge. However, no association was found between polypharmacy and 30-day mortality.
The high percentage of patients with polypharmacy observed in the EDEN-32 study (63.4%) study is comparable to the percentages found in other studies in the field of emergency care.7,18–20 It is noteworthy that, as in the previous studies mentioned, drugs for the prevention of cardiovascular events, including RAASi, statins, and diuretics, have been the most frequently prescribed in this population. Diuretics were the most common medications prescribed among the severe polypharmacy patients. These drugs have been included as one of the most prevalent drugs associated with preventable adverse events.21,22 On the other hand, the frequency of benzodiazepine prescriptions was nearly 30% in the study population, with the percentage of patients taking opioids and neuroleptics >10%. The association between these drugs and the occurrence of adverse events in the elderly population is well known, which is why only short-term use is recommended. 23 Progressive discontinuation of these drugs should be proposed at ED discharge, especially in patients at high risk of falls.
The main study finding is that after adjusting for comorbidity and functional status, polypharmacy was associated with the risk of ED revisits and hospital readmission, being higher in those patients with severe polypharmacy. These findings were consistent with those obtained by other authors,24,25 highlighting the negative effects of polypharmacy in the elderly population. Several authors have reported associations between polypharmacy and adverse events in elderly patients admitted to the ED. 26 The presence of multiple diseases, and therefore polypharmacy, increases the risk of drug non-compliance, drug–drug interactions, and adverse drug reactions (including readmission, falls, and mortality).27–29 A matter of debate is whether worse outcomes are related to patients’ comorbidities or polypharmacy. Our results demonstrated that, even when considering comorbidities, polypharmacy remained a risk factor for increased revisits to the ED. Therefore, given that elderly patients are considered at high risk and that the greatest risk of adverse events occurs in the first days or months after a new prescription drug has been started, 30 rapid simplification of chronic treatments for patients who visit the ED may be necessary. In fact, several experiences related to treatment optimization at discharge in this group of patients have presented positive results, although the results in terms of clinical variables and quality of life remain controversial.31,32 Avoiding cascade prescription phenomena to alleviate adverse effects of other drugs, as well as adapting chronic treatment to the new clinical situation of a patient after admission, should be part of the strategies to improve the quality of life for patients with multiple diseases. 33 Published guidelines to facilitate the de-prescription process advocate considering the patient’s opinions and an effective communication system with physicians responsible for patients outside the hospital setting as key elements in achieving effective treatment simplification.34,35
Our study did not find an association between polypharmacy and 30-day mortality. van Dam et al. 18 reported an increase in the risk of 90-day mortality but did not find an association with the risk of readmission. Other authors also have reported this association between mortality in patients with polypharmacy after ED discharge.7,36 The short analysis period of our study may explain why our data did not support this association. Sustained polypharmacy is likely an additional risk factor contributing to the increased risk of adverse effects.
To date, there is a lack of solid evidence to show that targeting polypharmacy in the ED improves patient outcomes. Deprescribing medications in the ED setting presents challenges given the short-term nature of contact between the patient and ED clinicians. However, a close medication review seems reasonable in frailty patients near the end of life, especially in those patients attended by drug-related problems. Prescribers should consider the presence of polypharmacy when prescribing new drugs at discharge. Future studies should investigate the effectiveness and applicability of the different tools that exist when addressing polypharmacy in patient’s new ED visits, readmissions, and mortality.
Limitations
This study had some limitations that should be considered when interpreting the results. The EDs included in the EDEN registry were not chosen at random and had expressed their interest in participating. However, the broad territorial representation (14 of the 17 autonomous communities were represented) means that the selection bias was probably small. The major study strengths include the large sample size and well-characterized study population. Second, this was a secondary analysis of a multipurpose cohort, which means that the associations identified may have been influenced by factors not included in the cohort design. Therefore, the findings should be considered to be useful for generating hypotheses and should be confirmed by studies specifically designed for this purpose and/or to test a hypothesis. Third, it should be noted that our study only assessed the prescription of drugs at ED admission, without considering any subsequent modifications or non-prescription medicines usage. ED visits associated with drug-related problems were also not recorded. Future studies are needed to evaluate the effect of reducing medications from the ED on the frequency of new consultations in the elderly population. Moreover, the patient’s adherence to the medication plan prescribed was not evaluated. It is well known that patients with polypharmacy frequently present adherence problems and voluntary suspensions of some of their drugs prescribed.3–5 The origin and the presence of caregivers were not evaluated either. These variables can affect adequate administration of the medication and therefore, the possible negative events associated with non-adherence or overtreatment. However, the results of our study allow us to quickly identify those patients with a potential risk of new visits to the emergency room based on their pharmacotherapy. Fourth, we evaluated ED episodes, not individual patients; therefore, multiple presentations of the same patient were included, but this only involved a few patients since the evaluation period was only 1 week, so the probability of such patients having a significant effect on the study results was very low.
Conclusion and relevance
Polypharmacy was found to be a frequent phenomenon among the elderly population treated in EDs in our country, with antihypertensives, and statins being the most frequently drugs prescribed in this population. Patients taking >10 drugs had a higher risk of ED revisits and hospital readmissions ⩽30 days after discharge but mild to severe polypharmacy did not have a significant effect on short-term mortality in this study.
Footnotes
Acknowledgements
None.
Declarations
Local investigators
Hospital Clínico San Carlos, Madrid: Juan González del Castillo, Cesáreo Fernández, Jorge García Lamberechts, Paula Queizán García, Andrea B. Bravo Periago, Blanca Andrea Gallardo Sánchez, Alejandro Melcon Villalibre, Sara Vargas Lobé, Laura Fernández García. Hospital Universitario Infanta Cristina, Parla: Beatriz Honrado Galán, Sandra Moreno Ruíz, Sara Carbajal Tinoco. Hospital Santa Tecla, Tarragona: Lidia Cuevas Jiménez, Osvaldo Jorge Troiano Ungerer. Hospital Universitario de Canarias, Tenerife: Guillermo Burillo Putz, Aarati Vaswani-Bulchand, Patricia Eiroa-Hernández. Hospital Norte Tenerife: Montserrat Rodríguez-Cabrera. Hospital General Universitario Reina Sofia, Murcia: Pascual Piñera Salmerón, M. Encarnación Sánchez Cánovas, Pedro Alarcón Martínez, Mabel Coromoto Suárez Pineda, Manuel E. Castillo Vargas, María del Carmen Molina Morazo. Hospital Universitario del Henares, Madrid: Raquel Cenjor Martín, Noha El-Haddad Boufares, Raquel Barrós González. Hospital Clinic, Barcelona: Sonia Jiménez, Sira Aguiló Mir, Francesc Xavier Alemany González, María Florencia Poblete Palacios, Claudia Lorena Amarilla Molinas, Ivet Gina Osorio Quispe, Sandra Cuerpo Cardeñosa. Hospital General Universitario de Elche: Matilde González Tejera, Ana Puche Alcaraz, Cristina Chacón García. Hospital Universitario y Politécnico La Fe, Valencia: Leticia Serrano Lázaro, Javier Millán Soria, Jésica Mansilla Collado, María Bóveda García. Hospital. General Universitario Dr. Balmis, Alicante: Pere Llorens Soriano, Adriana Gil Rodrigo, Begoña Espinosa Fernández, Mónica Veguillas Benito, Sergio Guzmán Martínez, Gema Jara Torres, and María Caballero Martínez. Hospital Universitario de Bellvitge, L’Hospitalet de Llobregat, Barcelona: Javier Jacob, Ferran Llopis, Elena Fuentes, Lidia Fuentes, Francisco Chamorro, Lara Guillen, Nieves López. Hospital de la Axarquia de Velez-Malaga: Lucía Zambrano Serrano, Rocío Muñoz Martos, Rocío Lorenzo Álvarez. Hospital Regional de Málaga: Manuel Salido Mota, Valle Toro Gallardo, Antonio Real López, Lucía Ocaña Martínez, Esther Muñoz Soler, Mario Lozano Sánchez, Eva Fragero Blesa. Hospital Santa Barbara, Soria: Fahd Beddar Chaib, Rodrigo Javier Gil Hernández. Hospital Valle Pedroches, Pozoblanco, Cordoba: Jorge Pedraza García, Paula Pedraza Ramírez. Hospital Reina Sofia, Córdoba: F. Javier Montero-Pérez, Carmen Lucena Aguilera, Francisco de Borja Quero Espinosa, Angela Cobos Requena, Esperanza Muñoz Triano, Inmaculada Bajo Fernández, María Calderón Caro, Sierra Bretones Baena. Hospital Universitario Gregorio Marañon, Madrid. Susana Gordo Remartinez, Ana Isabel Castuera Gil, Laura Martín González, Melisa San Julian Romero, Montserrat Jiménez Lucena, María Dolores Pulfer, Juan Fernández Herranz, Marta Rincón Francés, Irene Arnaiz Fernández. Hospital Universitario De Burgos: Amanda Ibisate Cubillas, Monica de Diego Arnaiz, Verónica Castro Jiménez, Lucía González Ferreira, Rocio Hernando González, María Eugenia Rodríguez Palma. Complejo Asistencial Universitario de León: Marta Iglesias Vela, Mónica Santos Orús, Rudiger Carlos Chávez Flores, Alberto Álvarez Madrigal, Albert Carbó Jordá, Enrique González Revuelta, Héctor Lago Gancedo, Miguel Moreno Martín. Hospital Universitario Morales Meseguer, Murcia: Rafael Antonio Pérez-Costa, María Rodríguez Romero, Esperanza Marín Arranz, Ana Barnes Parra, Sara Sánchez Aroca. Hospital Francecs de Borja de Gandía: Alicia Sara Knabe, Andrea Cantos López, Rafael Terol Calvo, Mario Velasco Garcia. Hospital Universitario Severo Ochoa, Leganés: Beatriz Valle Borrego, Esther Álvarez-Rodríguez, Guillermo Villoria Almeida, Rebeca González González, Cristina Iglesias Frax, Teresa Agudo Villa. Hospital Universitario Virgen Arrixaca, Murcia: Eva Quero Motto, Nuria Tomas Garcia, Laura Bernal Martínez, Marina Carrión Fernández, Miguel Parra Morata. Hospital Universitario Lorenzo Guirao, Cieza: Carmen Escudero Sánchez, Belén Morales Franco, Alberto Artieda Larrañaga. Hospital Josep Trueta, Girona: Maria Adroher Muñoz, Ester Soy Ferrer, Eduard Anton Poch Ferrer. Hospital de Mendaro, Gipuzkoa: Jeong-Uh Hong Cho. Hospital Miguel Servet, Zaragoza: Belén Gros Bañeres, Cristina Martín Durán, María Teresa Escolar Martínez-Berganza, Iciar González Salvatierra, Alberto Guillén Bobé, Violeta González Guillén, María Diamanti, Beatriz Casado Ramón. Hospital Comarcal El Escorial, Madrid: Sara Gayoso Martín. Hospital Do Salnes, Villagarcía de Arosa: Goretti Sánchez Sindín. Hospital de Barbanza. Ribeira, A Coruña: Azucena Prieto Zapico, Jésica Pazos González, María Esther Fernández Álvarez, Martina Silva Penas. Hospital del Mar, Barcelona: Isabel Cirera Lorenzo, Patricia Gallardo Vizcaíno, Margarita Puiggali Ballard, M. Carmen Petrus Rivas, Bárbara Gómez y Gómez. Hospital Santa Creu y Sant Pau, Barcelona: Aitor Alquezar-Arbe, Miguel Rizzi, Marta Blázquez Andión, Josep Antonio Montiel Acosta, Isel Borrego Yanes, Adriana Laura Doi Grande, Sergio Herrera Mateo, OlgaTrejo Gutiérrez. Hospital de Vic: Lluís Llauger. Hospital del Nalón, Langreo, Asturias: Lucía Garrido Acosta, Cesar Roza Alonso. Hospital Altagracia, Manzanares: Sara Calle Fernández. Hospital Nuestra Señora del Prado de Talavera de la Reina: Ricardo Juárez González, Mar Sousa, Laura Molina. Hospital Universitario Vinalopó, Elche: Esther Ruescas, María Martínez Juan María José Blanco Hoffman. Hospital de Móstoles: Fátima Fernández Salgado, Eva de las Nieves Rodríguez, Gema Gómez García. Hospital Virgen del Rocio: Amparo Fernández-Simón Almela, Esther Pérez García, Pedro Rivas Del Valle, María Sánchez Moreno, Rafaela Rios Gallardo, Laura Redondo Lora, Ana Gómez Caminero, Claudio Bueno Mariscal. Hospital General Universitario Dr. Peset, Valencia: María Amparo Berenguer Diez, María Ángeles de Juan Gómez, María Luisa López Grima, Rigoberto Jesús del Rio Navarro. Hospital Universitario Son Espases: Bernardino Comas Diaz, Sandra Guiu Martí, Juan Domínguez Casasola, Pere Rull Bertrán. Clinica Universitaria Navarra, Madrid: Nieves López-Laguna, Lourdes Hernández-Castells. Hospital Clínico Universitario, Valencia: José J. Noceda Bermejo, María Teresa Sánchez Moreno, Raquel Benavent Campos, Jacinto García Acosta, Alejandro Cortés Soler. Hospital Álvaro Cunqueiro: María Teresa Maza Vera, Raquel Rodríguez Calveiro, Paz Balado Dacosta, Violeta Delgado Sardina, Emma González Nespereira, Carmen Fernández Domato, Elena Sánchez Fernández-Linares. Hospital Universitario de Salamanca: Ángel García García, Francisco Javier Diego Robledo, Manuel Ángel Palomero Martín, Jesús Ángel Sánchez Serrano. Hospital de Zumarraga: Patxi Ezponda. Hospital Virxe da Xunqueira: Andrea Martínez Lorenzo. Hospital Universitario Los Arcos del Mar Menor, San Javier. Murcia. María Soriano. Hospital Universitario Río Ortega Valladolid: Susana Sánchez Ramón, Inmaculada García Rupérez, Raquel Hernando Fernández, José Ramón Oliva Ramos, Virginia Carbajosa Rodríguez. Hospital Juan Ramón Jiménez: Setefilla Borne Jerez, Asumpta Ruiz Aranda, Maria José Marchena. Hospital Central de Asturias: Eugenia Prieto Piquero, Hugo Mendes Moreira, Isabel Lobo Cortizo, Jennifer Turcios Torres, Lucia Hinojosa Diaz, Jesús Santianes Patiño, Octavio Gutiérrez Alcalá.