
Abstract
Introduction:
The primary aim of this study was to compare the incidence of venous thromboembolism (VTE) among women initiating ospemifene vs other selective estrogen receptor modulator (SERM) therapies for estrogen-deficiency conditions or breast cancer prevention, and vs women with untreated vulvar and vaginal atrophy (VVA). The secondary objective examined numerous additional safety outcomes.
Methods:
This was a retrospective cohort study using the IBM Watson MarketScan claims database. Women receiving ospemifene, another SERM, or with a new diagnosis of VVA with no treatment from 1 May 2013 to 2 October 2018 were followed through the claims for incident adverse outcomes. The primary outcome was the first occurrence of VTE following cohort entry; secondary outcomes included cerebrovascular events and other adverse events potentially associated with SERM use. Cox models compared the risk of VTE between ospemifene and comparators, using a variety of approaches to control for confounding.
Results:
The incidence of VTE during the first continuous treatment episode was 3.39 (95% confidence interval [CI]: 1.55–6.43) events per 1,000 person-years (PY) for ospemifene (N = 8977), 11.30 (95% CI: 8.81–14.28) events per 1,000 PY for comparator SERM (N = 12,621), and 10.92 (95% CI: 10.49–11.37) events per 1,000 PY for untreated VVA (N = 242,488). Cox models indicated no increase in risk of VTE for ospemifene vs other SERMs (hazard ratio [HR]: 0.40, 95% CI: 0.19–0.82), and vs untreated VVA (HR: 0.47, 95% CI: 0.24–0.91).
Conclusion:
This real-world safety analysis found no increase in risk of VTE or other adverse events with use of ospemifene in postmenopausal women.
Plain Language Summary
Keywords
Introduction
Selective estrogen receptor modulators (SERMs) are estrogen receptor agonists or antagonists used for various indications, including treatment of breast cancer, osteoporosis, and menopausal symptoms.1,2 SERMs have been linked to risk of venous thromboembolism (VTE), including deep vein thrombosis (DVT) and pulmonary embolism (PE),3,4 possibly due to alteration of the coagulation pathway protein concentration. 4
Ospemifene is an oral, non-steroidal SERM approved in the United States (US) in 2013 for treatment of moderate-to-severe dyspareunia, a symptom of vulvar and vaginal atrophy (VVA), due to menopause.2,5 Ospemifene received approval in Europe in 2015 for treatment of moderate-to-severe symptoms of VVA in postmenopausal women who are not candidates for local vaginal estrogen therapy.6,7
VVA is an underdiagnosed and undertreated condition, and current therapies include systemic and local estrogens and lubricants/moisturizers; ospemifene is the only SERM approved for VVA. 8 The pivotal randomized, ospemifene clinical trials, and a meta-analysis of six randomized controlled trials, indicated that ospemifene 60 mg alleviated dyspareunia and vaginal dryness compared with placebo.9–16 The incidence of headaches, DVT, coronary heart disease, and cerebrovascular events (CVE) was similar between ospemifene and placebo, 9 suggesting it was well tolerated.
Considering the known risk of VTE with SERMs, real-world studies of the risk of VTE with ospemifene are needed. The European Medicines Agency mandated a 5-year post-authorization safety study (PASS) to examine the incidence of VTE and other outcomes among ospemifene users. We previously published interim descriptive results from this PASS, reporting a low incidence of VTE among ospemifene users, with no indication of an increased risk compared with other SERMs or untreated VVA. 17 This paper reports the final findings with comparative analysis results from the PASS.
Methods
Study design and data source
This was a retrospective cohort study using the IBM Watson MarketScan Commercial and Medicare Supplemental claims database from the United States, which contains information for more than 200 million covered lives. Medical and pharmacy claims data between 1 May 2012 and 31 December 2018 were used for this study. Details of the study design have been reported previously. 17
Study cohorts
Three cohorts of women aged ⩾54 years (as a conservative proxy for post-menopausal status) were identified from the MarketScan database from 1 May 2013 to 2 October 2018: ospemifene initiators, comparator SERM initiators (receiving raloxifene, bazedoxifene, or tamoxifen for breast cancer prevention or estrogen-deficiency conditions), and an untreated VVA cohort. The index date was the drug start date for the treated cohorts and the initial VVA diagnosis date for the untreated group. Details of inclusion and exclusion criteria have been reported previously, 17 and are included in Supplementary Box 1.
Variable definitions
Exposure
Exposure to ospemifene and other SERMs was defined using treatment episodes of continuous medication use with no more than a 30-day gap, as in the previous study. 17 Exposure to different comparator SERMs was considered as a single exposure; switching among the comparator SERMs did not lead to a change in exposure category.
Outcome
The primary outcome was first occurrence of a diagnosis code for VTE, overall and categorized as DVT, PE, or retinal vein thrombosis. Secondary outcomes included CVEs, endometrial hyperplasia, endometrial cancer, pelvic organ prolapse, urinary incontinence, gallbladder events, atrial fibrillation, renal failure, renal carcinoma, renal adenoma, liver tumors, thymic epithelial tumors, increased triglycerides, and vaginal bleeding. Patients were followed for outcomes from the day after the index date until end of enrollment in the database or end of the study period (31 December 2018).
Covariates
Demographic characteristics at index date and healthcare utilization from the 6 months before index were examined as in the previous interim analysis. 17 Comorbidities that could be associated with VTE risk 18–27 were assessed from the 1-year baseline period, including atrial fibrillation, transient ischemic attack, hypertension, diabetes mellitus, atherosclerosis, immobility, congestive heart failure, obesity, chronic obstructive pulmonary disease, rheumatic disease, chronic kidney disease, inflammatory bowel disease, and inherited or acquired thrombophilia. Trauma and surgery were examined within 90 days before index. Receipt of relevant medications during the baseline period were also noted as in the previous interim analysis. 17
Statistical analysis
Descriptive analysis
The incidence rate and Poisson 95% confidence intervals (CIs) of VTE during the first continuous treatment episode for ospemifene and other SERMs and first episode of untreated time for the untreated VVA cohort were calculated. A Kaplan-Meier (KM) plot presented time to first event.
The incidence of VTE was also estimated during all follow-up time using an intention to treat (ITT) approach, and during the first 90 days of the first treatment episode (i.e. censored at 90 days of follow-up). It was also calculated by type (DVT, PE, or retinal vein thrombosis) and by age at index date (54–72 years and ⩾ 73 years).
Similar analyses were performed for incidence of CVE, an important secondary outcome. The other secondary outcomes were assessed descriptively, as number and percentage of patients experiencing each event and incidence rate with 95% CI.
Comparative analysis during the first continuous treatment episode
Univariable Cox models estimated unadjusted hazard ratios (HRs) for treatment group and each baseline variable. Covariates that modified the HR for treatment group by ⩾ 5% were included in the final model.
Since age, a major risk factor for VTE and CVE, varied considerably across treatment groups, comparative analyses were conducted only in women aged 54–72 years, representing approximately 99% of ospemifene users. Age was modeled as a continuous variable and as age-squared to further adjust for this key confounder.
Sensitivity analyses
Several sensitivity analyses were conducted. First, Cox models assessed VTE and CVE during all follow-up time (the ITT analysis) as well as during the first 90 days of the first treatment episode.
Another sensitivity analysis used propensity score methods that included all patients without age restriction. Logistic regression models were constructed with all baseline variables as predictors and receipt of ospemifene versus other SERMs (and separately, ospemifene vs untreated VVA) as the outcome. These models estimated each patient’s propensity for receiving ospemifene. Patients were matched 1:1 on propensity score using a nearest neighbor approach with a caliper of 0.2 times the standard deviation (SD) of the logit of the propensity score. Standardized differences assessed the balance between matched groups. Incidence rates and Cox models of VTE and CVE were rerun in the matched groups, using a robust variance estimator in the Cox models to account for the matching.
A final sensitivity analysis on VTE following ospemifene users from the VVA diagnosis date assessed the potential immortal time bias that the primary analysis might contain. Ospemifene use was a time-varying exposure, and initiators lacking a VVA diagnosis were assigned two imputed VVA diagnosis dates, defined as 10 days before ospemifene start (the median gap between diagnosis and ospemifene initiation for diagnosed patients) and 30 days before ospemifene start. The baseline and follow-up variables were redefined using these VVA index dates. Cox models of VTE included any time prior to ospemifene start in the ospemifene-treated patients as untreated time.
Results
Cohort selection
A total of 31,405 women had a dispensing of ospemifene from 1 May 2013 to 2 October 2018. Approximately 30% were aged < 54 years and excluded. The final cohort included 8,977 women after applying further inclusion and exclusion criteria. The comparator cohorts included 12,621 initiators of a comparator SERM and 242,488 women with untreated VVA (Supplementary Figure 1).
Characteristics of study cohorts
Mean age was 59.0, 63.7, and 62.3 years for the ospemifene, comparator SERM, and untreated VVA cohorts, respectively (Table 1). The most common comparator SERM was raloxifene (11,639 [92.2%]) followed by tamoxifen (982 [7.8%]); no bazedoxifene use was found. During the 6 months before index, both comparator groups had higher frequency of physician and emergency room visits and hospitalizations than the ospemifene group. In the 1-year baseline period, hypertension was the most common comorbidity in all cohorts, followed by diabetes; antihypertensives and lipid-lowering therapy were the most commonly dispensed medications. The ospemifene cohort had the lowest frequency of most comorbidities and medication use.
Baseline characteristics of ospemifene initiators and comparators.
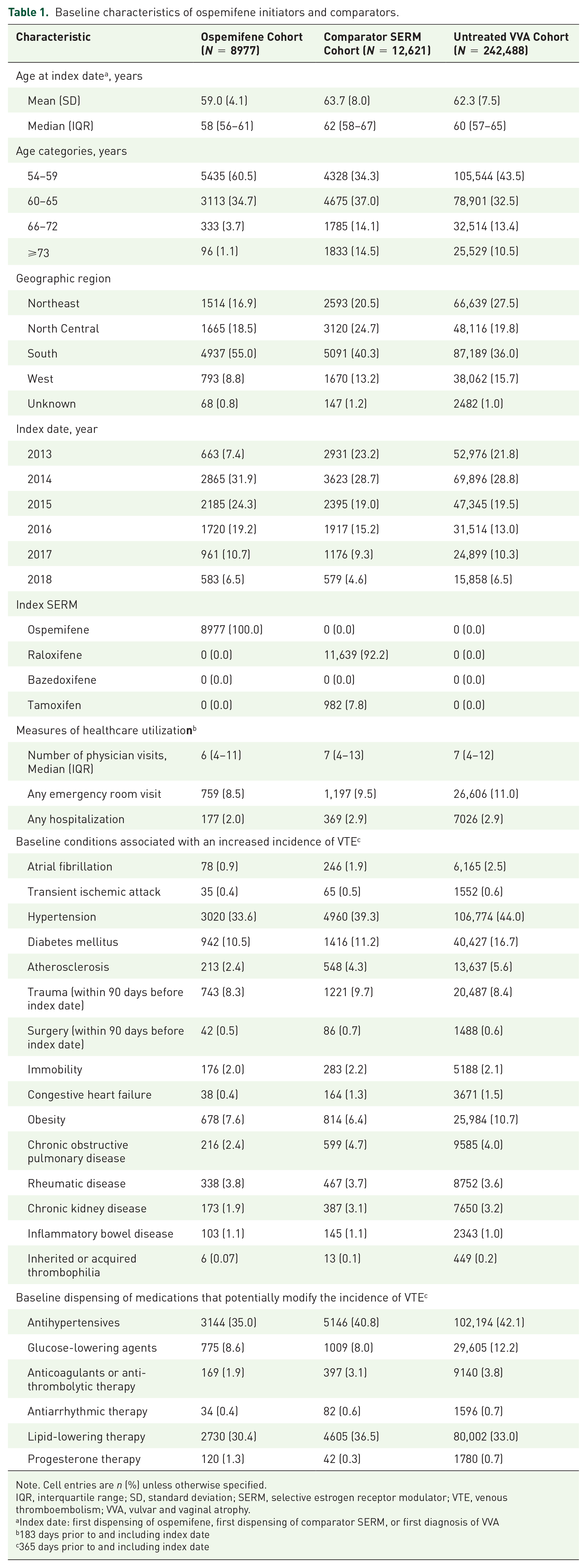
Note. Cell entries are n (%) unless otherwise specified.
IQR, interquartile range; SD, standard deviation; SERM, selective estrogen receptor modulator; VTE, venous thromboembolism; VVA, vulvar and vaginal atrophy.
Index date: first dispensing of ospemifene, first dispensing of comparator SERM, or first diagnosis of VVA
183 days prior to and including index date
365 days prior to and including index date
Incidence of VTE
In the age 54–72 years subgroup, during the first treatment episode, 9 (0.1%) ospemifene users experienced a VTE, with an incidence rate of 3.42 (95% CI: 1.57–6.50) events per 1000 person-years (PY) (Table 2). In the comparator SERM cohort, 55 (0.5%) women developed a VTE, with an incidence of 10.56 (95% CI: 7.95–13.74) per 1000 PY. VTE occurred in 1788 (0.8%) women in the untreated VVA cohort; the incidence rate was 9.11 (95% CI: 8.69–9.54) per 1000 PY. In all cohorts, most events were DVT, and retinal vein thrombosis was rare (Table 2). As expected, the incidence of VTE increased in women aged ⩾ 73 years in both comparator cohorts; however, the older age group in the ospemifene cohort was too small to identify any events. Among women aged 54–72 years with a VTE, the median time to event was 115, 105, and 196 days for ospemifene, comparator SERMs, and women with untreated VVA, respectively (Supplementary Figure 2).
Frequency and incidence of VTE during first continuous treatment episode, all follow-up time, and first continuous treatment episode censored at 90 days by age category.

Ages are in years
CIs calculated using the Poisson distribution
Patients eligible for outcome did not have outcome during baseline.
CI, confidence interval; IR, incidence rate; PY, person-years; SERM, selective estrogen receptor modulator; VTE, venous thromboembolism; VVA, vulvar and vaginal atrophy.
The ITT results were similar to the primary analysis (Table 2). During all available follow-up time among women aged 54–72 years, 33 (0.4%) in the ospemifene cohort developed a VTE, with an incidence of 4.54 (95% CI: 3.12–6.37) per 1000 PY. The incidence for the comparator SERM cohort was 10.50 (95% CI: 8.60–12.70) per 1,000 PY and 9.11 (95% CI: 8.69–9.54) per 1000 PY for untreated VVA. Among women with a VTE, the median time to event was 195, 147, and 196 days for ospemifene, comparator SERMs, and women with untreated VVA, respectively (Supplementary Figure 3).
Fewer than half of the VTE events in each cohort occurred during the first 90 days of the first treatment episode. The incidence of VTE in women aged 54–72 years was lower than in the primary analysis for the ospemifene cohort, at 2.63 (95% CI: 0.72–6.73) per 1,000 PY, but largely the same as in the primary analysis for both comparator cohorts.
Comparative analyses from first continuous treatment episode in women aged 54–72 years
Only age-squared modified the HR for treatment group by >5% when comparing ospemifene with other SERMs; therefore, it was the only covariate included in the adjusted model (Table 3). The adjusted model confirmed the lower risk of VTE for ospemifene vs other SERMs (HR: 0.40, 95% CI: 0.19–0.82). The comparison with untreated VVA included age-squared and hypertension as covariates, generating an HR of 0.47 (95% CI: 0.24–0.91).
Adjusted Cox model of time to first venous thromboembolism during first continuous treatment episode, in women aged 54 to 72 years.

Variables selected for final model are those that modify the HR for treatment group by at least 5%
CI, confidence interval; HR, hazard ratio; SERM, selective estrogen receptor modulator; VTE, venous thromboembolism; VVA, vulvar and vaginal atrophy.
Sensitivity analyses
The ITT results were similar to the primary analysis for the comparison with other SERMs, although age did not act as a confounder; the HR for ospemifene was 0.45 (95% CI: 0.30–0.66) (Supplementary Table 1). In the comparison with the untreated cohort, age-squared and hypertension acted as confounders; the analysis revealed an attenuated effect size for ospemifene exposure, with an adjusted HR of 0.60 (95% CI: 0.43–0.85). Censoring the first treatment episode at day 90 produced a somewhat stronger effect for ospemifene vs comparator SERMs than the primary analysis (adjusted HR: 0.29, 95% CI: 0.10–0.88). The comparison with the untreated cohort censoring at day 90 estimated an adjusted HR for ospemifene of 0.37 (95% CI: 0.14–1.00).
The propensity score models indicated numerous predictors of treatment group. Of the 8977 ospemifene users, 7547 (84.1%) were successfully matched to a comparator SERM user and all were matched to a woman with untreated VVA. Matching successfully reduced all standardized differences between baseline variables to < 0.10. The final Cox models were univariate models of treatment group. These models confirmed the lack of increase in risk of VTE with ospemifene relative to other SERMs (HR: 0.42, 95% CI: 0.18–0.96) and untreated VVA (HR: 0.65, 95% CI: 0.31–1.38).
A VVA diagnosis was recorded at baseline for 4483 (49.9%) ospemifene users. The index date for ospemifene users was set to the date of first VVA diagnosis, if present, or 10 days prior to ospemifene start if missing, and the inclusion/exclusion criteria were applied to the new index date, retaining 7538 (88.4%) of the ospemifene users from the primary cohort. The adjusted Cox model estimated an HR for ospemifene exposure of 0.60 (95% CI: 0.34–1.07). Replacing the imputed VVA diagnosis date of 10 days prior to ospemifene start with an earlier date (30 days prior to ospemifene start) produced similar results, with an adjusted HR for ospemifene exposure of 0.66 (95% CI: 0.37–1.16).
Secondary outcomes
During the first treatment episode among the patients aged 54–72 years, the incidence of CVE was lower in the ospemifene cohort than comparators (Supplementary Table 2). Both adjusted Cox models and Cox models comparing the propensity matched groups without age restriction indicated no difference in risk of CVE (Supplementary Table 3).
Only increased triglycerides occurred in >5% of the ospemifene cohort, at an incidence rate of 209.46 (95% CI: 188.00–232.70) per 1000 PY. Uterine diagnostic tests and procedures occurred in 2.7% of the cohort, at an incidence of 91.32 (95% CI: 79.75–104.10) per 1000 PY. No other outcomes occurred in > 1% of ospemifene users. Rates of each secondary outcome were generally similar across the three cohorts (Supplementary Table 2).
Discussion
In this retrospective analysis of real-world ospemifene use, the incidence of VTE was low, and less than half the rate among women receiving other SERMs or with untreated VVA. This pattern held true in the first continuous course of treatment as well as several modifications to the follow-up risk period and changes to the analytic approaches for reduction of confounding.
The ospemifene cohort was younger than the comparator cohorts, with lower prevalence of some known VTE risk factors (e.g. hypertension, atrial fibrillation, and chronic obstructive pulmonary disease).18–27 Hence, age restriction as well as adjustment were used for comparative analyses.
The Cox models confirmed the lack of increased risk of VTE with ospemifene relative to comparator SERM or untreated VVA. In all comparisons with other SERMs, the risk of VTE was lower in the ospemifene cohort. The comparisons with untreated VVA did not consistently find a reduced risk of VTE with ospemifene (i.e. some 95% CIs crossed the null value), but found no indication of an increase in risk, regardless of the modeling approach used. The CVE analyses suggest that the use of ospemifene, regardless of age, was not associated with an increased risk of CVE relative to other SERMs or untreated VVA.
The finding that the SERMs differed with regard to the risk of VTE is not unexpected. Unlike estrogens, which are uniformly estrogen-receptor agonists, the SERMs exert selective agonist, antagonist, or neutral effects on different target tissues. The effects depend on differential estrogen-receptor expression in a given target tissue, differential estrogen-receptor conformation on ligand binding, and differential expression and binding to the estrogen receptor of coregulator proteins. 28
Since their therapeutic effects and indications are different, 29 SERMs can also have different side effects. Therefore, their risks of inducing VTE can vary significantly. It is plausible that the risk of thromboembolism (originally identified for estrogens) was overestimated for some SERMs and overgeneralized as a class label effect, whereas in reality a broad spectrum of effects is likely. We would expect some SERMS to increase the risk of VTE, while others do not.
The results of this real-world analysis are consistent with the ospemifene clinical development program, which found an incidence of VTE of 3.65 (95% CI: 0.44–13.90) per 1000 PYs with ospemifene and 3.66 (0.09–20.41) per 1000 PYs with placebo.9–16,30 Also, the rates of CVE and other secondary outcomes were similar between groups in the ospemifene clinical trials,9–16,30 in line with the present study’s findings.
Limitations of the study include the use of claims data, which contain diagnosis codes used for billing purposes that may be inaccurate and primarily represents large employers. 31 Thus, findings may not be generalizable to individuals with other types of insurance or without health insurance, as well as those from outside the United States. As VVA tends to be underreported, 8 the untreated VVA cohort may represent women who report VVA symptoms to their healthcare providers and receive the diagnosis, but not all women with VVA. In addition, lifestyle factors for VTE, such as body mass index and smoking status, are not available in claims data. It is possible that women who take ospemifene engage in other health-improving behaviors, which may help reduce their risk of VTE and other adverse outcomes.
It is not known why the untreated VVA group did not obtain a prescribed treatment or why half of the ospemifene group had no recorded VVA diagnosis. Similarly, the other SERMs had a different indication than the ospemifene cohort. Various analytic approaches addressed these issues, although each carried its own limitations. The primary analysis of VTE during the first treatment episode examined the most appropriate risk window and utilized a transparent, efficient covariate selection method; however, follow-up duration differed among the cohorts. Altering the risk windows to the first 90 days and to all follow-up time supplemented the primary analysis of the outcomes, although the inherent imbalance in exposure durations and indications still existed.
Propensity score matching adjusted simultaneously for many variables and generated well-balanced groups (among measured characteristics) but sacrificed some generalizability and precision of the estimates by excluding unmatched patients.
As the SERM class carries a known risk of VTE,3,4 the finding of lower risk with ospemifene indicates that it (in contrast to the other drugs in its class) is unlikely to increase the risk of VTE. The comparison with untreated VVA supports the interpretation that ospemifene use was not associated with increased risk of VTE. All analyses produced point estimates of the HR for ospemifene vs comparators below 1.0, reinforcing the robust finding of no increase in risk of VTE. Residual confounding from factors unavailable in claims data (e.g. smoking) 32 may still exist, but the effect of any unmeasured confounder would have to be very large and very common to overturn these results.
Conclusions
The safety analyses of ospemifene use in real-world medical practice found a low rate of VTE and other adverse outcomes, confirming the findings observed during the ospemifene development program. The rate of VTE in ospemifene users was more than three times lower than the rate with other SERMs. The reduced risk of VTE with ospemifene relative to other SERMs persisted, although somewhat attenuated, after age restriction and adjustment through various analytical approaches. The reduced risk observed with ospemifene versus comparator SERMs from all analyses performed and consistent differentiation observed between the Kaplan-Meier curves from the beginning strongly suggest that unlike other SERMs, ospemifene does not increase the risk of VTE. In contrast, several models comparing ospemifene with untreated VVA produced adjusted HRs with a 95% CI that crossed the null value, despite consistently showing numerically lower incidence of VTE. The two sets of comparisons performed in this real-world analysis clearly indicate that there is no increased risk of VTE with the use of ospemifene among postmenopausal women and suggests that the SERM-associated elevated risk of VTE does not apply to ospemifene.
Supplemental Material
sj-docx-1-taw-10.1177_20420986221135931 – Supplemental material for Risk of venous thromboembolism among women receiving ospemifene: a comparative observational study
Supplemental material, sj-docx-1-taw-10.1177_20420986221135931 for Risk of venous thromboembolism among women receiving ospemifene: a comparative observational study by Beth L. Nordstrom, Bin Cai, Fabio De Gregorio, Lu Ban, Kathy H. Fraeman, Yuki Yoshida and Trevor Gibbs in Therapeutic Advances in Drug Safety
Supplemental Material
sj-tif-3-taw-10.1177_20420986221135931 – Supplemental material for Risk of venous thromboembolism among women receiving ospemifene: a comparative observational study
Supplemental material, sj-tif-3-taw-10.1177_20420986221135931 for Risk of venous thromboembolism among women receiving ospemifene: a comparative observational study by Beth L. Nordstrom, Bin Cai, Fabio De Gregorio, Lu Ban, Kathy H. Fraeman, Yuki Yoshida and Trevor Gibbs in Therapeutic Advances in Drug Safety
Supplemental Material
sj-tif-4-taw-10.1177_20420986221135931 – Supplemental material for Risk of venous thromboembolism among women receiving ospemifene: a comparative observational study
Supplemental material, sj-tif-4-taw-10.1177_20420986221135931 for Risk of venous thromboembolism among women receiving ospemifene: a comparative observational study by Beth L. Nordstrom, Bin Cai, Fabio De Gregorio, Lu Ban, Kathy H. Fraeman, Yuki Yoshida and Trevor Gibbs in Therapeutic Advances in Drug Safety
Supplemental Material
sj-tiff-2-taw-10.1177_20420986221135931 – Supplemental material for Risk of venous thromboembolism among women receiving ospemifene: a comparative observational study
Supplemental material, sj-tiff-2-taw-10.1177_20420986221135931 for Risk of venous thromboembolism among women receiving ospemifene: a comparative observational study by Beth L. Nordstrom, Bin Cai, Fabio De Gregorio, Lu Ban, Kathy H. Fraeman, Yuki Yoshida and Trevor Gibbs in Therapeutic Advances in Drug Safety
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.