
Abstract
Prescribing of potentially inappropriate medications (PIMs) that pose more risk than benefit in older patients is a common occurrence across all healthcare settings. Reducing such prescribing has been challenging despite multiple interventions, including educational campaigns, audits and feedback, geriatrician assessment and formulary restrictions. With the increasing uptake of electronic medical records (EMRs) across hospitals, clinics and residential aged care facilities (RACFs), integrated with computerized physician order entry (CPOE) and e-prescribing, opportunities exist for incorporating clinical decision support systems (CDSS) into EMR at the point of care. This narrative review assessed the process and outcomes of using EMR-enabled CDSS to reduce the prescribing of PIMs. We searched PubMed for relevant articles published up to January 2018 and focused on those that described EMR-enabled CDSS that assisted prescribers to make changes at the time of ordering PIMs in adults. Computerized systems offering only medication reconciliation, dose checks, monitoring for medication errors, or basic formulary information were not included. In addition to outcome measures of medication-related processes and adverse drug events, qualitative data relating to factors that influence effectiveness of EMR-enabled CDSS were also gathered from selected studies. We analysed 20 studies comprising 10 randomized trials and 10 observational studies performed in hospitals (n = 8), ambulatory care clinics (n = 9) and RACFs (n = 3). Studies varied in patient populations (although most involved older patients), type of CDSS, method of linkage with EMR, study designs and outcome measures. However, assuming little publication bias, the totality of evidence favoured EMR-enabled CDSS as being effective in reducing the prescribing of PIMs in hospitals, although results were more mixed for ambulatory care settings and RACFs. While absolute effects in most positive studies were modest, they suggest EMR-enabled CDSS are feasible and acceptable to clinicians, and if certain design features are adhered to, there is potential for even greater impact.
Keywords
Introduction
Advances in the treatment of medical conditions mean more people are living with multiple comorbidities into an older age. In Australia, 43% of adults, 50 years or older, take five or more prescribed medications, 1 with similar rates in the US 2 and Europe. 3 It is imperative medications are used appropriately in this population to maximize positive health outcomes, while also ensuring the sustainability of government healthcare programmes and minimizing harm to patients. Polypharmacy and potentially inappropriate medications (PIMs) i.e. medications used in a manner that poses more risk than benefit particularly where safer alternatives exist, have been associated in observational studies with reduced quality of life, adverse drug events (ADEs), falls, nonadherence, hospitalizations, mortality and increased healthcare utilization and cost.4–8 It is estimated that among people aged 65 years or older, at least one PIM is regularly prescribed to between 25% and 56% of hospitalized patients, 9 up to a third of community-dwelling subjects 10 and almost half of those living in residential aged care facilities (RACFs). 11 Approximately one in five medicines commonly used in older people may be inappropriate, 12 rising to a third among those living in RACFs. 13
Various reviews have detailed strategies for reducing the prescribing of PIMs, such as educational campaigns, audits and feedback, geriatrician assessment and formulary restrictions.14–16 More recently, deprescribing has been defined as the process of systematically identifying and withdrawing PIMs among individual patients where current or potential harm outweigh current or potential benefit after taking into consideration an individual’s comorbidities, life expectancy, quality of life, and values and preferences. 17 Various tools, frameworks, criteria, algorithms and structured guides have been developed that aim to assist the prescriber in the task of deprescribing.11,18–21
With the increasing uptake of electronic medical records (EMRs) across all healthcare settings incorporating computerized physician order entry (CPOE) and e-prescribing systems,22,23 opportunities exist for integrating clinical decision support systems (CDSS) into EMRs at the point of care. Reviews have highlighted the efficacy of CDSS and e-prescribing in reducing prescribing errors and ADEs and improving overall quality use of medicines, albeit on fairly weak evidence.24–28 However, these reports have not focused specifically on EMR-enabled CDSS that aim to reduce the prescribing of PIMs. A study of two large outpatient practices using EMRs has identified that 23% of older patients receive at least one PIM, as defined by the Beers criteria. 29 Among hospitalized patients subject to STOPP (screening tool of older persons’ prescriptions) criteria, review of EMR data showed 55% received one or more PIM. 30
In this article, we provide a narrative review of studies which have assessed the process and outcomes of using EMR-enabled CDSS to reduce the prescribing of PIMs.
Methods
PubMed was searched for articles, either single studies or systematic reviews, containing text words ‘electronic medical record’ and ‘deprescribing’ ‘polypharmacy’ ‘inappropriate prescribing’ ‘decision support systems’ and their related synonyms in the title or abstract, and which were published up to January 2018. The ‘related functions’ tab in PubMed, perusal of bibliographies of retrieved articles, and searches in Google Scholar using similar search terms were used to find additional articles, and personal files kept by the authors were also consulted. Articles were selected [initially by one author (IAS) and then confirmed by consensus with other authors] if they described electronic prescribing software integrated or interfaced with EMR (or its CPOE or e-prescribing components) and using CDSS in some form that enables prescribers to make changes at the time of prescribing in adults. 31 Studies describing stand-alone e-prescribing systems or EMR-linked systems devoid of CDSS targeting PIMs (i.e. offering only medication reconciliation, dose checks, monitoring for medication errors, or basic formulary information) were excluded, as were studies of CDSS for which data relating specifically to PIM prescribing were not reported, studies not written in English, or studies performed in nondeveloped countries. Articles were categorized according to hospital, ambulatory or residential care settings, and experimental versus observational studies. Outcomes were assessed in terms of process (medication-related) measures and patient outcomes. Qualitative data providing insights into factors that influence effectiveness of EMR-linked CDSS were also gathered from selected studies.
Results
We analysed 20 studies comprising 10 randomized controlled trials (RCTs) and 10 observational studies performed in hospitals (n = 8), ambulatory care clinics (n = 9) and RACFs (n = 3). Details of each study are briefly summarized in Table 1.
Summary of individual studies.
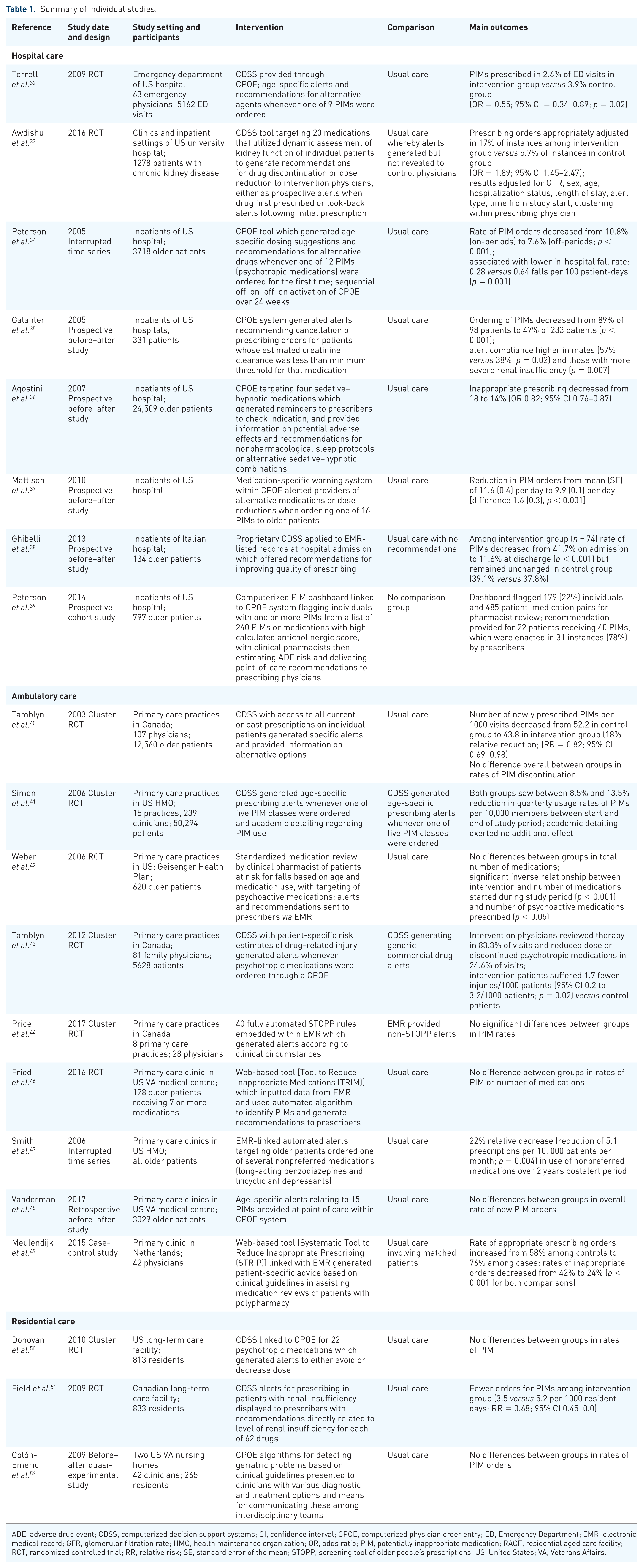
ADE, adverse drug event; CDSS, computerized decision support systems; CI, confidence interval; CPOE, computerized physician order entry; ED, Emergency Department; EMR, electronic medical record; GFR, glomerular filtration rate; HMO, health maintenance organization; OR, odds ratio; PIM, potentially inappropriate medication; RACF, residential aged care facility; RCT, randomized controlled trial; RR, relative risk; SE, standard error of the mean; STOPP, screening tool of older people’s prescriptions; US, United States; VA, Veterans Affairs.
Hospital care
Experimental studies
In an RCT involving 63 emergency department (ED) physicians, CDSS was provided through CPOE in which age-specific alerts and suggestions for safer alternatives appeared when physicians in the intervention arm tried to order one of nine PIMs. 32 Among 2647 ED visits involving older patients who were managed by intervention physicians, 111 visits involved an order for a PIM, for which the CDSS generated 114 recommendations which were accepted 49 times (43%). This compared with 99 of 2515 visits managed by control physicians for which a PIM was ordered, such that PIMs were prescribed in 2.6% versus 3.9% of ED visits among intervention and control physicians respectively [odds ratio (OR) = 0.55, 95% confidence interval (CI) = 0.34–0.89; p = 0.02]. The proportion of all medications that were inappropriate dropped from 5.4 to 3.4% postintervention.
In another RCT involving 1278 patients with chronic kidney disease in both clinic and inpatient settings, subjects were randomized to prescribers who had or did not have access to a CDSS tool. 33 The CDSS tool which targeted 20 medications was embedded in an EMR that utilized dynamic assessment of patients’ kidney function to detect scenarios in which drug discontinuation or dosage reduction was recommended, both at the time of initial prescription (‘prospective’ alerts) and by monitoring changes in renal function for patients already receiving a study medication (‘look-back’ alerts). A total of 4068 triggers occurred in 1278 unique patients; 1579 alerts seen by intervention physicians and 2489 captured but suppressed for control physicians. Prescribing orders were appropriately changed in 17% of instances in the intervention arm versus 5.7% of instances in control arm (OR 1.89, 95% CI 1.45–2.47; p < 0 .0001). Prospective alerts had greater impact than look-back alerts (55.6% versus 10.3% alerts leading to changes in orders).These results were adjusted for glomerular filtration rate, sex, age, hospital teaching status, length of stay, type of alert, time from start of study, and clustering within prescribing physician. While this was a positive result, authors remained concerned at the high rates of inappropriate drug prescribing in patients with kidney impairment despite the alerts.
Observational studies
In an interrupted time-series study involving 3718 older individuals, age-specific dosing suggestions and offers of alternatives to 12 potentially inappropriate psychotropic medications were displayed to physicians through a CPOE system for two of four 6-week study periods in an off–on–off–on pattern. 34 Among a total of 7456 initial orders for psychotropic medications, the rate of PIM orders decreased from 10.8% to 7.6% (p < 0.001), in association with a lower in-hospital fall rate (0.28 versus 0.64 falls per 100 patient-days, p = 0.001). No effect on hospital length of stay or days of altered mental status was found.
In a prospective before–after study, automated alerts recommending order cancellation appeared when a medication was ordered in a CPOE system for a patient whose estimated creatinine clearance was less than the minimum threshold defined for that medication. 35 The prescribing of PIMs was assessed for 4 months before, and 14 months after, alert implementation. The frequency of patients receiving at least one dose of a PIM decreased from 89% of 98 unique patients to 47% of 233 unique patients (p < 0.001) after alert implementation (42% absolute reduction). Orders were cancelled in 41% of instances in which an alert was given. Alert compliance was higher in male patients (57% versus 38%, p = 0.02) and those with more severe renal insufficiency (p = 0.007), and was greater among staff who received more prolonged training (59% with >24 months versus 34% with <6 months training; p = 0.04) .
A prospective before–after study involving 24,509 individuals targeted the prescribing of four sedative–hypnotic medications (diphenhydramine, diazepam, lorazepam, and trazodone). Reminder screens appeared in the CPOE system requesting prescribers to check the indication and offered information on potential adverse effects and recommendations for nonpharmacological sleep protocols or alternative sedative–hypnotic combinations. 36 Prescribing of inappropriate sedative–hypnotics decreased from 18% of 12,536 patients over 12 months pre-implementation to 14% of 12,153 patients postimplementation (OR 0.82, 95% CI 0.76–0.87), with 95% being successfully directed to a safer sedative–hypnotic drug or a nonpharmacological sleep protocol.
In another prospective before–after study, a medication-specific warning system within CPOE alerted providers of alternative medications or dose reductions when ordering one of 16 PIMs to older patients. 37 PIM orders were reduced from a mean [standard error (SE)] of 11.6 (0.4) per day in the 19 months pre-implementation to 9.9 (0.1) orders per day in the 20 months postimplementation [difference 1.6 (0.3); p < 0.001]. There was no evidence that the effect waned over time or was affected by secular trends and season, although the study could not determine whether ADEs were reduced.
In a prospective before–after study involving 134 patients aged ⩾ 65 years, a CDSS for detecting inappropriate prescribing called INTERcheck® was applied to EMR-listed records of two patient groups; a control group where the CDSS analysed medication lists of 74 patients but offered no recommendations to clinicians, followed by an intervention group of 60 patients where recommendations were offered. 38 The number of control patients exposed to at least one PIM remained unchanged between admission and discharge (n = 29; 39.1% versus n = 28; 37.8 %) but in the intervention group decreased from 25 (41.7 %) to 7 (11.6 %; p < 0.001). Among intervention patients throughout the observation period, the number of new-onset potentially severe drug–drug interactions among those receiving PIMs also decreased from 37 (59.0 %) to 9 (33.0 %; p < 0.001).
In a pilot intervention study involving 797 older adults admitted to general medicine, orthopaedics and urology services of a tertiary hospital over a 3-week period, a computerized PIM dashboard linked to a CPOE system flagged individuals with at least one administered PIM from a list of 240 PIMs or medications with a high calculated anticholinergic score. 39 Participating clinical pharmacists estimated ADE risk using logical combinations of data (e.g. use of multiple sedatives) and delivered immediate point-of-care recommendations (by phone or text message) to treating physicians. The dashboard flagged 179 (22%) individuals and 485 participant-medication pairs for pharmacist review, with recommendations warranted for 22 participants receiving 40 PIMs, which were enacted in 31 instances (78%) by clinicians.
Ambulatory care
Experimental studies
A cluster RCT involving 107 primary care physicians and 12,560 older patients assessed a CDSS intervention that provided access to a complete drug profile of all current or past prescriptions on individual patients through a dedicated link between the EMR and an electronic drug insurance programme. 40 Intervention physicians received pop-up age-specific alerts when prescribing a PIM, informing them of possible consequences and alternative therapies. The number of new PIMs per 1000 visits was 18% lower in the intervention versus control group [43.8 versus 52.2; relative risk (RR) 0.82, 95% CI 0.69–0.98]. However, differences between groups for PIM discontinuation rates were significant only for therapeutic duplications ordered by study physician and another physician (RR 1.66, 95% CI 0.98–4.70) and drug interactions caused by prescriptions written by study physician (RR 2.15, 95% CI 0.98–4.70).
In another cluster RCT involving 15 practices (239 clinicians, 50,924 patients) within a health maintenance organization, all practices received computerized age-specific prescribing alerts whenever a PIM (tertiary tricyclic amine antidepressants, long-acting benzodiazepines, propoxyphene, nonsteroidal anti-inflammatory drugs, muscle relaxants) was ordered. 41 Seven practices also received academic detailing regarding PIM use, while the other eight practices did not. Using interrupted time series analysis applied to 2 years before and 1.5 years after substituting age-specific for drug-specific alerts, both groups saw between 8.5% and 13.5% reduction in the quarterly usage rates of PIMs per 10,000 members (146.3 to 126.6 and 150.2 to 137.2, respectively). Academic detailing exerted no additional effect.
Another RCT involving 620 community-dwelling patients aged over 70 years and at risk for falls based on age and medication use, assessed a standardized medication review by a pharmacist who targeted psychoactive medications and sent messages to prescribers via the EMR, alerting them of the risk of falls and offering recommendations for alternative medications. 42 Patient self-reports of falls were collected at 3-month intervals over the 15-month study period; fall-related diagnoses and medication data were collected through the EMR. Although the intervention did not reduce the total number of medications, a significant negative relationship was seen between the intervention and the total number of medications started during the study period (regression estimate −0.199; p < 0.01) and the total number of psychoactive medications (regression estimate −0.204; p < 0.05.) The intervention group was 0.38 times as likely to have had one or more fall-related diagnoses (p < 0.01), but no impact was seen when data on self-reported falls was included.
In another RCT involving 81 family physicians and 5628 patients who received orders for psychotropic drugs, CDSS with patient-specific risk estimates of drug-related injury generated alerts to intervention prescribers whenever psychotropic medications were ordered through a CPOE, versus control prescribers receiving commercial drug alerts. 43 Patient-specific risk of injury was computed at the time of each visit using statistical models of nonmodifiable risk factors (age, sex, injury history, presence of cognitive impairment, gait, and balance problems) and psychotropic drug doses. Risk thermometers presented changes in absolute and relative risk with each change in drug treatment. Intervention physicians reviewed orders in 83.3% of visits and dose reduced or discontinued psychotropic medication in 24.6% visits, resulting in 1.7 fewer injuries/1000 patients (95% CI 0.2–3.2; p = 0.02) compared with controls, with greater effects for patients with higher baseline risks of injury (p < 0.03).
In a cluster RCT involving 28 physicians from eight primary care practices, 40 fully automated STOPP rules were implemented as EMR alerts during a 16-week intervention period, with the control group receiving other non-STOPP alerts. 44 The calculated PIM rate was 2.6% (138/5308) in control practices and 4.11% (768/18,668) in intervention practices at baseline. No significant change in PIMs was observed among intervention patients.
In an RCT involving 128 patients aged 65 years and older who were receiving seven or more medications and attending a primary care clinic, a web tool [Tool to Reduce Inappropriate Medications (TRIM)] 45 linking an EMR to a CDSS was assessed for its effects on deprescribing PIMs, based largely on Beers and STOPP criteria. 46 TRIM extracted information on medications and chronic conditions from the EMR and contained data entry screens for information obtained from brief chart review and telephonic patient assessment. These data served as input for automated algorithms identifying PIMs, with feedback reports to clinicians providing deprescribing recommendations. After adjusting for covariates and clustering of patients within clinicians, no effect on deprescribing medications or reducing PIMs was seen, although the study may have been underpowered.
An interrupted time series analysis over a 39-month period was used to evaluate changes in medication prescribing as a result of EMR-linked computerized alerts cautioning against specific medications (long-acting benzodiazepines and tertiary amine tricyclic antidepressants) in older persons attending primary care clinics of a US health maintenance organization. 47 The alerts were constructed so that warnings regarding falls and fracture risk were prominent, with further information on specific alternative psychoactive agents. Over 2 years following alert implementation, there was a persistent 22% reduction (5.1 prescriptions per 10, 000 per month; p = 0.004) in use of nonpreferred medications compared with 12 months pre-implementation. There was no offsetting increase in use of preferred psychoactive medications, indicating less overall exposure of older patients to psychoactive medications.
Observational studies
In a retrospective before–after study involving 3029 older patients, age-specific alerts relating to 15 PIMs based on Beers criteria were provided at point of care within a CPOE system. 48 A total of 1539 patients pre-alert and 1490 patients postalert were prescribed 1952 and 1897 PIMs, respectively. No significant reductions in the rate of new PIM orders were seen overall, 12.0 to 12.6%, although providers prescribed fewer PIMs during both time periods.
In a case-control study involving 42 physicians in primary care, the web-based Systematic Tool to Reduce Inappropriate Prescribing (STRIP), which linked with EMR and generated patient-specific advice based on clinical guidelines, was used to assist medication reviews of patients with polypharmacy. 49 Participants were asked to optimize medication regimens of two comparable patients; one in their usual manner (control) and one using the STRIP Assistant (case), with changes validated by an expert panel of two geriatrician pharmacologists. Inappropriate prescribing occurred in 42% of controls versus 24% of cases, while appropriate prescribing occurred in 76% of cases and 58% of controls (p < 0.001 for both comparisons).
Residential care
Experimental studies
In an RCT involving 813 patients, a CDSS linked to CPOE for 22 psychotropic medications which produced alerts to either avoid or decrease the dose made no difference to prescribing of PIMs. 50 This was despite the fact that more alerts were generated in the intervention than in the control group (4.8 versus 3.8 per 100 resident-months; RR = 1.27, 95% CI 1.01–1.59) and 8% of psychotropic medication orders were modified in response to an alert on intervention units compared with 2% of orders in control units (RR = 3.69, 95% CI 1.08–12.57).
In another RCT involving 833 residents, CDSS alerts for prescribing in patients with renal insufficiency were displayed to intervention prescribers but hidden though tracked for control prescribers. 51 Calculation of creatinine clearance used the Cockcroft–Gault equation, and recommendations in the alerts were directly related to specific levels of renal impairment for each drug, with 94 alerts being created for 62 drugs. Alerts were triggered when a physician initiated an order in the CPOE system for one of these medications in residents with renal insufficiency. Final orders for drugs to be avoided were submitted less often in the intervention units, 3.5 versus 5.2 per 1000 resident days in the control units (RR = 0.68; 95% CI 0.45–1.0). The most common drugs triggering alerts were levofloxacin, nitrofurantoin, cephalexin, metformin, gabapentin and glyburide.
Observational studies
In a before–after quasi-experimental study involving 265 residents seen by 42 clinicians, CPOE algorithms for detecting geriatric problems (falls, fever, pneumonia, urinary tract infections, osteoporosis) based on clinical practice guidelines were presented on screen to physicians through the CPOE system, with an array of diagnostic and treatment options and means to communicate with interdisciplinary teams. 52 Comparing 6 months before and after deployment, use of the system by clinicians was infrequent, and while among patients with falls there were trends toward reduced use of neuroleptics and sedative–hypnotics, no significant changes in prescribing were seen.
Factors impacting effectiveness of electronic-medical-record-linked clinical decision support systems
Designing CDSS that facilitate deprescribing of PIMs must take account of what end users perceive as useful and practical in real-world work settings. Many CDSS rely on providing alerts and prescribing aids or algorithms to prescribers as they order specific medications. The studies in our review and several others53–59 have highlighted factors that impact on the effectiveness of prescribing-related CDSS contained within CPOE systems. Automatic provision of recommendations early within the providers’ workflow at the time of prescribing,33,36 suggestions for alternative medications to substitute for PIMs, full integration with clinical and laboratory information systems, and requests for reasons for not following the recommendations are viewed positively. Prescribers dislike receiving alerts about information they are already well aware of, alerts that are repetitive because of the frequency of the condition among patients they see, or because the alert comes up every time they see particular patients, and receiving alerts claiming inappropriate prescribing when they have already made a decision to treat the patient in such a manner on the basis of a compelling indication which trumps risk of harm. 60 In one review of 23 studies describing 32 different alerts, drug–disease alerts attracted the greatest number of studies reporting positive effects on prescribing (five out of six studies) but none reported any impact on patient outcomes. 61 The seniority of the clinician receiving the alert also matters, in that junior doctors are less likely to heed an alert to cease a medication until they have consulted a senior colleague.32,62
Clinicians will often override e-prescribing alerts (between 49 and 96% 49 ) because of lack of specificity of the messages or irrelevance of the medication to the current drug regimen. Clinicians in focus groups have suggested suppressing alerts for renewals of medication combinations that patients are currently taking and tolerating, 32 as well as for alerts related to medications used for short-term courses of therapy. 41 Other suggestions include designing alerts with the use of colours so that clinicians can easily recognize the severity of the alert, increasing the specificity of alerts by allowing clinicians to set the desired alerting threshold, running drug alerts only on the medications that the patient is currently taking (i.e. an active medication list), and minimizing the number of clicks necessary when interacting with the system. Tiering drug–drug interactions according to severity has also improved compliance with alerts in hospital practice, with 100% compliance for severe alerts. 63 In hospitals, improved refinement of, and response to, PIM alerts may be achieved if those that are overridden are reviewed by a clinical pharmacist who then discusses the cases with the relevant prescriber, especially those that the pharmacist regards as at great risk of incurring ADEs, compared with appropriate overrides in critically ill patients. 64
Some of the more successful PIM reduction studies reported in this review have involved CDSS that suggest alternatives to PIMs based on physiological assessment such as renal function. Of note is the study by Awdishu and colleagues 33 in which prescribers were more responsive to ‘prospective alerts’ than to ‘look-back alerts’, suggesting that receiving advice at the time of initial prescribing maximizes CDSS effectiveness. Meaningful alerts require consideration of age, sex, weight, comorbidities, concomitant medications, measures of organ function, and, especially in older patients, assessment of frailty and life expectancy. 40 This necessitates full integration of EMR and associated CDSS with clinical and laboratory feeder systems. Integrated EMR systems with which clinicians have become highly familiar as a result of prolonged exposure and training also appear to be associated with more positive effects. 35 In the negative trial reported by Price and colleagues, 45 data quality probes highlighted incompleteness of data in EMR fields used for PIM reporting and the low use of decision supports, such as medical problem and medication lists. Focus groups highlighted the need for better integration of STOPP guidelines with prescribing workflows, with the authors cautioning policy makers not to expect better care from use of CDSS in the absence of ongoing review of data quality and improvement.
In summary, CDSS need to generate advice and alerts for the right patient at the right time with the right information to the right clinician who has authority and willingness to avoid PIM prescribing.
Discussion
Formal medication reviews and deprescribing are time and resource intensive, and are infrequently performed in clinical practice for several reasons. There may be underappreciation of the hazards of polypharmacy, clinical inertia, limited pharmacology knowledge or self-confidence in deprescribing, or limited time and necessary information about the particulars of individual patients. 65 The potential for these barriers to be overcome by EMR-enabled CDSS aimed at reducing the prescribing of PIMs is attractive, but is it being realized?
Our contemporary review of EMR-enabled CDSS in reducing prescribing of PIMs indicates the evidence base to date is limited, with relatively few RCTs, and very few that examined patient outcomes over the medium to long term versus medication-related process measures. Only five studies attempted to measure patient outcomes comprising falls, ADEs or injuries,34,37,38,42,43 of which only two38,43 reported a significantly positive effect. In part, small sample size, less than expected levels of PIM prescribing, lack of prioritization of alerts and recommendations, and low ADE rates may have been mitigating factors. 44 Longitudinal studies that assess outcomes such as rates of ADE, hospitalization, or mortality at 6 months or longer may also be needed to highlight patient-important effects over the longer term.
There was significant variation between studies in patient populations (although most involved older patients), type of CDSS, method of linkage with EMR, study designs and outcome measures. The studies also featured very few commercially available CDSS designed to reduce PIMs, 38 with most being locally developed in research centres or within single jurisdictions. These may not be transferable to other locales in the absence of considerable further in-house refinement. The fact that only 7 of 20 studies38,40,43,44,47,49,51 were conducted in sites or jurisdictions outside the US healthcare system further limits generalizability of results to other settings.
However, assuming minimal publication bias, the totality of evidence favours EMR-enabled CDSS as being effective in reducing the prescribing of PIMs in hospitals by up to 50%, but less effective in ambulatory care settings (up to 23%) and borderline effective in RACFs. Effects were more consistently positive in hospital settings (seven of eight studies32–38) compared with ambulatory care (four of eight studies40,43,47,49) and residential care (one of three studies 51 ) settings. Interventions involving more sophisticated CDSS which generated alerts and recommendations that took account of patient characteristics and targeted selected medications (psychoactive medications or medications dependent on renal clearance) or specific patient types (older patients receiving multiple medications or those with renal insufficiency)32–38,43,51 appeared to be more effective than CDSS that generated more generic recommendations relating to all PIMs (based on Beers and other criteria), irrespective of the clinical circumstances of individual patients.
While effects in absolute terms in most positive studies were modest, they suggest such interventions are feasible and acceptable to clinicians, and if certain design features are adhered to, there is potential for even greater impact. Compared with preventing drug ordering in the setting of a known contraindication such as drug allergy, reducing the rate of PIM ordering requires higher-level decision making. Disagreement over evidence of the benefits and harms of specific medications, pressure from colleagues or patients to prescribe, nonfamiliarity with principles of gerontological prescribing, poor clinician–patient communication, inadequate EMR/CDSS training, rapid clinician turnover, or other unforeseen reasons may have impacted studies reporting nil or marginal effects. 46 Nevertheless, several ongoing trials attest to the continued interest in developing better EMR-linked CDSS systems aimed at reducing PIMs66–68 and their results are eagerly awaited.
Our analysis is limited in not being a formal systematic review, although results were categorized according to clinical setting and methodological rigour. No meta-analysis was attempted due to the heterogeneity in study design and outcome measures. More systematic evidence syntheses are being planned by other investigators, 69 but in the meantime the current review serves as an indication of the state of the art for clinicians, CDSS designers and policy makers.
In conclusion, based on current evidence, EMR-enabled CDSS can reduce prescribing of PIMs in hospital practice, less so in ambulatory care, and minimally in RACFs. There is potential for more impact if the design and implementation of CDSS are more user friendly, more responsive to patient contexts in which prescribing occurs, and more selective and informative in the types of alerts and reminders generated.