
Abstract
Background:
The aim of this study was to determine the current magnitude and characteristics of intravenous patient-controlled analgesia (IV-PCA) errors, and to identify opportunities for improving the PCA modality.
Methods:
We conducted a descriptive analysis of IV-PCA medication errors submitted to the MEDMARX database. Events were restricted to those occurring in inpatient hospital settings between 1 January 2005 and 31 December 2015. IV-PCA errors were classified by error category, cause of error, error type, level of care rendered, and actions taken.
Results:
A total of 1948 IV-PCA errors were identified as potential errors (3.9%), nonharmful errors (89.5%), or harmful errors (6.7%) based on the National Coordinating Council for Medication Error Reporting and Prevention taxonomy for categorizing medication errors. Of these, 19.1% required a clinical intervention to address the deleterious effects of the error, indicating an underestimation of the risks associated with IV-PCA errors. The most frequent types of errors were improper dose/quantity (43.2%) and omission errors (19.9%). While human performance deficit was the leading cause of error (50.2%), other common causes included failure to follow procedure and protocol (42.2%) and improper use of the pump (22.7%). Although remedial actions were often taken to prevent error recurrence, actions were taken to rectify the systemic deficits that led to errors in only a minority of cases (11.8%).
Conclusion:
Preventable errors continue to pose unnecessary risks to patients receiving IV-PCA. Multimodal analgesic regimens and novel PCA systems that reduce human error are needed to prevent errors while preserving the advantages of PCA for the management of acute pain.
Introduction
Patient-controlled analgesia (PCA) is widely used to manage acute postsurgical pain.1,2 A recent hospital database analysis reported that approximately 25% of patients undergoing total knee/hip arthroplasty or open abdominal surgery received intravenous (IV)-PCA. 3 In 2004, an estimated 13 million patients received IV-PCA therapy for the management of postoperative pain in the United States (US). 2 Because PCA permits patients to self-administer small doses of an analgesic when needed, the PCA modality facilitates titration to the patient’s individual analgesic needs and yields higher patient satisfaction as well as better pain management.1,4,5
Numerous issues can undermine the safety of the IV-PCA modality. These include gaps in analgesic treatment due to infiltrated IV lines, 6 mobility constraints related to IV lines, 7 an increased risk of infection, 8 phlebitis,9,10 proxy dosing, 11 and harmful medication errors.2,12–17 All of these factors increase the risk of adverse events.2,12–19 In one study, errors involving PCA had a more than four-fold increased likelihood of leading to harm compared with other types of medication errors owing to inadvertent dosing, erroneous route of administration, and other causes. 14
Errors associated with IV-PCA also pose a substantial cost burden to the healthcare system. Using data from a voluntary error reporting database, Meissner and colleagues reported that 407 IV-PCA-related errors per 10,000 people occurred in the US in 2004, costing up to an additional $388 million in healthcare expenditures. 2 Despite recognition of the substantial clinical and economic consequences associated with IV-PCA medication errors in the literature, there is a limited understanding of the current risk of harm and root causes of these errors. The most recent studies of IV-PCA medication errors were conducted more than a decade ago.2,12–15,18,19 Since then, the landscape of PCA devices has evolved with the development of smart PCA pumps containing safety features (e.g. barcode scanners, drug library software, alert systems) designed to prevent medication errors.7,20 Additionally, general awareness of the need to prevent medication errors involving IV-PCA devices and other types of infusion pumps has increased over the past decade.21,22 As a result, new regulatory requirements have been enacted to address the risk of harm and medication errors associated with infusion pumps, such as the 2011 US Food and Drug Administration (FDA) Infusion Pump Improvement Initiative, which mandates additional safety requirements for manufacturers. 23
We anticipate that the above changes are likely to impact the prevalence of IV-PCA medication errors. However, the current extent and pattern of medication errors associated with IV-PCA use for the management of acute postoperative pain in hospital settings remains largely unknown. Therefore, to bridge this knowledge gap, we conducted a descriptive analysis of 2005–2015 MEDMARX data to investigate the current magnitude and characteristics of IV-PCA medication errors as well as opportunities for improving the PCA modality.
Materials and methods
Database
MEDMARX is a nationally recognized, patient de-identified, voluntary medication error reporting system that was designed and developed by the US Pharmacopeia in August of 1998.19,24 In 2004, the MEDMARX database was acquired by Quantros. 25 MEDMARX is regarded as the one of the largest databases of adverse drug events in the US, with over 870 participating hospitals and related healthcare systems reporting 1.3 million medication errors as well as 40,000 adverse drug reaction records as of 2005.14,19 Notably, the number of MEDMARX participating hospitals has decreased since 2005, allowing a characterization of the types of medication errors but not the trend of errors over the study period. MEDMARX data for this study was provided by Quantros as a de-identified dataset. Thus, this study was exempt from approval by an ethics committee.
Eligibility criteria and event selection
For this study, we selected IV-PCA opioid analgesic medication errors occurring in inpatient hospital settings that were submitted to the MEDMARX database between 1 January 2005 and 31 December 2015. We restricted our analyses to errors associated with the management of acute postoperative pain. The unit of analysis was independent IV-PCA error events reported to MEDMARX.
Characteristics of medication errors
MEDMARX collects medication error event data in a standardized format using a series of required and optional fields. Most fields contain a list of possible selections (i.e. a pick list) to guide the reporter to document specific information. MEDMARX uses the National Coordinating Council for Medication Error Reporting and Prevention (NCC MERP) taxonomy to classify medication errors by severity. This taxonomy includes nine categories (categories A–I) 26 that reflect whether an actual error occurred (actual error, categories B–I) or not (potential error, category A), whether the error reached the patient (categories C–I) or not (categories A–B), and whether the error resulted in harm to the patient (harmful error, categories E–I) or not (nonharmful error, categories A–D). We excluded potential errors (category A) from the nonharmful error group in order to differentiate nonharmful errors that actually occurred (categories B–D) from nonharmful errors that may or may not have occurred (categories A–D). Therefore, nonharmful errors in this study refer to actual errors that were not associated with harm (categories B–D).
The MEDMARX system also has fields for describing the nature of an error including node (phase) of the medication process (i.e. the stage in the medication use process during which the error occurred, including prescribing, transcribing, dispensing, and administering stages), type of error, cause of error, contributing factors, and level of care provided to the patient as result of the error. Each medication error event (identified by a unique identifier) can have multiple entries or rows for certain variables such as type of error, cause of error, contributing factors, level of care rendered, and actions taken. Therefore, some errors were associated with multiple causes, contributing factors, or actions taken. In contrast, certain variables such as staff associated with the error, NCC MERP index category, and node of the medication process were documented as single entries per event.
Statistical analyses
Descriptive analyses were performed to determine the frequencies and characteristics of IV-PCA errors reported during the study period. Chi-square tests were conducted with significance assessed at p < 0.05 to compare frequencies between harmful and nonharmful errors. All data were analyzed using SAS® version 9.4 (SAS Institute, Inc., Cary, NC, USA).
Results
A total of 92,090 errors associated with opioid analgesics were reported to the MEDMARX database by 632 facilities between 1 January 2005 and 31 December 2015. Of these, 1948 errors (2.1%) reported by 168 inpatient hospital facilities were associated with IV-PCA. Figure 1 illustrates the IV-PCA error selection process.
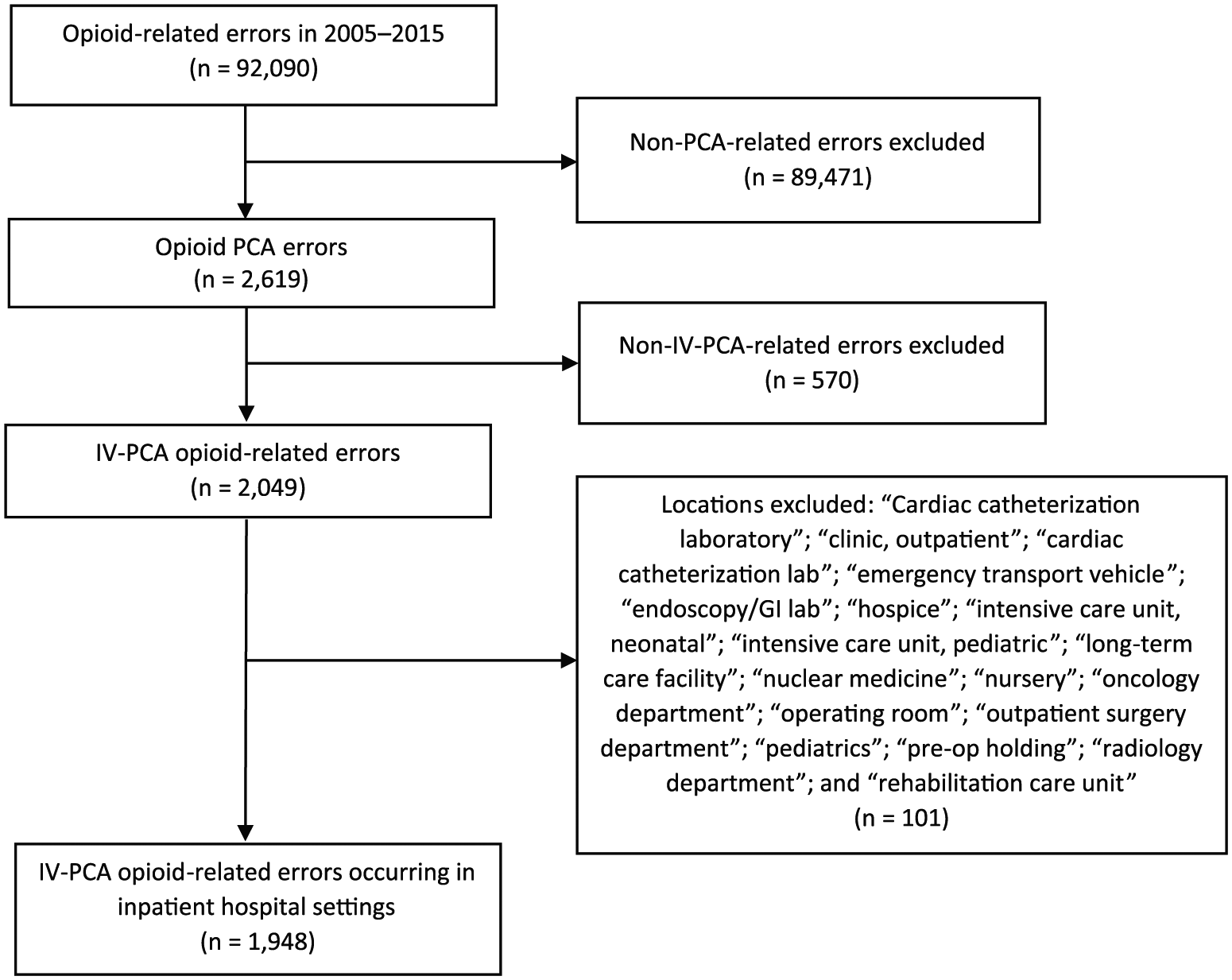
Schematic for event selection in the MEDMARX database.
Demographics: facility and patient characteristics
Most facilities reporting to MEDMARX were either general community hospitals or university hospitals, and a majority had a 100–499-bed capacity. Although only 10.7% of facilities reporting IV-PCA errors to MEDMARX were university hospitals, these types of hospitals were disproportionately represented in the data set for this study, reporting 42.3% of errors associated with IV-PCA (Table 1).
Characteristics of facilities reporting IV-PCA medication errors to MEDMARX during the study period, 2005–2015.
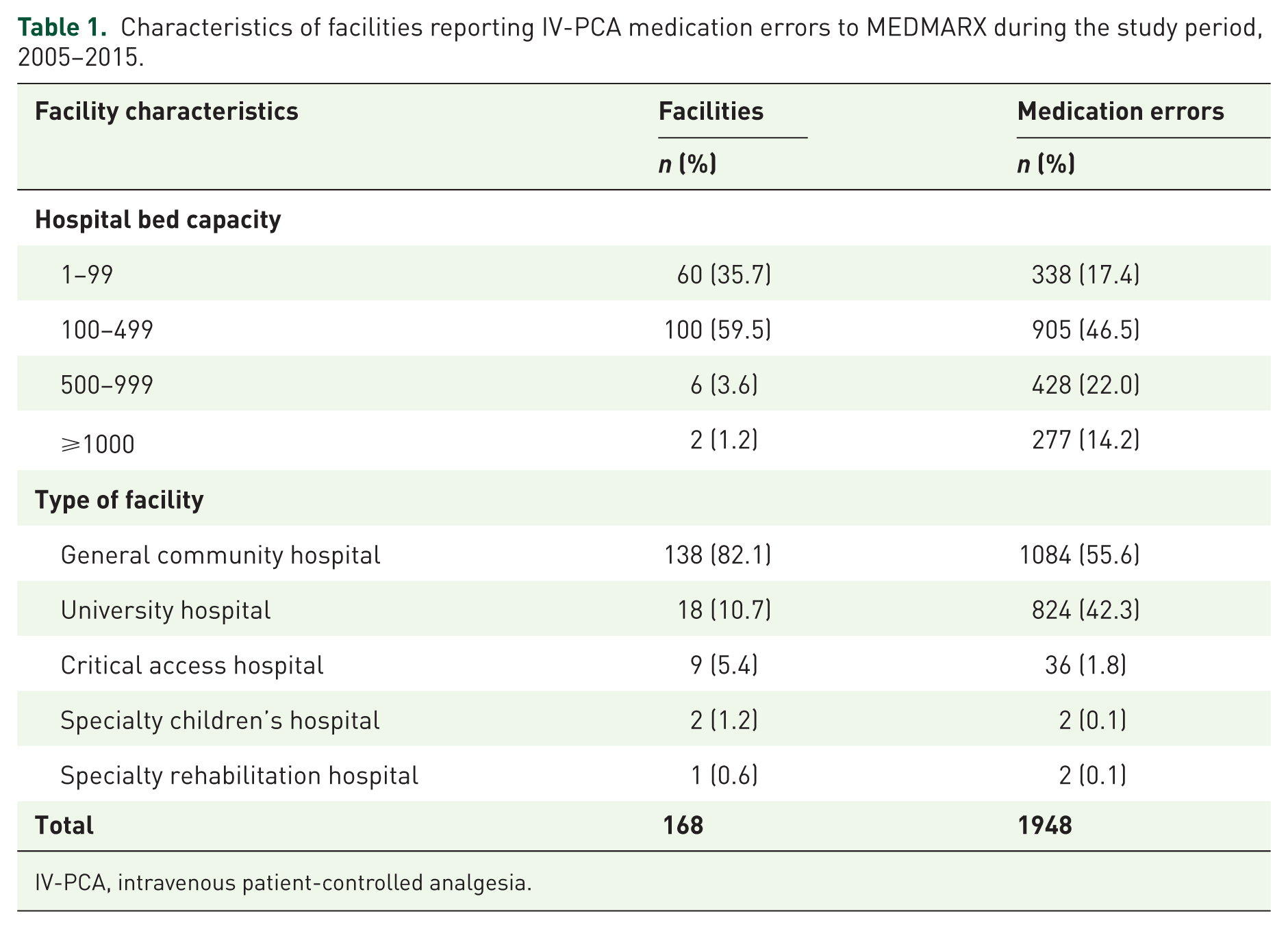
IV-PCA, intravenous patient-controlled analgesia.
IV-PCA errors were reported in all age groups, with a majority of harmful (43.8%) and nonharmful (41.6%) errors occurring in patients aged 40–64 years. For errors where patient sex was available, 55.0% of errors were reported in female patients, and this was consistent across harmful and nonharmful errors (Supplementary Table 1).
NCC MERP index for classification of IV-PCA errors
A majority of IV-PCA errors (1873 errors, 96.1%) were actual errors compared with the 3.9% that were potential errors (Figure 2). Most (71.0%) IV-PCA errors reached the patient (categories C–I), while 29.0% did not (categories A and B). Based on the severity of harm associated with an error, 89.5% of IV-PCA events were rated as nonharmful errors (categories B–D) and 6.7% were rated as harmful (categories E–I). None of the errors contributed to or resulted in permanent harm (category G).
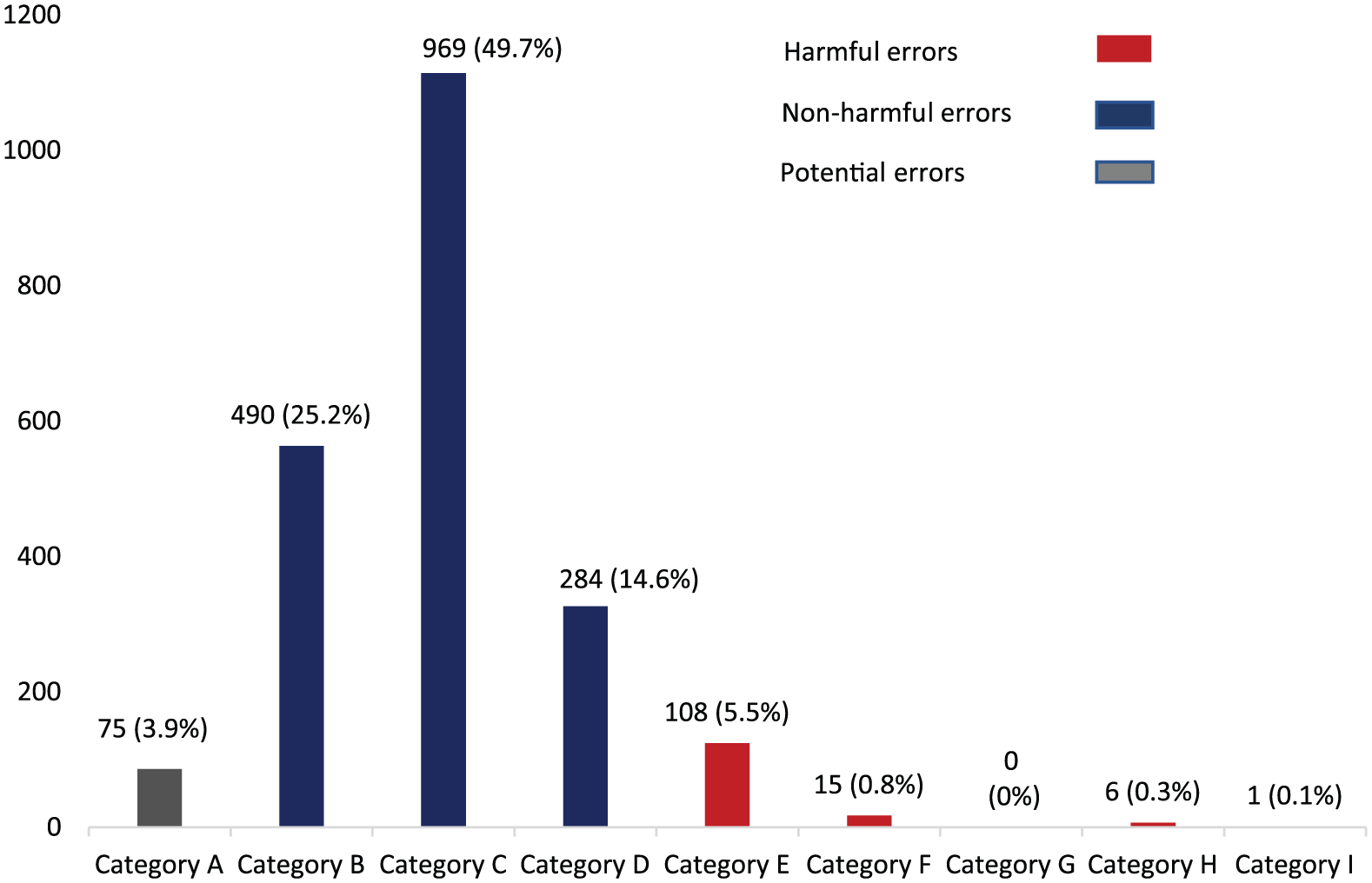
Distribution of IV-PCA errors reported to MEDMARX based on NCC MERP index classification (n = 1948).
Node of error in the medication use process
Among actual IV-PCA errors (n = 1873), more than half (55.2%) occurred during drug administration. We cross-tabulated medication process node by error severity and found that, compared with nonharmful errors, harmful errors more frequently (p < 0.05) occurred during medication administration and prescription; in contrast, nonharmful errors occurred more frequently (p < 0.05) than harmful errors during medication dispensing and transcription/documentation (Table 2).
Distribution of severity of actual IV-PCA errors by node in the medication use process (n = 1873).
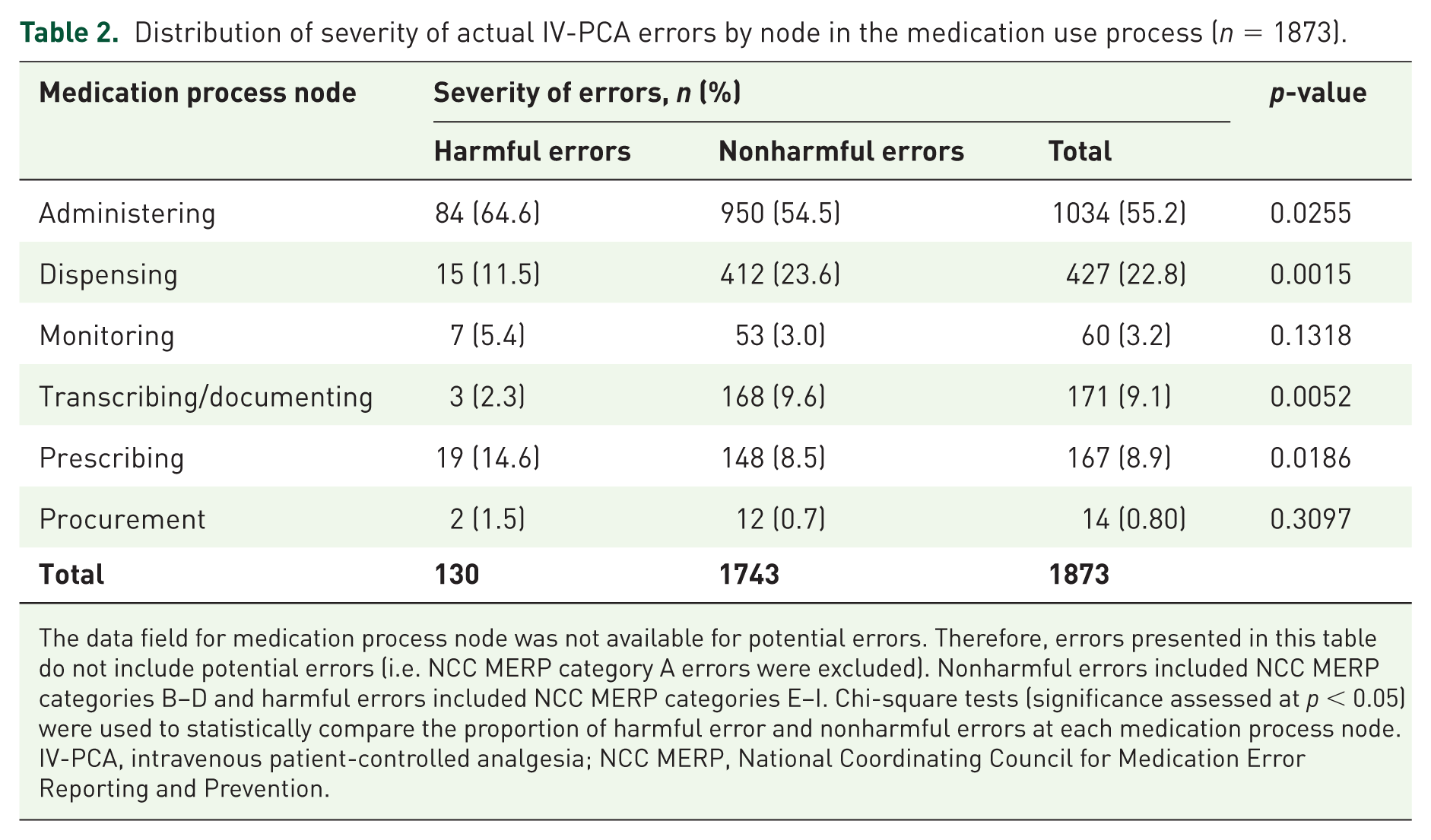
The data field for medication process node was not available for potential errors. Therefore, errors presented in this table do not include potential errors (i.e. NCC MERP category A errors were excluded). Nonharmful errors included NCC MERP categories B–D and harmful errors included NCC MERP categories E–I. Chi-square tests (significance assessed at p < 0.05) were used to statistically compare the proportion of harmful error and nonharmful errors at each medication process node.
IV-PCA, intravenous patient-controlled analgesia; NCC MERP, National Coordinating Council for Medication Error Reporting and Prevention.
Type of error
Among 1873 actual errors, the most frequent type of error identified was improper dose/quantity (43.2%), defined as any dose, strength, or quantity of vials differing from the prescribed dose or strength (Table 3). Other common types of errors were omission error (19.9%), unauthorized or wrong drug, (12.2%), prescribing error (9.4%), wrong administration technique (8.0%), and wrong time (7.8%). Omission error is defined as failure to administer an ordered dose; this excluded patient refusal, clinical decision not to administer (contraindication), and other reasons (e.g. patient sent for testing). An unauthorized/wrong drug error occurred when medication that was not authorized by a legitimate prescriber was dispensed or administered. Wrong administration technique is defined as the use of an inappropriate/improper technique to administer a drug, including incorrect activation of a drug administration system.
Distribution of error types associated with actual IV-PCA events by error severity in the MEDMARX database (n = 1873).
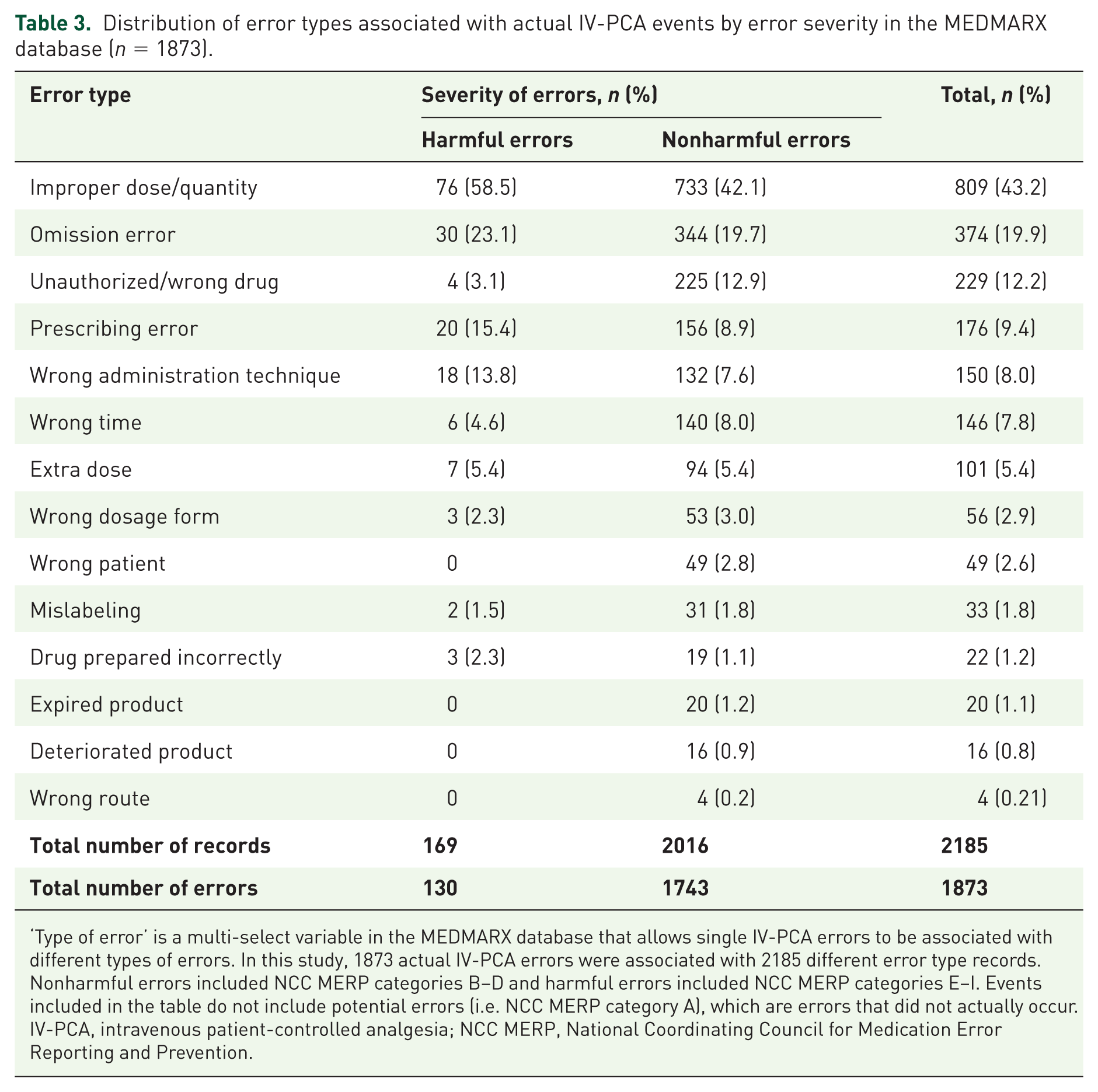
‘Type of error’ is a multi-select variable in the MEDMARX database that allows single IV-PCA errors to be associated with different types of errors. In this study, 1873 actual IV-PCA errors were associated with 2185 different error type records. Nonharmful errors included NCC MERP categories B–D and harmful errors included NCC MERP categories E–I. Events included in the table do not include potential errors (i.e. NCC MERP category A), which are errors that did not actually occur.
IV-PCA, intravenous patient-controlled analgesia; NCC MERP, National Coordinating Council for Medication Error Reporting and Prevention.
Cause of error
Performance (human) deficit was the most frequent cause of error (50.2%; Table 4). Other frequent causes were procedure/protocol not followed (42.2%), computer-related error (36.5%), improper use of the pump (22.7%), and improper dosage and quantity (19.2%). Pump or equipment failure was the cause of error in 4.2% of cases.
Distribution of cause of error for actual IV-PCA events by error severity in the MEDMARX database (n = 1873).
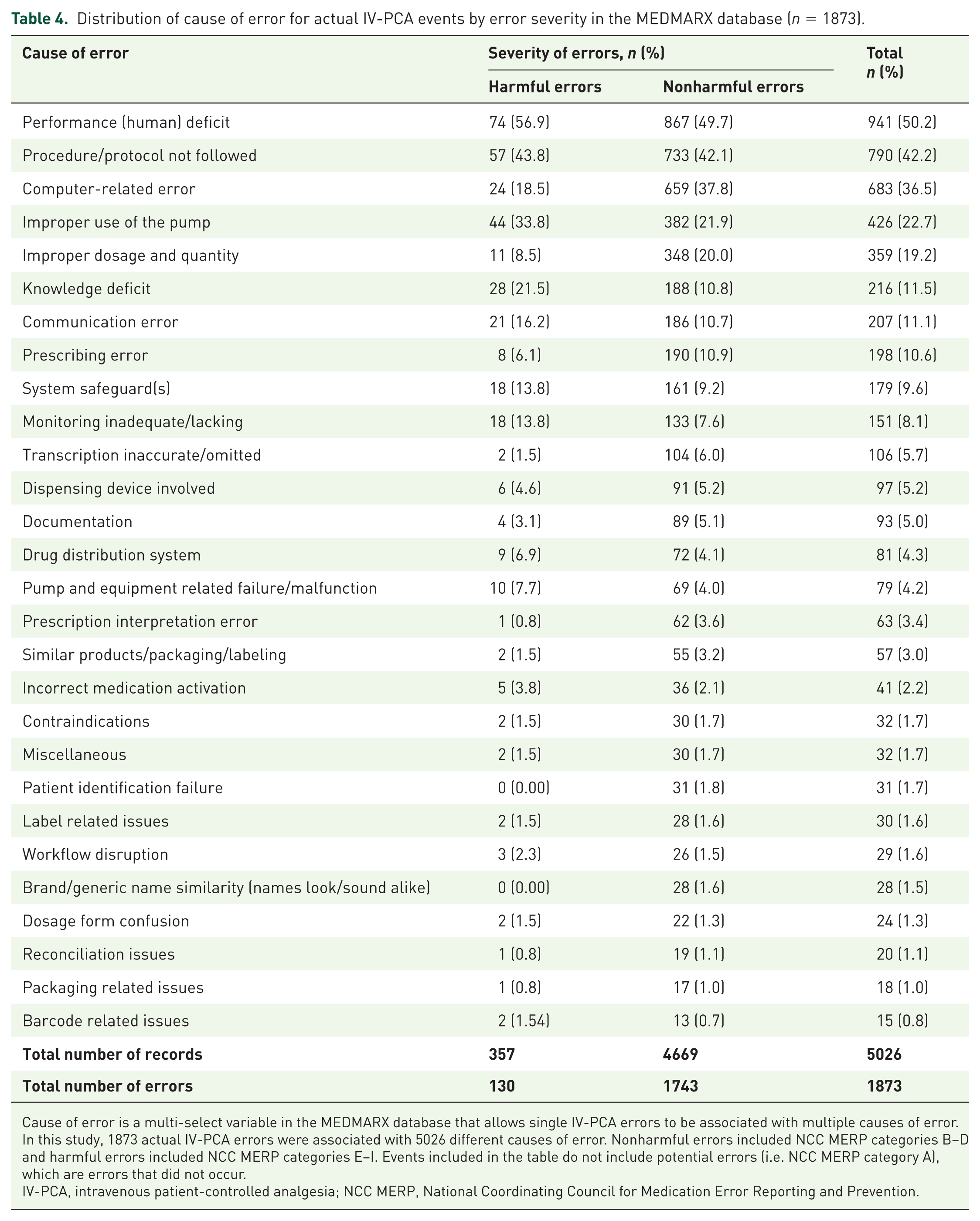
Cause of error is a multi-select variable in the MEDMARX database that allows single IV-PCA errors to be associated with multiple causes of error. In this study, 1873 actual IV-PCA errors were associated with 5026 different causes of error. Nonharmful errors included NCC MERP categories B–D and harmful errors included NCC MERP categories E–I. Events included in the table do not include potential errors (i.e. NCC MERP category A), which are errors that did not occur.
IV-PCA, intravenous patient-controlled analgesia; NCC MERP, National Coordinating Council for Medication Error Reporting and Prevention.
Contributing factors
Data on contributing factors were only available for actual errors (i.e. potential errors were excluded). For 72.4% of IV-PCA errors, the contributing factors were absent (40.5%) or could not be determined (31.9%) (Figure 3). Among events with known contributing factors, staff-related factors such as staff inexperience, distractions, increased workload, fatigue, shift changes, insufficient staff, temporary staff, staff floating, and cross-coverage were the leading factors contributing to IV-PCA errors. These staff-related factors were implicated in 31.2% of actual IV-PCA events reported to MEDMARX during the study period.
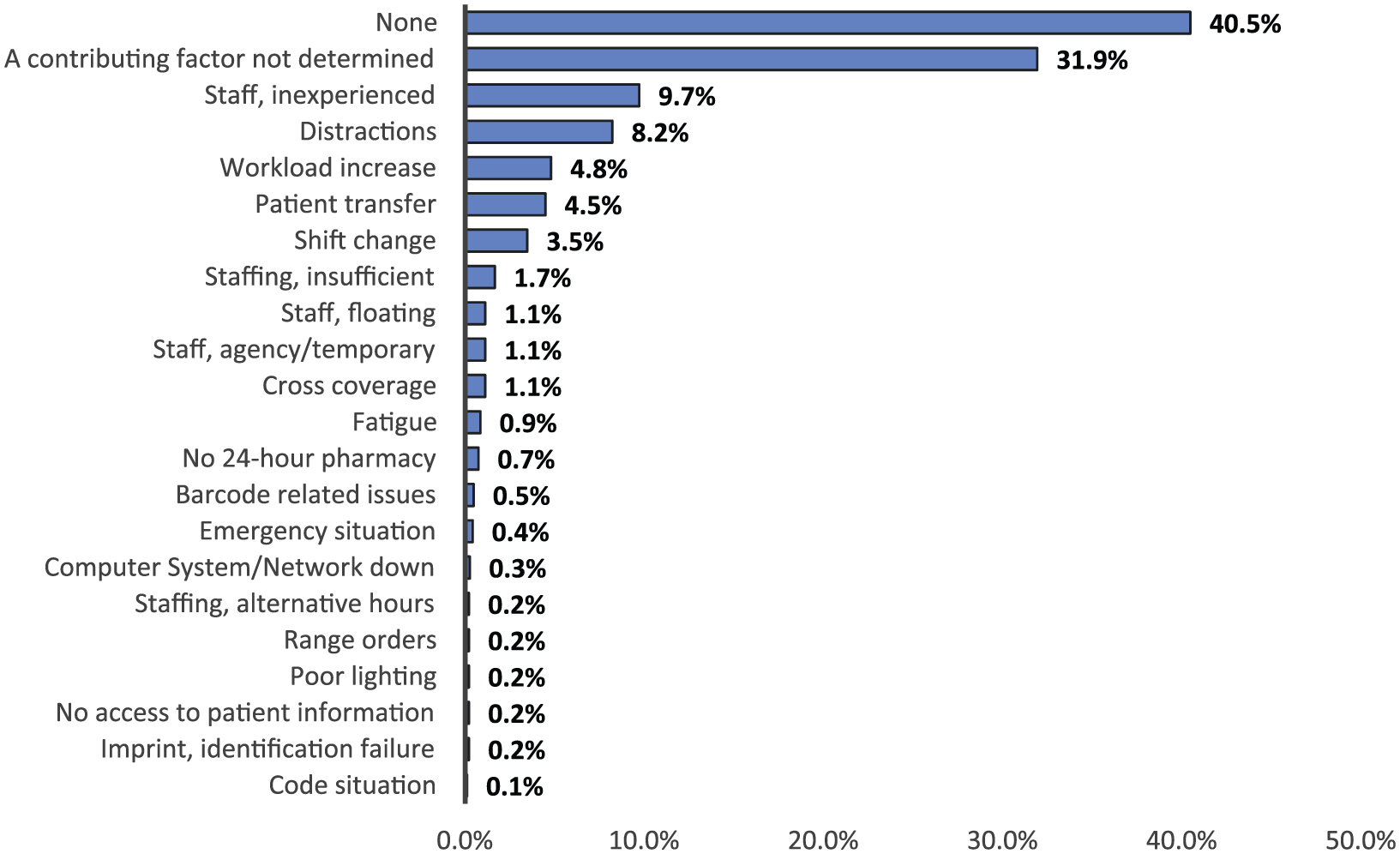
Distribution of factors contributing to actual IV-PCA events in the MEDMARX database (n = 1873).
Action taken
Remedial actions were often taken to address or prevent the recurrence of an error. Our analyses indicated that various remedial actions were taken in response to 92.6% of the 1948 IV-PCA errors reported to MEDMARX (Figure 4). The most frequently used strategy for preventing error recurrence was informing the staff member who was responsible for the initial error (46.5%) or those who were otherwise involved with the error (22.0%). Other common strategies included: informing the physician, providing training, and improving communication processes. Notably, remedial actions were directed towards the specific error or personnel involved in the error in a majority of cases, whereas remedial actions were directed towards the systemic deficits that led to the error in a minority of cases (11.8%). Examples of the latter such actions were enhanced communication processes, changes in policy or procedure, modification of staffing practices or policy, and implementations of new policies or procedures.
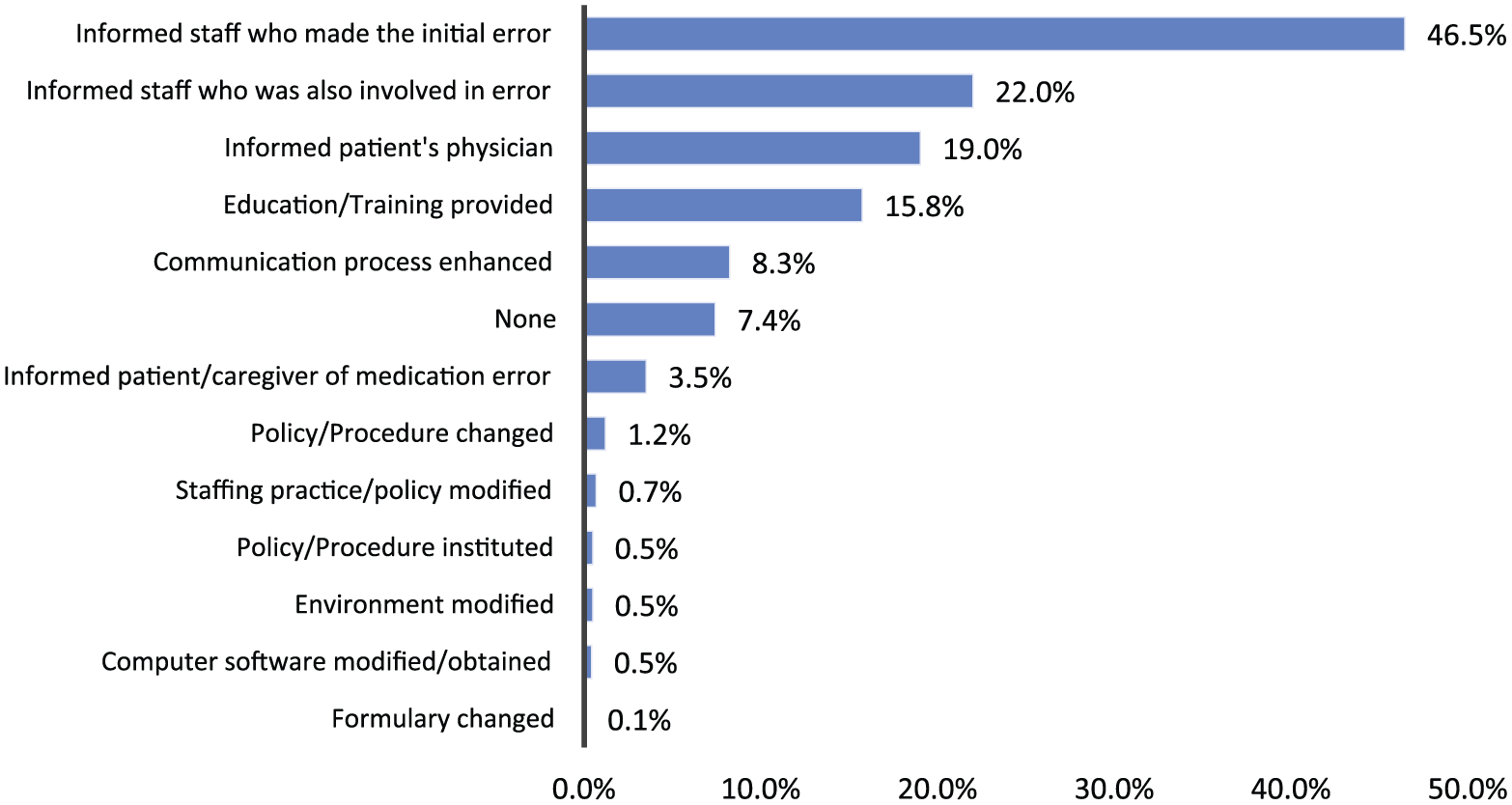
Remedial actions taken to prevent the recurrence of IV-PCA events in the MEDMARX database (n = 1948).
Level of care
Some level of intervention is often provided to patients in order to prevent or reverse the harmful effects of a medication error. In our dataset, no care was provided (42.7%) or information on the level of care could not be determined (16.6%) for 819 (59.2%) of 1383 errors that reached patients (Figure 5). For the remaining 564 errors, emergency care such as the administration of oxygen, cardiopulmonary resuscitation (CPR), cardiac defibrillation, or a narcotic antagonist intended to sustain life or address a serious or fatal complication was provided in 372 cases (66.0%), while further examination and monitoring was implemented to prevent serious complications following an error in 192 cases (34.0%). Table 5 illustrates the distribution of intervention types initiated for 1383 IV-PCA errors that reached patients (each error event was eligible for association with more than one unique intervention). The results indicated that a substantial amount of IV-PCA medication errors resulted in life-threatening situations. Interestingly, 77.7% of the 564 errors requiring an intervention to specifically address or prevent further serious complications were classified as nonharmful errors based on the NCC MERP taxonomy.
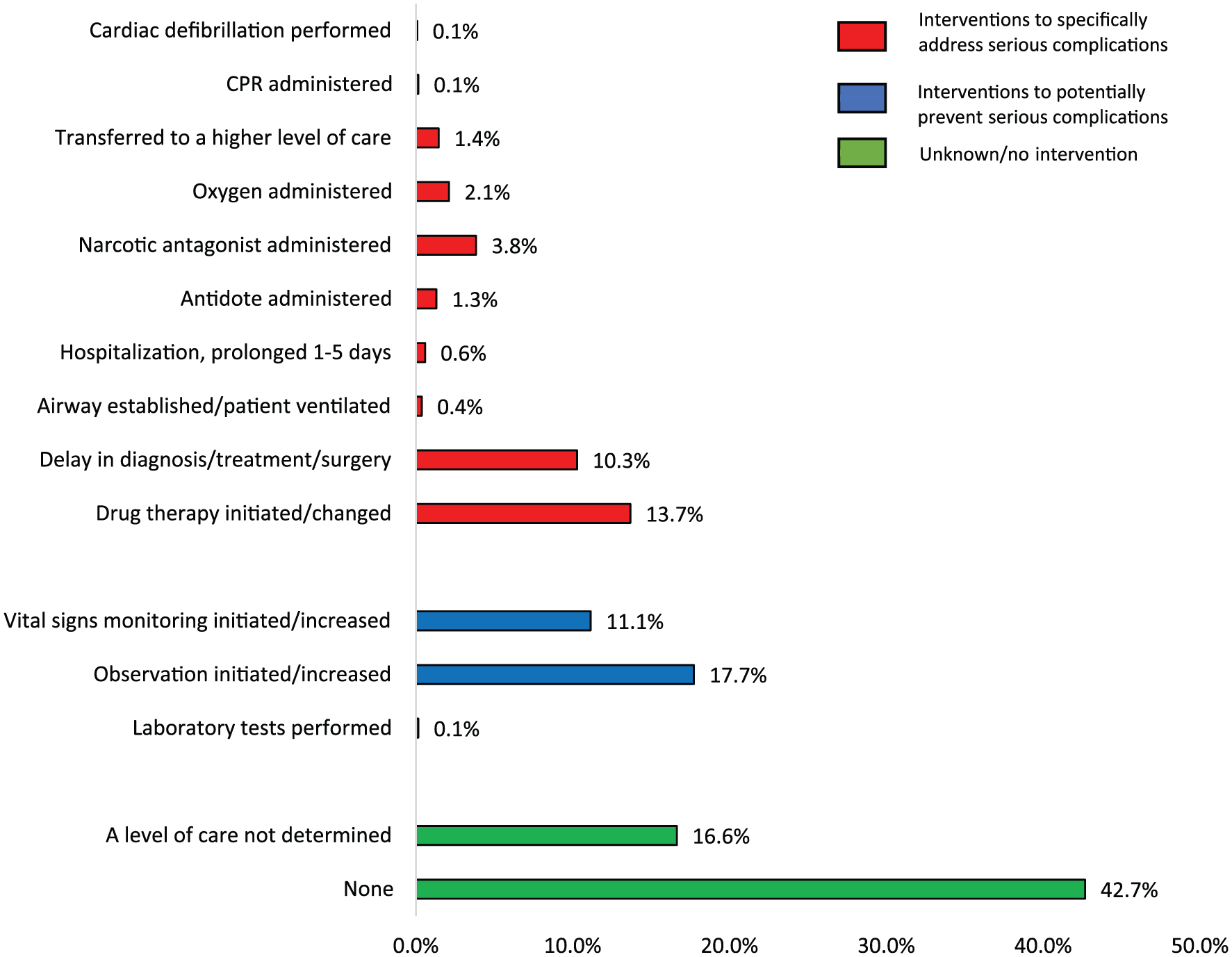
Level of care associated with IV-PCA events that reached patients in the MEDMARX database (n = 1383).
Error result on level of care rendered to the patient by error severity (n = 1383).
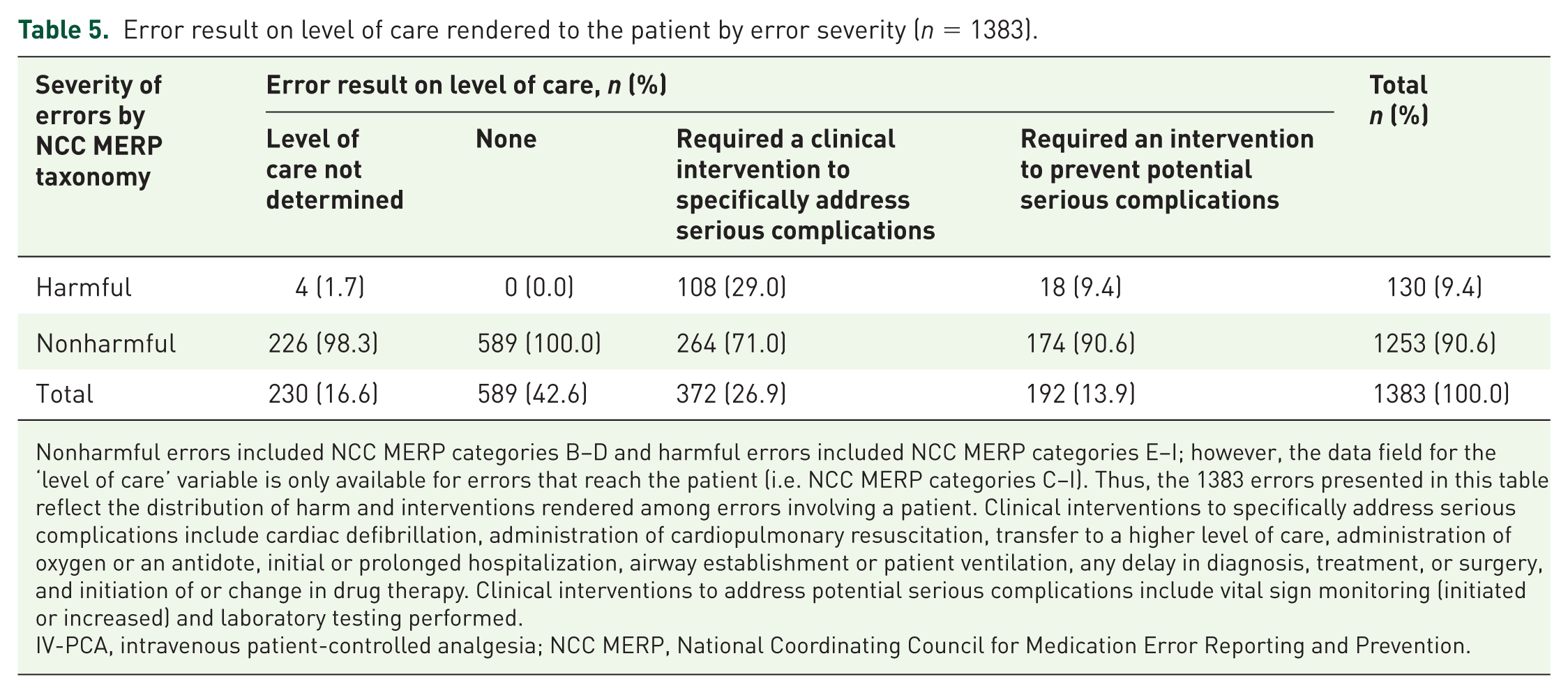
Nonharmful errors included NCC MERP categories B–D and harmful errors included NCC MERP categories E–I; however, the data field for the ‘level of care’ variable is only available for errors that reach the patient (i.e. NCC MERP categories C–I). Thus, the 1383 errors presented in this table reflect the distribution of harm and interventions rendered among errors involving a patient. Clinical interventions to specifically address serious complications include cardiac defibrillation, administration of cardiopulmonary resuscitation, transfer to a higher level of care, administration of oxygen or an antidote, initial or prolonged hospitalization, airway establishment or patient ventilation, any delay in diagnosis, treatment, or surgery, and initiation of or change in drug therapy. Clinical interventions to address potential serious complications include vital sign monitoring (initiated or increased) and laboratory testing performed.
IV-PCA, intravenous patient-controlled analgesia; NCC MERP, National Coordinating Council for Medication Error Reporting and Prevention.
Next, we conducted a subgroup analysis of errors requiring interventions to specifically address serious or fatal complications (n = 372) against error type and error cause. The types of errors most commonly associated with the necessitation of an intervention were improper dose (48.4%), omission error (28.5%), prescribing error (9.7%), wrong administration technique (9.1%) and wrong time (9.1%) (Supplementary Table 2). Additionally, performance (human) deficit (57.4%), procedure/protocol not followed (43.8%), and improper use of the pump (33.1%) were leading causes of errors associated with necessitation of an intervention (Supplementary Table 3).
Personnel associated with the error
Nursing staff (60.3%) were the personnel most commonly associated with IV-PCA errors, followed by pharmacists (24.5%) and physicians (8.6%) (Figure 6). Of note, physician-related error was associated with the only reported IV-PCA error that caused a death during the study period.
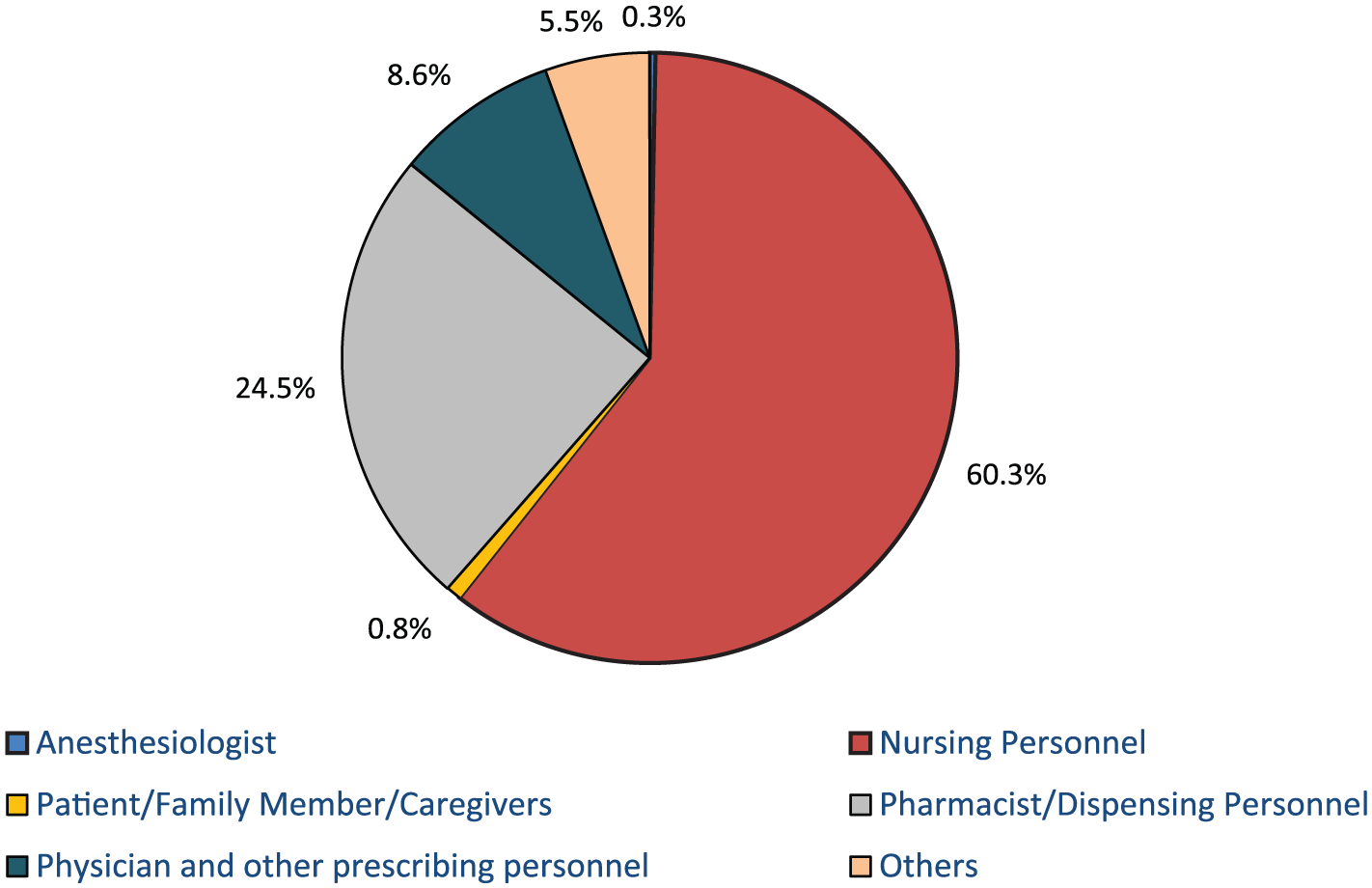
Staff involved with actual IV-PCA events in the MEDMARX database (n = 1873).
Type of opioid
The opioids most commonly associated with IV-PCA errors were hydromorphone (47.4%), morphine (38.2%), and fentanyl (9.9%). Hydromorphone and morphine accounted for 93.9% of harmful IV-PCA errors during the study period (Supplementary Table 4).
Location of the error
A majority of IV-PCA errors occurred on the hospital floor (61.9%). Similarly, hospital floors (72.3%) and admitting/pharmacy units (10.8%) were the two locations most commonly associated with harmful IV-PCA errors (Table 6). Improper dose/quantity was the most common error type in hospital locations except for admitting/pharmacy units, where omission error and wrong time were the most common error types (Supplementary Table 5).
Location by the severity of errors reported to the MEDMARX database (n = 1948).
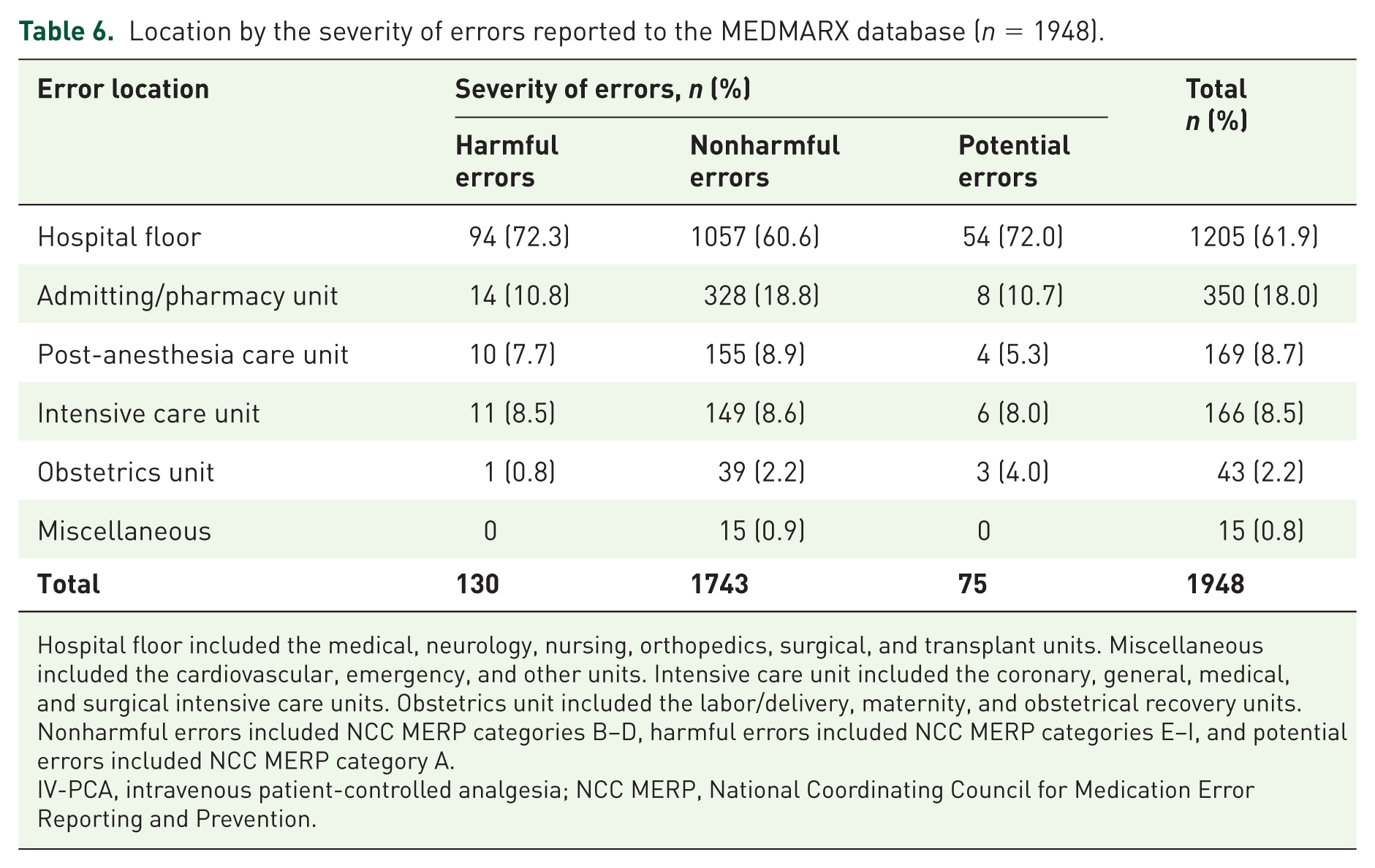
Hospital floor included the medical, neurology, nursing, orthopedics, surgical, and transplant units. Miscellaneous included the cardiovascular, emergency, and other units. Intensive care unit included the coronary, general, medical, and surgical intensive care units. Obstetrics unit included the labor/delivery, maternity, and obstetrical recovery units. Nonharmful errors included NCC MERP categories B–D, harmful errors included NCC MERP categories E–I, and potential errors included NCC MERP category A.
IV-PCA, intravenous patient-controlled analgesia; NCC MERP, National Coordinating Council for Medication Error Reporting and Prevention.
Discussion
In the present study, we utilized real-world data from the 2005–2015 MEDMARX database to assess the extent and characteristics of IV-PCA-related medication errors as well as opportunities for the improvement of IV-PCA devices. Similar to previous studies using the MEDMARX database and published recommendations on medication error classification, we used the NCC MERP taxonomy to categorize IV-PCA errors into harmful and nonharmful errors.12–14,18,19,26,27 Based on the NCC MERP taxonomy, 6.7% of IV-PCA errors reported to MEDMARX were harmful errors. Hicks and colleagues 14 similarly reported a 6.5% incidence of harmful errors among PCA-related errors submitted to the MEDMARX database between 2000 and 2004. Yet, based on the level of care rendered in response to errors, 19.1% of all 1948 IV-PCA errors in our study were harmful and necessitated cardiac defibrillation, CPR, airway ventilation, administration of a narcotic antagonist, or transfer to a higher level of care. A substantial difference between the magnitude of errors warranting clinical interventions and that of harmful events based on the NCC MERP taxonomy (19.1% versus 6.7%) suggests a substantial misclassification bias in the MEDMARX database. Upon further investigation, we found that 13.5% of all IV-PCA errors identified in our study were classified as nonharmful by the NCC MERP index despite association with a clinical intervention to prevent serious complications. Misclassification of harmful IV-PCA errors was also reported in a similar study by Lawal and colleagues. 28 Taken together, these findings indicate that harmful IV-PCA errors are common and frequently lead to adverse outcomes warranting additional care and healthcare resource utilization.
Although medication errors can originate at any node (phase) in the medication use process, many studies have reported that IV-PCA errors are most likely to occur during drug administration.14,29,30 Consistent with the literature, we observed that almost two-thirds of harmful IV-PCA errors occurred during the administration phase. The administration node is the last phase that involves drug, the administrator, and the patient simultaneously. Errors that occur in this phase are less likely to be detected and prevented than errors in other phases, and are more likely to reach the patient and produce harm.29–32
Improper dose or quantity was the leading type of IV-PCA error reported to MEDMARX and was implicated in more than half of harmful IV-PCA errors. Considering that IV lines allow the direct delivery of opioids into the bloodstream, there is a higher risk of adverse drug reactions such as opioid-induced respiratory depression and other serious complications at higher doses.31–36 Improper dose/quantity was associated with nearly half (47%) of opioid-related adverse events and deaths between 2004 and 2011 as reported to the Joint Commission’s Sentinel Event database. 37 Our study and others12–14 indicate that errors such as improper dose capable of undermining the intent and safety goal of IV-PCA remain prevalent.
Performance (human) deficit was the leading cause (50.2%) of IV-PCA events in our study, suggesting that health professionals who were adequately trained and educated still committed errors. However, examination of the factors contributing to IV-PCA errors indicated that multidimensional issues stemming from systemic deficiencies (e.g. staff inexperience, inevitable distractions or fatigue related to long working hours, and insufficient staff) rather than solely staff-related issues were the root causes of all IV-PCA errors with a known contributing factor. Unfortunately, facilities reporting errors to MEDMARX frequently performed personnel-specific remedial actions such as informing the staff member who was responsible for the initial error (46.5%) or those who were otherwise involved with the error (22.0%) and rarely initiated interventions to correct the systemic deficits that contributed to errors. We report that in only a minority (11.8%) of cases did reporting institutions initiate remedial actions to address systemic deficits that led to IV-PCA errors. Our findings emphasize the importance of addressing systemic deficiencies and health system processes that lead to errors; this might be facilitated by the assembly of interdisciplinary teams to address systemic deficiencies. This ‘systems approach’ has been advocated previously by the Institute of Medicine and the Institute for Safe Medication Practices.38,39
The literature consensus is that medication errors are largely preventable.30,40,41 Our findings corroborate this view, as a majority of the common types and causes of IV-PCA errors in our analysis are preventable. Collectively, the present results suggest that interventions targeting frequently occurring types and causes of IV-PCA errors, especially during the drug administration phase, may prevent harmful events associated with IV-PCA use. An effective strategy to decrease errors may be the improved use of technology. 16 Interventions incorporating technological safety features (e.g. computerized physician order entry, preprogrammed drug libraries) have been successfully used to decrease the incidence of IV medication errors including those occurring during drug administration.31,32,35,42–46 Yet, there remains an unmet need for novel PCAs with enhanced safety features. For example, non-IV routes of PCA administration may prevent common issues such as IV line infiltration or leakage that can disrupt analgesic delivery and lead to the inadequate management of postoperative pain. In a study by Panchal and colleagues 6 IV line infiltration was identified as the most common factor contributing to a 12% analgesic gap rate observed with IV-PCA. Lastly, the use of biometric or radiofrequency identification in PCA devices can potentially prevent the dispensing of opioids to the wrong patient and PCA proxy dosing.
The present study had some limitations. Like other voluntary reporting systems, MEDMARX is inherently prone to underreporting; it is estimated that only 1.2–7.7% of errors are reported to error reporting databases. 2 Additionally, MEDMARX is only available to participating hospitals that are contracted to report medication errors to the MEDMARX program. Accordingly, <3% of hospitals in the US contributed to the MEDMARX database during our study period, indicating that events described in this study are not necessarily representative of all IV-PCA-related errors occurring in the US. If we extrapolate the number of errors requiring specific clinical interventions to address harm (n = 372) using error reporting rates (1.2%) and the proportion of hospitals in the US that reported errors to MEDMARX during the study period (3%), up to 1.03 million harmful errors (372 ÷ 1.2% × 3%) involving IV-PCA are predicted to have occurred in the US over our 11-year study period.
Also, other events occurring during the study period may have been captured by other medication error reporting databases such as the US FDA Manufacturer and User Facility Device Experience (MAUDE) database, which is a repository for suspected device-associated deaths, serious injuries, and malfunctions submitted by manufacturers, importers, facilities, and voluntary reporters (e.g. healthcare professionals and patients).28,47 Additionally, since the acquisition of MEDMARX by Quantros in 2008, there has been a systematic decline in the number of facilities reporting opioid-related medication errors to the database. This decline may have led to an underestimation of the number of errors reported.
Voluntary reporting systems are also susceptible to reporting bias, with certain types of errors being more or less likely to be reported, influenced by the method of data collection or stimulated by publicity, litigation, or, as in this case, new regulatory requirements such as the US FDA Infusion Pump Improvement Initiative introduced in 2010. 48 We do not believe that the results of this study were affected by over-reporting stimulated by the Infusion Pump Improvement Initiative or other related regulatory changes, as the characteristics and magnitude of harmful and nonharmful errors identified by the NCC MERP taxonomy in the present study are similar to those reported by previous studies utilizing MEDMARX database data prior to 2010.12–15,17–19
Finally, we were unable to determine the rate of IV-PCA medication errors in our study, as information on the total number of patients receiving PCA was unavailable. We were similarly unable to determine causality or estimate other types of IV-PCA errors reported in literature such as proxy dosing and analgesic gaps, as this information was unavailable in the MEDMARX database.
Despite these limitations, to our knowledge, this study is the longest and most recent epidemiologic study investigating IV-PCA medication errors to date. Additionally, the use of ‘level of care’ rendered as a proxy of severity sheds new light on the reporting bias of severe outcomes and the underestimation of harm associated with IV-PCA errors by the NCC MERP taxonomy in MEDMARX.
Conclusion
Although largely preventable, harmful errors involving IV-PCA continue to occur in US hospitals. A considerable proportion of IV-PCA errors in this study required clinical intervention to address or prevent deleterious effects. Most errors occurred during drug administration and commonly involved improper dose or quantity, omission errors, and the use of unauthorized or wrong drugs. Patient safety must remain a priority as the regulatory requirements and guidelines surrounding IV-PCA continue to evolve. Concerted efforts should be made to improve safety surveillance systems, enhance staff training, increase hospital system initiatives, and promote the development of novel PCA systems with enhanced safety features designed to circumvent errors in order to provide the greatest safety and comfort to patients with acute postoperative pain.
Supplemental Material
MedMarx_Manuscript_Supplemental_Tables – Supplemental material for Medication errors involving intravenous patient-controlled analgesia: results from the 2005–2015 MEDMARX database
Supplemental material, MedMarx_Manuscript_Supplemental_Tables for Medication errors involving intravenous patient-controlled analgesia: results from the 2005–2015 MEDMARX database by Maitreyee Mohanty, Oluwadolapo D. Lawal, Margie Skeer, Ryan Lanier, Nathalie Erpelding and Nathaniel Katz in Therapeutic Advances in Drug Safety
Footnotes
Compliance with ethical standards
MEDMARX data for this study were provided by Quantros as a de-identified dataset. Thus, this study was exempt from approval by an ethics committee.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by AcelRx Pharmaceuticals, Redwood City, California, USA.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Supplemental material
Supplementary material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.