
Abstract
Objective
The efficacy and side-effects of nefopam were prospectively compared with those of fentanyl for patient-controlled analgesia (PCA) following cardiac surgery.
Methods
Patients scheduled to undergo cardiac surgery were randomly assigned between three PCA groups (nefopam, fentanyl or nefopam + fentanyl). Pain was assessed at rest and during movement at 12, 24, 36, 48 and 72 h after surgery using a visual analogue scale (VAS). Total infused PCA volume, number of rescue drug injections, duration of intubation and length of stay in the intensive care unit were recorded. The incidence of adverse effects was noted at 48 h postoperatively.
Results
There were no significant between-group differences in VAS score, total PCA infusion volume or number of rescue injections (n = 92 per group). Nausea was significantly more common in the fentanyl group compared with both other groups.
Conclusions
PCA with nefopam alone provides suitable postoperative analgesia after cardiac surgery.
Introduction
Nefopam has been used to treat mild-to-moderate postoperative pain since the mid 1970 s. 1 Although its mechanism of action is not completely understood, it is a centrally acting, nonopioid analgesic that inhibits reuptake of serotonin, norepinephrine and dopamine. 2
Open cardiac surgery causes severe pain that can affect a patient’s vital signs and prognosis. Postoperative analgesia is required to achieve patient comfort, stable haemodynamics and postoperative rehabilitation. 3 Analgesia with opioids alone can cause side-effects such as respiratory depression, sedation, urinary retention and nausea. 4 Since opioids have limited analgesic potency, it has been suggested that drug combinations might improve analgesia and limit the occurrence and severity of side-effects. 5 Studies have consistently demonstrated a 30–40% decrease in postoperative opioid consumption when nefopam is used following abdominal or orthopaedic surgery.6,7 Unlike nonsteroidal anti-inflammatory drugs, nefopam has no effect on platelet function, 8 and (in contrast to opioids) does not increase the risk of respiratory depression. 9 In addition, nefopam has been shown to result in decreased morphine consumption when used as a coanalgesic following abdominal surgery. 10
The efficacy and safety of nefopam have not been proven in patients undergoing cardiac surgery. In addition, to the best of our knowledge there are no studies reporting on the use of nefopam as the sole analgesic after cardiac surgery. The aim of this prospective, randomized, double-blind study, therefore, was to investigate the efficacy and side-effects of nefopam both as a sole analgesic and as an adjuvant analgesic in support of fentanyl for patient-controlled analgesia (PCA) after cardiac surgery.
Patients and methods
Study population
The study enrolled patients aged ≥20 years with ASA physical status I–III, 11 scheduled to undergo cardiac surgery in the Department of Anaesthesia and Pain Medicine, Asan Medical Centre, Seoul, Republic of Korea, between May 2011 and January 2012. Exclusion criteria were: emergency surgery; failure to give informed consent; reduced left ventricular function (ejection fraction <40%); history of allergy to study drugs; use of monoamine oxidase inhibitors; active seizure or history of seizure; glaucoma; high risk of urinary retention (i.e., urethral or prostate disease); severe renal or hepatic disease; critical pulmonary disease or history of respiratory disease; tachyarrhythmia or surgery for arrhythmia. Patients were assigned to one of three PCA groups using a randomization plan generator (available at http://www.Randomization.com/): nefopam only; fentanyl only; nefopam + fentanyl.
The Asan Medical Centre Institutional Review Board, Seoul, Republic of Korea approved the study. Ad all patients provided written informed consent prior to enrolment.
Anaesthesia
In all patients, anaesthesia was induced using 0.2 mg/kg etomidate, 0.6 mg/kg rocuronium and 20.0 ng/ml effective site concentration remifentanil via target-controlled infusion (Minto pharmacokinetic model 12 ). Anaesthesia was maintained with propofol and remifentanil using the Orchestra® Base Primea target-controlled infusion system (Fresinius Kabi, Bad Homburg, Germany). During surgery, volume-controlled ventilation was performed and systemic arterial pressure, central venous pressure and cardiac output were monitored.
PCA
Based on the findings of others, 13 the present study used a basal fentanyl PCA infusion rate of 20 µg/h, with a bolus demand dose of 10 µg/15 min and maximal hourly infusion dose of 60 µg. The analgesic effect of 20 mg nefopam has been shown to equal that of 6–12 mg morphine at a continuous basal PCA dose of 2 mg/h. 14 Therefore our study used a basal nefopam PCA infusion dose of 4 mg/h, with a bolus demand dose of 2 mg/15 min and maximal hourly dose of 12 mg.
The PCA was initiated postoperatively in a double-blind manner by an anaesthetist. The total drug volume was 150 ml/patient. Patients in the nefopam group received 300 mg nefopam (2 mg/ml, infused continuously at 4 mg/h) and 0.6 mg ramosetron (to prevent nausea). Patients in the fentanyl group received 1500 µg fentanyl (10 µg/ml, infused continuously at 20 µg/h) with 0.6 mg ramosetron. Patients in the nefopam+fentanyl group received 140 mg nefopam (0.93 mg/ml, infused continuously at 1.86 mg/h) with 700 µg fentanyl (4.7 µg/ml, infused continuously at 9.4 µg/h) and 0.6 mg ramosetron. Drugs were infused at 2 ml/h using an AutoMed3200® (Ace Medical, Seoul, Republic of Korea), with a patient-controlled bolus injection volume of 1 ml. The lock out time was set to 15 min to protect against overdose. The maximal infusion volume was 6 ml per h.
Pain was assessed using a visual analogue scale (VAS) at 12, 24, 36, 48 and 72 h after surgery, both at rest (VASR) and during movement (VASM). Tachycardia, sweating, sedation, respiratory depression, itching, nausea and vomiting were noted during the first 48 h postoperatively. The total PCA volume and number of rescue drug injections were recorded at 12, 24, 36 and 48 h postoperatively. Duration of intubation and length of stay in the intensive care unit (ICU) were noted.
Sample size
Since the aim of the study was to test the noninferiority of nefopam to fentanyl, VAS at 24 h postoperatively was chosen as the primary endpoint. The required number of subjects per group was calculated from the expression:

Statistical analyses
Data were expressed as mean ± SD or n (%). Demographic data were compared using Kruskal–Wallis test for continuous variables and χ2-test for categorical variables. Between-group comparisons of side-effects were performed using χ2-test or Fisher's exact test, and multiple comparisons were performed using χ2-test or Fisher's exact test with Bonferroni correction. Between-group comparisons of extubation time and duration of ICU stay were made using Kruskal–Wallis test. Total PCA volume and number of rescue drug injections at 12, 24, 36 and 48 h were compared using repeated measures analysis of variance followed by post hoc test to assess significance between two groups. A linear mixed model was used to compare simultaneous VAS values, to account for correlations between repeated observations. The noninferiority of nefopam to fentanyl was analysed using 95% confidence intervals (CI) for the difference in VAS (μ2−μ1, as above). Noninferiority was confirmed when the upper 95% CI was less than the noninferiority margin (δ = 1.5). All statistical analyses were performed with SPSS® version 17.0 (SPSS Inc., Chicago, IL, USA) for Windows®. P-values <0.05 were considered statistically significant.
Results
Demographic and clinical characteristics of patients receiving patient-controlled analgesia with nefopam, fentanyl, or nefopam + fentanyl following cardiac surgery.
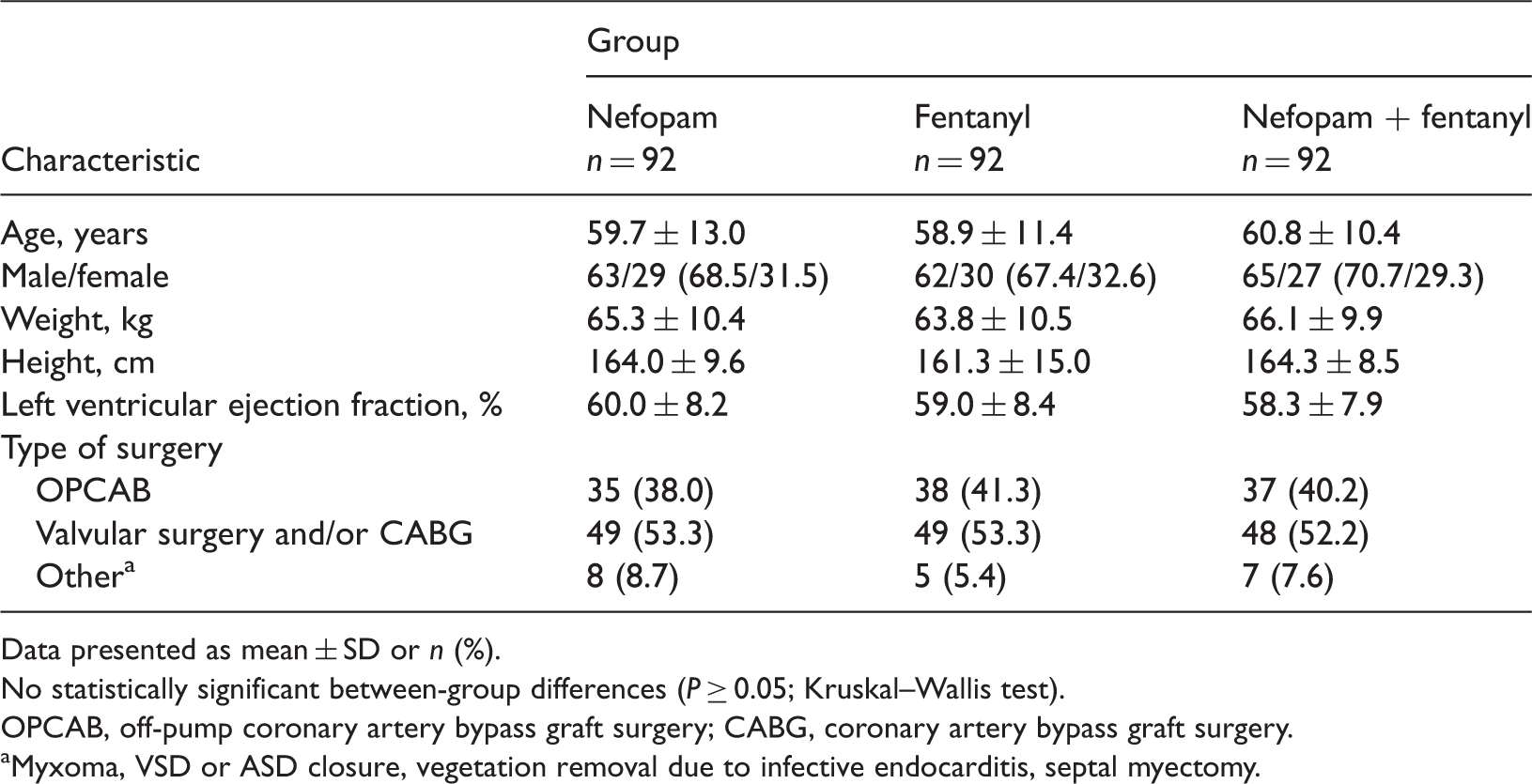
Data presented as mean ± SD or n (%).
No statistically significant between-group differences (P ≥ 0.05; Kruskal–Wallis test).
OPCAB, off-pump coronary artery bypass graft surgery; CABG, coronary artery bypass graft surgery.
Myxoma, VSD or ASD closure, vegetation removal due to infective endocarditis, septal myectomy.
Test for noninferiority between nefopam and fentanyl in patient-controlled analgesia following cardiac surgery.

Data presented as mean ± SD or mean (95% confidence intervals).
VASR 24, resting visual analogue scale pain score at postoperative 24 h; VASM 24, visual analogue scale pain score with movement at postoperative 24 h.
Noninferiority margin defined as 1.5.
Visual analogue scale (VAS) pain scores during 72 h following cardiac surgery in patients receiving patient-controlled analgesia with nefopam, fentanyl, or nefopam + fentanyl.

Data presented as mean ± SD.
VASR, VAS at rest; VASM, VAS with movement.
P = 0.014 vs fentanyl; linear mixed model.
P = 0.024 vs fentanyl; linear mixed model.
Incidence of adverse events during 48 h following cardiac surgery in patients receiving patient-controlled analgesia with nefopam, fentanyl, or nefopam + fentanyl.

Data presented as n (%).
χ2-test or Fisher's exact test.
P < 0.05 vs fentanyl; multiple comparison with Bonferroni correction.
There were no significant between-group differences in the duration of intubation or length of stay in the ICU (data not shown).
Cumulative total infused volume of patient-controlled analgesia (PCA) and number of rescue drug injections during 48 h following cardiac surgery in patients receiving patient-controlled analgesia with nefopam, fentanyl, or nefopam + fentanyl.

Data presented as mean ± SD.
No statistically significant between-group differences (P ≥ 0.05; repeated measures analysis of variance followed by post hoc test).
Discussion
The findings of the present study suggest that nefopam is as effective as fentanyl for postoperative pain relief after cardiac surgery. Acute pain is inevitable after cardiac surgery because of the damage to many pain-sensitive structures due to tissue destruction, intercostal nerve trauma, scar formation, rib fracture, stainless-steel wire sutures and costochondral separation.15−18 The resulting inflammatory response triggers the release of numerous chemical mediators in the periphery, lowering the nociceptor threshold and making these receptors more responsive to painful stimuli.
19
Nefopam is a centrally acting nonopioid analgesic that acts by modulating the effects of these chemical mediators. Its antinociceptive action results from inhibition of serotonin, norepinephrine and dopamine reuptake,2,20 and its antihyperalgesic action is due to reduced glutaminergic transmission via N-methyl-
The incidence of tachycardia and sweating was similar in all three groups in the present study. This is in contrast with others who reported that sweating was more common in patients given nefopam than propacetemol or morphine. 7 All patients in the present study were admitted to the ICU following surgery and some were infused with inotropic agents or vasopressors, according to need. As these sympathomimetic drugs can mask the effects of nefopam, 23 the vital signs, respiratory effort and hepatorenal functions of every patient in the present study were closely observed while they were in the ICU. It was therefore not relevant that the sympathomimetic action of nefopam renders it contraindicated for patients with limited coronary reserves 3 since it was possible to detect any early signs of unstable haemodynamics, such as tachycardia and sweating.
The nonopioid nature of nefopam suggests that it would result in fewer side-effects (such as sedation or respiratory depression) compared with opioids. The frequencies of sedation and respiratory depression were similar in all groups in the present study, however. This may be explained by the cumulative effect of the opioids used during general anaesthesia; in addition, the surgical procedure itself may have contributed to these side-effects. A low incidence of sedation due to nefopam was also reported in other studies.9,24
Nefopam was associated with a lower incidence of nausea than fentanyl, in the present study. It has been reported that 10–30% of patients given a low dose of nefopam experience nausea, usually after its first administration. 25 Nefopam may affect the incidence of nausea by modulating chemical mediators such as serotonin.
The present data indicate that nefopam has a favourable safety profile in relation to many systemic organs of patients who undergo cardiac surgery. It did not cause haemorrhagic complications at the usual dose. 8 Life-threatening effects have been reported in relation to nefopam overdose, however, including rare fatal overdoses characterized by convulsions and arrhythmia.26,27 An accidental overdose was reported in a 77-year-old man who developed acute neurological impairment and renal failure. 28 Overdose was unlikely in the present study, however, since a low dose was used and all patients were closely observed in the ICU after surgery.
The present study has some limitations. A dose of 20 mg nefopam has been shown to be equipotent to 6–12 mg morphine, 24 but the fentanyl equivalent is not known. The study therefore employed the usual analgesic dose of nefopam. Since the focus of the study was on pain control rather than the physical status of the patients, we used the same drug dose for each patient regardless of their weight. ICU care with mechanical ventilation and sedation or inotropic and vasoactive agents could mask the effect of nefopam. In addition, we did not study the long-term effects of nefopam (e.g. duration of hospital stay) or its cost effectiveness. A long term multicentre study is needed.
In conclusion, the present study indicates that nefopam is effective for patients who have undergone cardiac surgery, and PCA with nefopam alone provides suitable postoperative analgesia after cardiac surgery.
Footnotes
Declaration of conflicting interest
This study was funded by Pharmbio, who are the manufacturers of nefopam.
Funding
This study was supported by a grant from Asan Medical Center Hospital in 2011 (2011-0271-0002, Commissioned by Pharmbio Pharmaceutical, Co, Ltd).