
Abstract
Background:
Medication errors represent a significant but often preventable cause of morbidity and mortality in neonates. The objective of this systematic review was to determine the effectiveness of interventions to reduce neonatal medication errors.
Methods:
A systematic review was undertaken of all comparative and noncomparative studies published in any language, identified from searches of PubMed and EMBASE and reference-list checking. Eligible studies were those investigating the impact of any medication safety interventions aimed at reducing medication errors in neonates in the hospital setting.
Results:
A total of 102 studies were identified that met the inclusion criteria, including 86 comparative and 16 noncomparative studies. Medication safety interventions were classified into six themes: technology (n = 38; e.g. electronic prescribing), organizational (n = 16; e.g. guidelines, policies, and procedures), personnel (n = 13; e.g. staff education), pharmacy (n = 9; e.g. clinical pharmacy service), hazard and risk analysis (n = 8; e.g. error detection tools), and multifactorial (n = 18; e.g. any combination of previous interventions). Significant variability was evident across all included studies, with differences in intervention strategies, trial methods, types of medication errors evaluated, and how medication errors were identified and evaluated. Most studies demonstrated an appreciable risk of bias. The vast majority of studies (>90%) demonstrated a reduction in medication errors. A similar median reduction of 50–70% in medication errors was evident across studies included within each of the identified themes, but findings varied considerably from a 16% increase in medication errors to a 100% reduction in medication errors.
Conclusion:
While neonatal medication errors can be reduced through multiple interventions aimed at improving the medication use process, no single intervention appeared clearly superior. Further research is required to evaluate the relative cost-effectiveness of the various medication safety interventions to facilitate decisions regarding uptake and implementation into clinical practice.
Introduction
Medication errors represent a significant burden to the healthcare system. 1 They can be defined as any preventable event that can cause or lead to inappropriate medication use or patient harm and can occur at any stage in the medication-use process such as prescribing, transcribing, dispensing, administering, and monitoring of medications. 2 Neonates are more prone to medication errors at each stage of the medicine management process due to the increased need for calculations, dilutions, and manipulations of medications.3,4 Furthermore, many medications are used off-label in the neonatal setting, meaning that they are not specifically licensed for use in neonates and are therefore often only available in adult formulations and concentrations. 5 As a result, prescribing and administration challenges often places neonates at risk of potentially fatal 10-fold or 100-fold dosing errors.6,7 There is also the associated challenge of limited dosing protocols and evidence-based information regarding the efficacy, safety, dosing, pharmacokinetic, and clinical use of medications in neonates. 6 In addition, relative physiological immaturity means that neonates have less capacity in being able to buffer unintended consequences of medication errors. 8 Such susceptibility towards medication errors in neonates, as previously described, is further emphasized by previous research that observed that medication errors with the potential to cause significant harm were three times more likely to occur in the neonatal intensive care unit (NICU) than in adult wards. 9 Furthermore, an analysis of all medical errors occurring within the NICU identified that medication errors were the single largest contributor, accounting for 47.2% of all errors. 10
Given the complexity of medication use in neonates, the high frequency in which high-risk medications are used and the potential for serious adverse events of even minor medication errors, intervention strategies to increase medication safety in neonatal care should be regularly reviewed. The identification and evaluation of such interventions are of critical importance in assisting healthcare systems and providers in understanding, implementing, and augmenting interventions to reduce neonatal medication errors. 11 Despite this importance, there have been few extensive systematic reviews on interventions for preventing medication errors in the neonatal setting, with the most recent reviews only including literature up until 2013.12 –14 Further, none of these reviews included both comparative and noncomparative studies. The aim of this systematic review was to identify and review different types of interventions to reduce neonatal medication errors.
Method
Search strategy
PubMed and EMBASE were searched for any studies published from 1966 until April 2016, without any language restrictions. The search included a medication errors/safety concept and a neonatal concept, with terms entered as controlled vocabulary and as keywords in all databases. MeSH search terms included: ‘medication errors’ AND ‘Infant, Newborn’, OR ‘Intensive Care Units, Neonatal’, OR ‘Intensive Care, Neonatal’, OR ‘Pediatrics’. Reference lists of all articles included in full-text review, as well as other review articles, were screened for additional studies.
Eligibility criteria
To be eligible for inclusion:
(1) An intervention specifically aimed at reducing the risk of medication errors must be carried out or reported.
(2) There must have been some measure to evaluate effectiveness in reducing risk of medication errors.
(3) The study setting must have included neonates.
Studies only published in abstract form were not eligible for inclusion.
Data abstraction
Two independent, nonblinded authors (MRN and LEG) reviewed each title and abstract for inclusion eligibility. Full-text review was also conducted by two independent, nonblinded authors (MRN and LEG) and discrepancies were resolved through author consensus discussions. For non-English language studies included in the full-text review, the primary author (MRN) translated the contents with computer translation software, which has previously been demonstrated as effective for systematic reviews. 15 The study selection process was documented as per the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA). 16 Data were collected in relation to study characteristics, intervention strategy, comparator treatment (if applicable), type of medication error evaluated, specific detail of medication error, and main study findings. Qualitative descriptors were utilized to describe the results of studies. We did not plan to perform a meta-analysis.
Study quality assessment
Study quality was evaluated by two independent reviewers (MRN and LEG) using the Cochrane Effective Practice and Organization of Care (EPOC) Review Group risk of bias tool, which evaluates all study types together including randomized controlled trials, nonrandomized trials, and controlled before–after studies utilizing the same eight criteria. 17
Results
Search results
Our search identified 1852 abstracts, 226 of which were duplicates and were removed. An additional 14 articles were identified from previous systematic reviews or from checking citations of included studies and were retrieved for full-text review, leaving a total of 1640 unique records. A total of 146 articles were included in full-text review and of these, 101 were deemed eligible for inclusion in the systematic review. One article reported separately on two independently studied interventions, resulting in a total of 102 eligible studies (Figure 1).
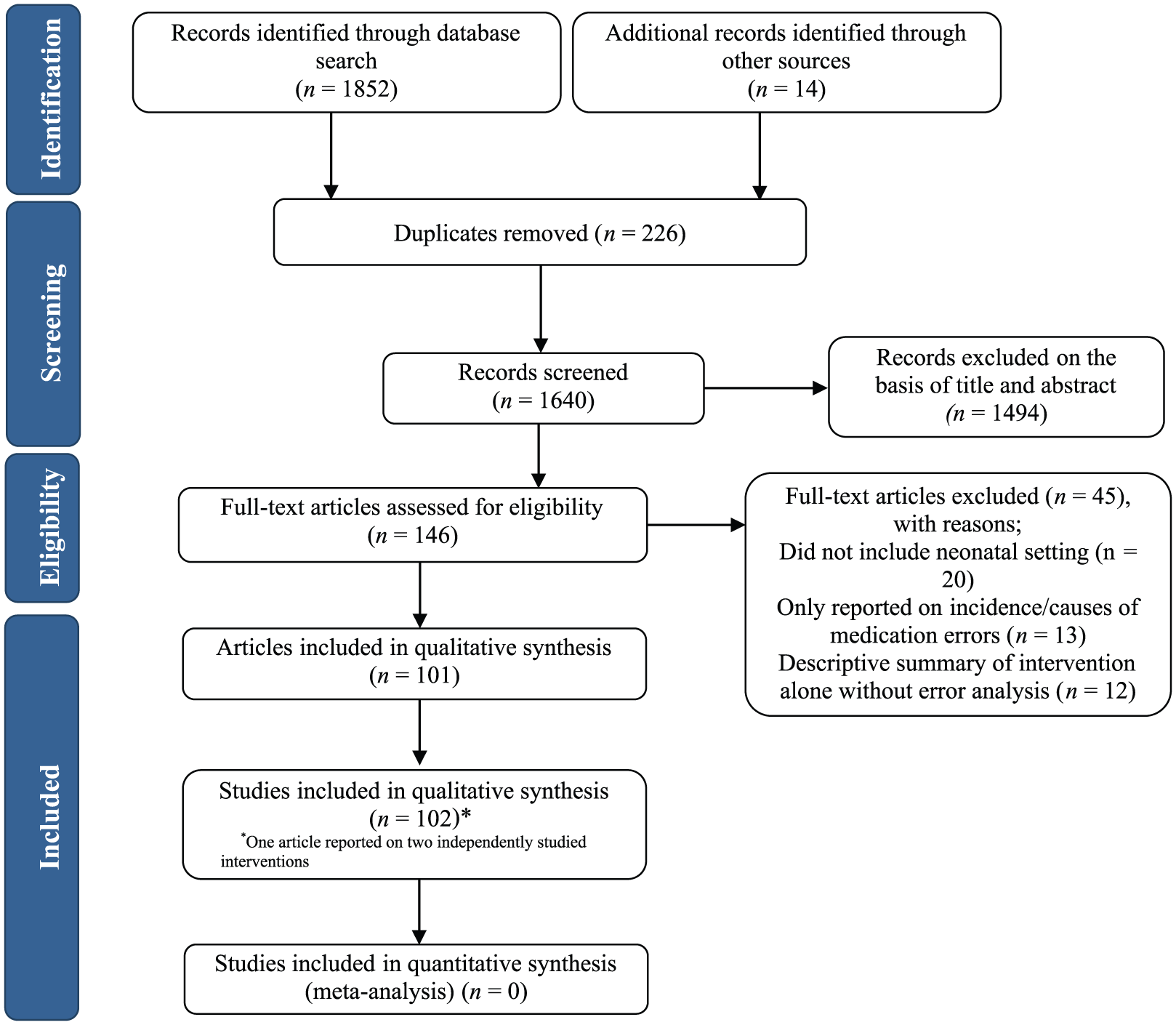
Flow diagram of included studies.
Overview of included studies
Identified studies were grouped according to their intervention type and are presented in Table 1, together with an example of an intervention within that group. The six intervention types included: technology (n = 38),18 –55 organizational (n = 16),56 –71 personnel (n = 13),72 –84 pharmacy (n = 9),85 –93 hazard and risk analysis (n = 8),10,93 –99 and multifactorial (i.e. a combination of any of the previous themes; n = 18).100 –117 A detailed summary of each individual study included in the review is presented in Table 2.
Overview of identified interventions for reducing medication errors in neonatal care.
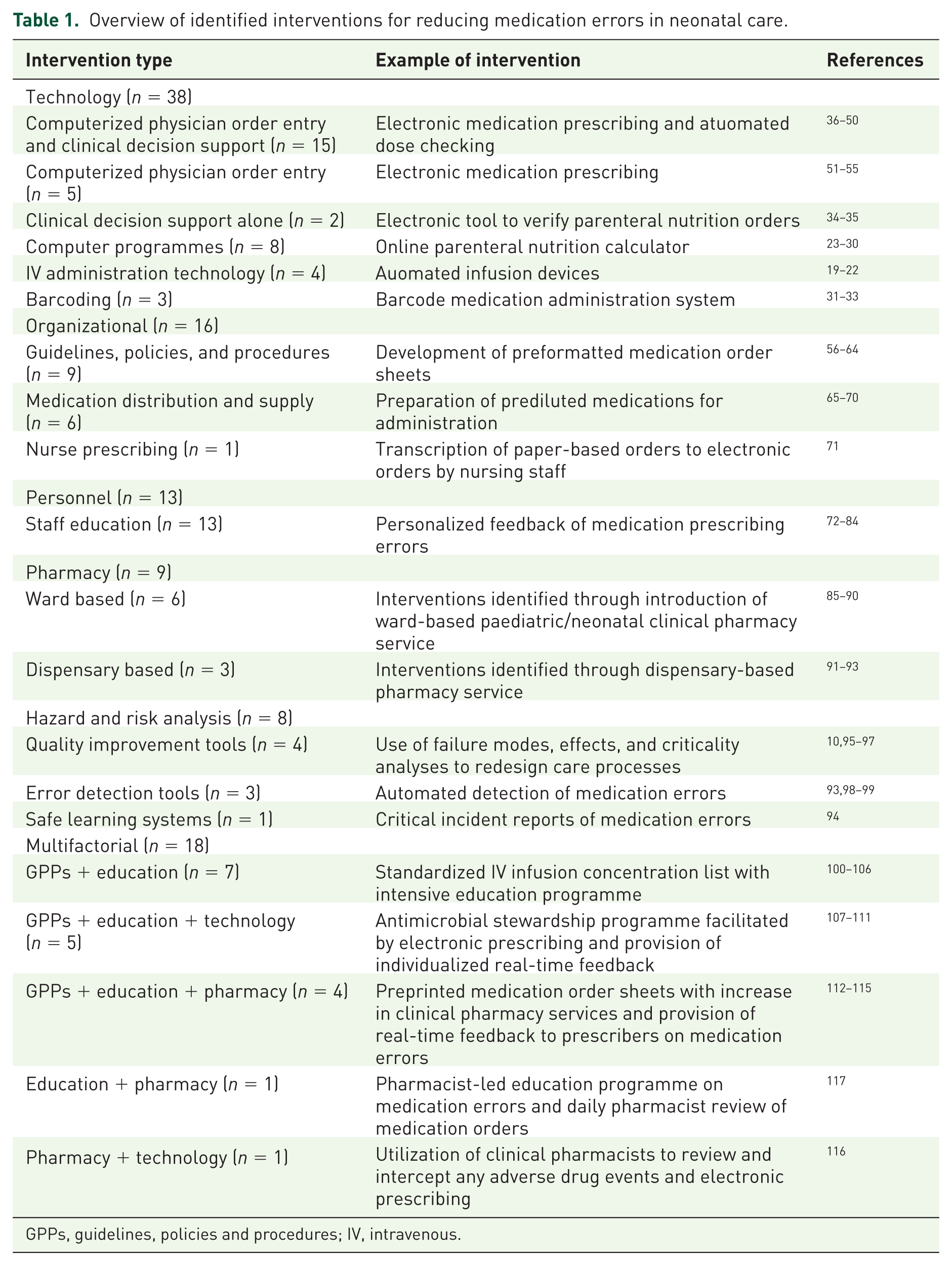
GPPs, guidelines, policies and procedures; IV, intravenous.
Summary of study characteristics and results by primary intervention theme.

ADE, adverse drug event; CDS, clinical decision support; CI, confidence interval; CPOE, computerized physician order entry; GPPs, guidelines, policies, and procedures; HR, hazard ratio; ICU, intensive care unit; IRR, incident rate ratio; IV, intravenous; N, neonatal only; NICU, neonatal intensive care unit; N/P, neonatal and paediatric; OR, odds ratio; PICU, paediatric intensive care unit; PPV, positive predictive value; RR, relative risk; TPN, total parenteral nutrition.
Of the 102 eligible studies, 86 were comparative studies and 16 were noncomparative studies (Table 3). The majority of included studies were undertaken in a combined PICU/NICU setting (n = 64; 63%). Most studies were conducted in the United States (n = 60; 59%), with 42 (41%) studies published since 2010. The majority of studies (n = 68; 66%) focused on a single medication error type, including prescribing (m = 41), administration (n = 26), or monitoring (n = 1), while the remaining 34 (33%) studies involved the investigation of multiple error types.
Aggregate data synthesis for included studies by comparator status.
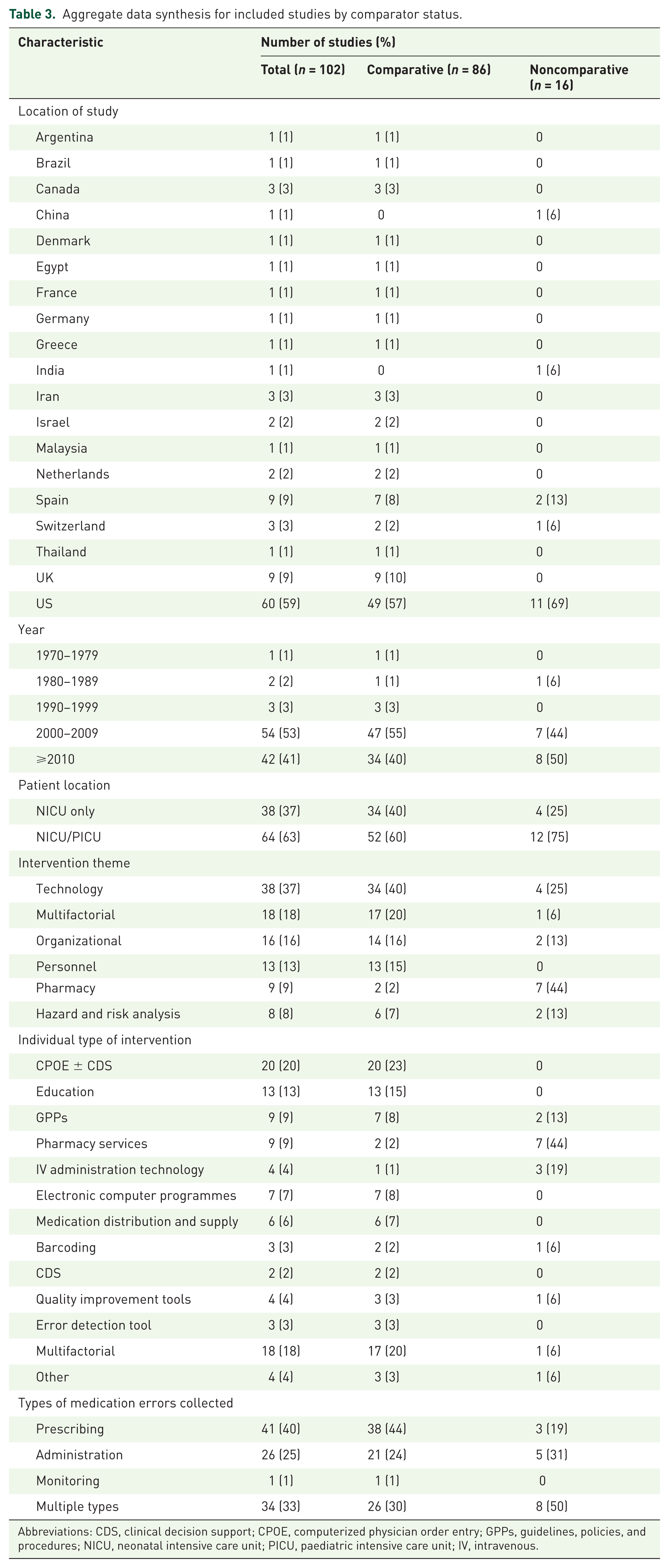
Abbreviations: CDS, clinical decision support; CPOE, computerized physician order entry; GPPs, guidelines, policies, and procedures; NICU, neonatal intensive care unit; PICU, paediatric intensive care unit; IV, intravenous.
Risk of bias evaluation
Most studies demonstrated an appreciable risk of bias (Figure 2). The lack of randomized controlled trials meant that studies were at high risk of bias across the domains related to random allocation of intervention and concealment of intervention group. Inadequate reporting or lack of accounting for differences in characteristics between the pre- and postintervention groups and nonblinding of the assessment of the primary outcome were the main areas of inconsistent bias. A number of studies had unclear risk of bias for incomplete outcome data due to the fact that the outcome was reliant on voluntary incident reports from staff rather than detailed review.
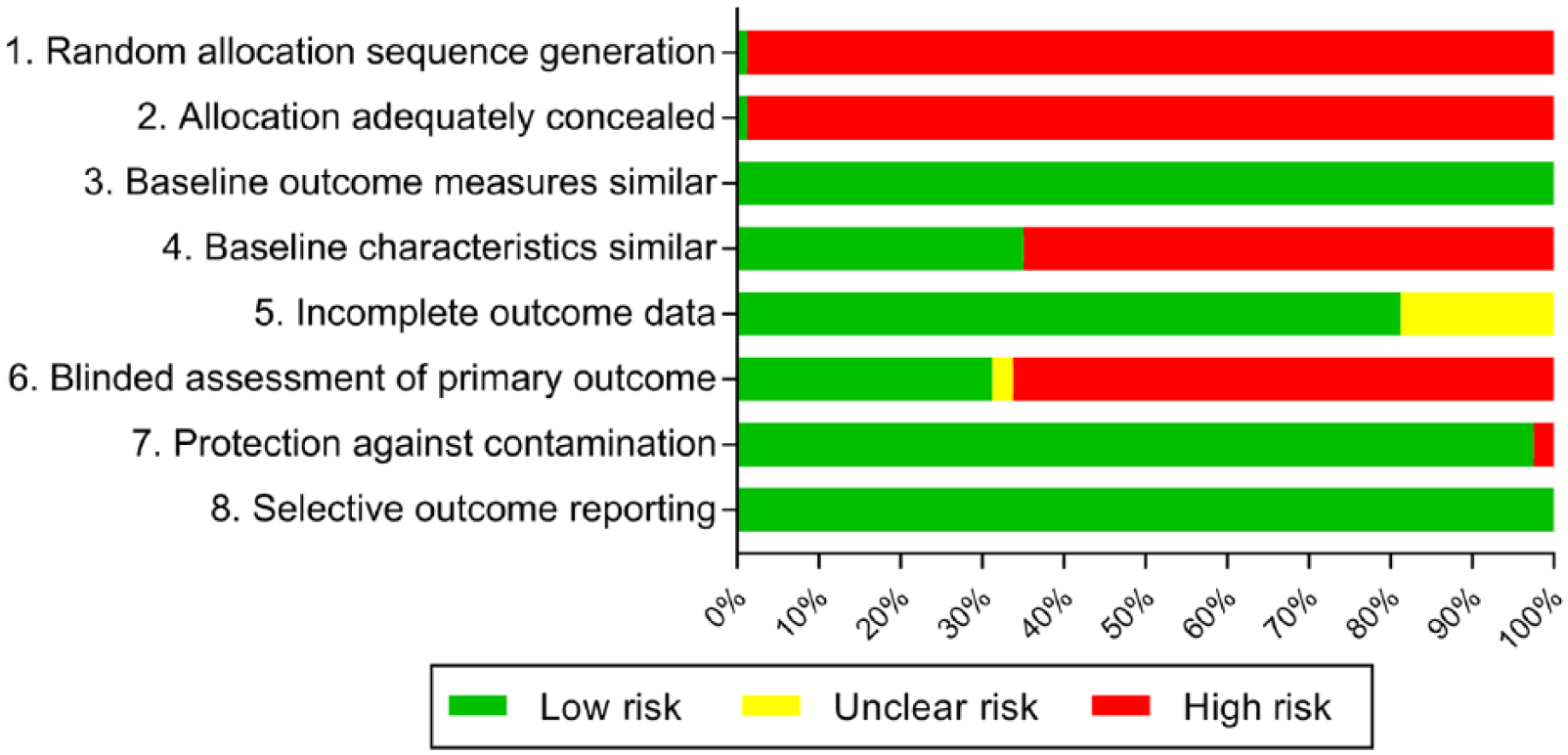
Risk of bias of included studies.
Qualitative synthesis
A breakdown of medication error reduction according to intervention types and medication error types within each intervention theme is presented in Table 4. Based on a qualitative synthesis of comparative studies, the greatest median reduction in overall medication errors was seen with the use of technology-based interventions (73% reduction; n = 33 studies), but this ranged widely from an increase in medication errors of 11% to a decrease in medication errors of 100%. The remaining intervention types produced a similar reduction of medication errors of approximately 50–60%, but again, with a wide range in results.
Qualitative synthesis of reduction in medication errors identified in comparative studies according to intervention theme and type.
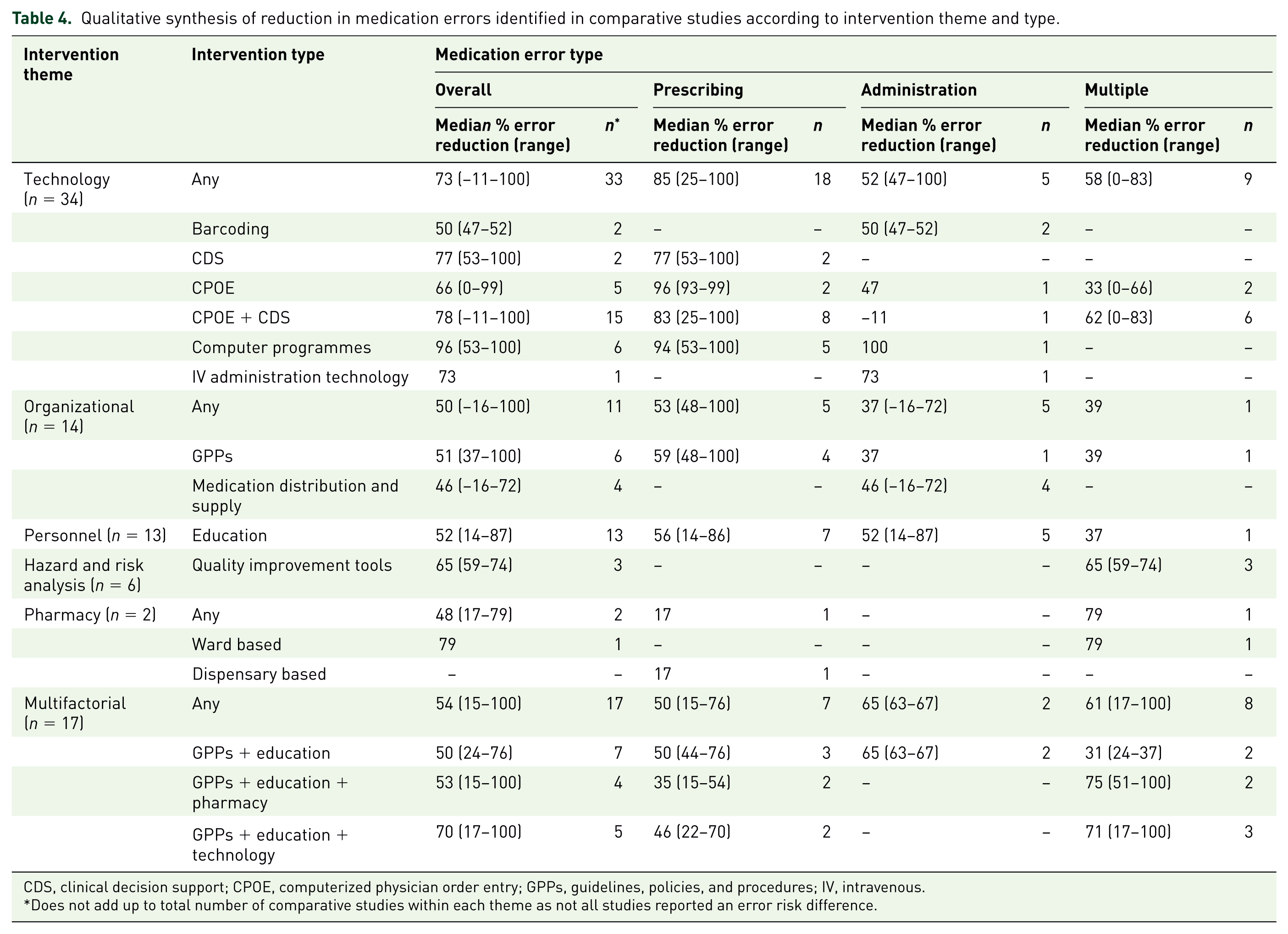
CDS, clinical decision support; CPOE, computerized physician order entry; GPPs, guidelines, policies, and procedures; IV, intravenous.
Does not add up to total number of comparative studies within each theme as not all studies reported an error risk difference.
Eight studies [consisting of a combination of technology- (n = 4), personnel- (n = 2), organizational- (n = 1), and multifactorial-based (n = 1) interventions] reported separately on minor and major medication errors.38,43,45,51,65,78,80,112 Among these studies, the median reduction in medication errors was notably greater for major (76%; 17–100%) compared with minor (26%; −16–66%) medication errors. Notably, one of the studies identified a 16% increase in minor medication errors following the intervention, but a substantial 100% reduction in major errors. 65 The corresponding median reduction in medication errors for any intervention was similar for those undertaken in a neonatal-only (56%; 25–100%) or combined neonatal/paediatric (66%; −16–100%) setting. Similarly, median reduction in medication errors for any intervention was similar regardless of whether errors were identified by incident reports (50%; 17–100%) or detailed medication order review (60%; −16–100%).
Discussion
Based on the findings of our review, no single intervention appeared clearly superior in reducing the risk of medication errors, with significant variability evident among studies within and across themes with respect to methods, definitions, and outcomes. Identified interventions often targeted different aspects of the medication management process, highlighting that a combination of interventions is most likely required to achieve a significant reduction in medication errors.
Santesteban and colleagues have published the most recent systematic review on interventions for preventing medication errors in neonatal care. 14 They restricted their search to studies undertaken in the neonatal unit setting only, identifying a total of 16 intervention studies published up until 2013. Our search was much more extensive, identifying 34 comparative studies undertaken in the neonatal setting, out of our total of 86 comparative studies included in this review. Despite this discrepancy in number of studies, the findings remain similar in that while many interventions demonstrated significant potential for reducing medication errors, no firm conclusions could be drawn as to which interventions were most effective. Our findings are also similar to that of an earlier systematic review by Rinke and colleagues that included 63 studies across both neonatal and paediatric settings, 12 as well as a recent Cochrane review that included findings from just seven studies. 13 Both of these reviews observed that the inability to draw firm conclusions was partly due to limited studies in some areas, while also due to significant methodological heterogeneity evident across studies. Further, a consistent issue raised across reviews is whether decreases in medication errors truly relate to benefits for patients in terms of reducing actual harm.
Despite challenges in linking medication errors directly to patient harm, there is evidence of additional benefits from various interventions beyond a reduction in medication errors. For example, Myers and colleagues observed that the introduction of a computerized physician order entry (CPOE) system with clinical decision support (CDS) was also associated with a reduction in phone calls to pharmacy. 36 Similarly, Vardi and colleagues also demonstrated that this technology was associated with a reduction in the time taken to order resuscitation medications from 14.4 min to 2.1 min (p < 0.001). 44 Notably, Maat and colleagues identified no reduction in medication errors associated with their implementation of CDS to assist in managing hypo/hyperglycaemia, but they did observe reductions in time taken to perform simple (1.3; 0.3–2.3 min) or complex orders (8.6; 5.1–12.1 min). 49
The potential for altered intervention effectiveness due to local variable factors is raised by Abboud and colleagues, who identified no reduction in gentamicin monitoring errors following the introduction of CDS as part of the prescribing process. 41 In this case, the authors suggested that the intervention had minimal benefit because they already had a clinical pharmacist responsible for ensuring monitoring was performed correctly, but results could differ in settings where clinical pharmacists are not present.
A common observation across studies that utilized a staged design to implement CPOE and then CDS was that maximal benefits were not gained until CDS was added.46,48 Intuitively, this makes sense as CDS or computer programmes are usually developed to address activities that have already been predetermined to be high risk, and so have greater potential for reduction in medication errors. Notably, such improvements were not necessarily restricted to technology-based interventions. Less costly interventions involving paper-based prescribing and CDS, such as use of preprinted order forms, were identified as achieving similar reductions in medication errors to more expensive, computer-based approaches.59,64 Therefore, in settings where CPOE systems are not readily available, lower-cost alternative approaches towards CDS are ideal.
An issue common across a number of studies was the need to adequately support staff in the implementation of any interventions, especially those that significantly change current practices. For example, with the introduction of automated infusion devices in drug libraries, there is a reliance on staff using the technology to its full extent in order to obtain maximal benefit. For various reasons, whether it be staff who consider the new process more complicated or too time consuming, work arounds may be created which can lead to medication errors. In introducing automated infusion devices, Manrique and colleagues monitored their use and identified an overall compliance rate of 78–85%.21,22 While the automated infusion devices appeared extremely effective in preventing potentially catastrophic medication errors, compliance was still not ideal. Hennings and colleagues identified that neonatal ICU staff were almost twice as likely (RR 1.68; 1.18–2.38) to reprogramme pumps than adult ICU staff. 20 Whether this was just due to staff ignoring or overriding the alerts or because the medication library and associated functions were not sufficiently programmed for use in the neonatal unit is unclear. However, these examples highlight the importance around thorough implementation strategies and the requirement to constantly monitor and evaluate the use of new technologies as they are implemented within the neonatal unit. There is also the constant requisite to review and update such technologies as time goes on, as further advancements are made.
Strengths of our review include the comprehensive literature search strategy and inclusion of a broad range of comparative and noncomparative studies to explore the breadth of research previously undertaken on interventions for reducing medication errors in neonates. This is of particular usefulness in exploring the evaluation of different interventions to support implementation into clinical practice, as well as guide future research priorities.
Notwithstanding the comprehensive nature of our systematic review, several limitations bear consideration. First, significant variability was evident across all included studies, with differences in intervention strategies, trial methods, types of medication errors evaluated, and how medication errors were identified and evaluated. Such heterogeneity has been observed in previous systematic reviews of interventions to reduce paediatric medication errors. 12 A key aspect for overcoming limitations in the existing evidence base identified in this review lies in standardization of definitions and research methodologies for medication error studies. In particular, consistent grading of medication errors using universal reporting standards, such as the one endorsed by the National Coordinating Council for Medication Error Reporting and Prevention, would facilitate a greater understanding of the impact of interventions on harmful medication errors. 118 This is of importance as only eight of the identified studies reported separately on minor and major medication errors, demonstrating a significant difference in error reduction depending on the definition utilized. Notably, one of the studies identified a 16% increase in minor medication errors following the introduction of the intervention, largely thought due to increased awareness and reporting of errors, but a substantial 100% reduction in major errors. 65 Others have also called for more consistent use of denominators that better reflect the total opportunities for error (e.g. prescribing errors per 1000 medication orders), rather than the use of other denominators such as medication errors per patient or per patient day; 12 the latter being considered more susceptible to bias from factors such as the criticality of the patient and number of medications being ordered, and limiting ability to accurately compare results across studies.
Conclusion
While neonatal medication errors can be reduced through multiple interventions aimed at improving the medication use process, no single intervention appeared superior. Despite the significant increase in the number of published studies focused on reducing neonatal medication errors, our knowledge of interventions to prevent neonatal medication errors remains hampered through a lack of uniformity in study design, data collection methodology, and outcome reporting. This heterogeneity leads to difficulties in developing clear guidance as to which interventions are best to adopt. Further research is required to evaluate the relative cost-effectiveness of the various medication safety interventions to facilitate decisions regarding uptake and implementation into clinical practice. Ultimately, the choice of the ideal interventions for improving medication safety will likely be an individual one, taking into consideration local resources, together with an understanding of the types and severity of errors that occur within the organization.
Footnotes
Acknowledgements
Luke E Grzeskowiak acknowledges salary support provided through an Australian National Health and Medical Research Council (NHMRC) Early Career Fellowship (ID 1070421).
Authors’ Note
Luke E Grzeskowiak is also affiliated to SA Pharmacy, Flinders Medical Centre, Bedford Park, SA, Australia.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The authors declare that there is no conflict of interest.