
Abstract
Background and purpose:
Diabetes in adolescents is usually associated with cardiovascular Autonomic Nervous System (ANS) disorders. The aim of this study was to investigate the effect of exercise and Mindful Self-Compassion Therapy (MSCT) on heart rate variability (HRV), aerobic capacity (VO2peak), and glycemic index of adolescent boys with type 1 diabetes (T1D).
Methods:
A total of 60 adolescent boys (Age: 12–18 years, Body Mass Index: 19.75 ± 2.26 kg/m2) were enrolled in this semi-experimental research. The participants were allocated into four groups: Control Diabetes (CD, n = 15), Exercise Diabetes (ED, n = 15), MSCT Diabetes (MD, n = 15), and Exercise + MSC Diabetes (EMD, n = 15). The ED group received 3 sessions per week of combined resistance and interval (running) and training, the MD group received 8 sessions of 60 min of MSCT, and the EMD group received exercise training + MSCT during a 12-week intervention period. A two-way multivariate analysis of covariance (MANCOVA) was used with pre-test values as covariate variables to evaluate changes in a range of HRV variables following the interventions.
Results:
The ED and EMD groups showed increases in High Frequency (HF), Root Mean Square of Successive RR Interval Differences (RMSSD), Standard Deviation of NN Intervals (SDNN), Very-Low-Frequency (VLF), Low-Frequency (LF), and VO2peak. There was a decrease in resting Heart Rate (HR), LF/HF, and HbA1c levels. The MD group had a substantial increase in HF and RMSSD and a significant decrease in HR and LF/HF (p < 0.05).
Conclusion:
The results support the application of combined interval/resistance exercise training and stress control method (MSCT) as an effective non-invasive intervention for enhancing the psychophysiological parameters of HRV in adolescent boys with T1D compared to exercise or MSCT alone.
Plain language summary
Type 1 Diabetes is commonly associated with damage to the nerves that control the heart and blood vessels which could lead to an increased risk of heart complications. While exercise training and self-compassion have shown positive results in managing type 2 diabetes, further research is needed to explore the benefits of combined interventions in people affected by Type 1 diabetes. The study investigated the combined effect of exercise (running and strength training) and Mindful Self-Compassion Therapy on variations in time between consecutive heartbeats, heart and respiratory health, and blood sugar control in 60 young males aged between 12 and 18 years with diabetes type 1. The results showed that application of concurrent exercise (combined aerobic/resistance training) and mindful self-compassion therapy may provide an effective safe intervention for improving the heart beat variations and mindfulness in young males with type 1 diabetes compared to exercise or mindful self-compassion therapy alone.
Keywords
Introduction
Nowadays, type 1 diabetes (T1D) is reported as one of the most common chronic health conditions in the world, affecting young people. 1 According to the World Health Organization (WHO), there is an increasing trend in the prevalence and occurrence of T1D. 2 In people with T1D, abnormal fluctuations in blood sugar level cause microvascular and macrovascular complications, leading to at least a 10-fold increase in cardiovascular complications and reduced quality of life compared to healthy individuals of the same age. 3
In general, the activity of the autonomic nervous system (ANS) in T1D is associated with an increase in sympathetic nervous system (SNS) participation and a decrease in parasympathetic activity because of reduced functional capacity. 4 Ultimately, the culmination of these physiological disturbances leads to the manifestation of disease-related cardiovascular or metabolic complications. These complications progress in childhood and adolescence without obvious clinical symptoms. 5 Cardiac Autonomic Neuropathy is a consequence of T1D underpinned by disturbances in the cardiovascular ANS. 3 This is one of the most neglected long-term complications of T1D that remains subclinical until the final stages of the disease. 6 Hence, early identification of risk factors is critical for the timely prevention and management of cardiovascular disease (CVD)
An early subclinical marker that can occur in the early stages of T1D with chronic complications is an imbalanced HRV. 7 The physiological phenomenon of HRV shows fluctuations between successive heartbeat intervals, enabling the heart to control stress situations according to the ANS. 8 Rapid non-invasive acquisition of HRV enables early detection of heart failure in children and adolescents, providing a surrogate for the implementation of appropriate interventions to control and improve cardiovascular health. 9 T1D-related age group has the most blood sugar deviations due to hormonal changes and imbalanced nutritional habits, making efficient insulin management and blood sugar control significantly important in reducing the progression and prevalence of complications. 10 Furthermore, HRV is affected not only by physical conditions but also by emotional stress (fear of long-term complications, hypoglycemia, feelings of helplessness, and exhaustion) and can therefore be considered an important psychophysiological parameter. 11
While insulin use is the most common intervention for optimal control of type 1 diabetes, concurrent aerobic and resistance exercise training plays an important role in diabetes management by improving HRV, glycemic control, body composition, lipid profile, CRF, blood pressure, body weight, increasing insulin sensitivity, and improving quality of life through blood sugar control.12 –14
Despite the implementation of common control programs (insulin administration, exercise training, and balanced nutrition), blood sugar may remain uncontrolled due to the emergence of psychological disorders such as stress and anxiety. 15 Recently, the psychological aspects of T1D have received increasing attention from experts due to behavioral and emotional components strongly associated with the self-managing nature of T1D, supporting that more efficient control of T1D could occur when psychological components are incorporated into the management plan. 16 Mindful Self-compassion Therapy (MSCT) is one of the psychological interventions for enhanced control of T1D. There is some evidence that MSCT reduces the amount of stress associated with diabetes self-care, with subsequent effects on metabolic responses such as low blood sugar levels. Previous studies have shown the positive impact of MSCT on reducing blood hemoglobin and improving HRV.17,18 Hence, compassion may act alongside exercise adaptations (metabolic, autonomic, and functional) as a tool for coping with stress in people with diabetes.17,19
Considering the limited research on adolescents with T1D, it is important to identify potential non-pharmacological interventions for reducing disease-related complications. The implementation of an exercise program (i.e., to stimulate and use muscle volume for improved metabolic health) combined with MSCT (i.e., to stimulate the parasympathetic aspects of the ANS for controlling unnecessary emotions and stress) could affect HRV as an indicator of cardiovascular health in T1D. The present study aimed to investigate the effect of interval/resistance training and MSCT on resting HRV values, aerobic capacity, and sugar factors in adolescent boys with T1D.
Methods
This research project was approved by the Ethics Committee of the Cardiovascular Medical Education and Research Center (ID. IRCT202111031052926N1), and all participants gave written informed consent prior to participation in the study.
Participants
The participants, including 60 boys with T1D (14.93 ± 1.64 years), were allocated into four groups: Exercise Diabetes (ED, n = 15), MSCT Diabetes (MD, n = 15), Exercise + MSCT Diabetes (EMD, n = 15), and Control Diabetes (CD, n = 15) (Figure 1). The mean and standard deviation in LF/HF in a similar population were 2.03 and 1.56, respectively 7 ; from this, we calculated that to maintain a power of 80% at a significance level of 0.05, we required 15 participants per group. Inclusion criteria were age of 12–18 years old, inactive (steps/day < 5000), minimum disease duration of 5 years, mean glycemia (FBS > 130 mg/dl) in the previous 3 months, and HbA1c > 7.5. Daily calorie intake was 2458 ± 394 for T1D participants. T1D participants were recruited through regional schools and were reviewed by an endocrinologist before being enrolled into study. A flow diagram of participation according to CONSORT is shown in Figure 1.
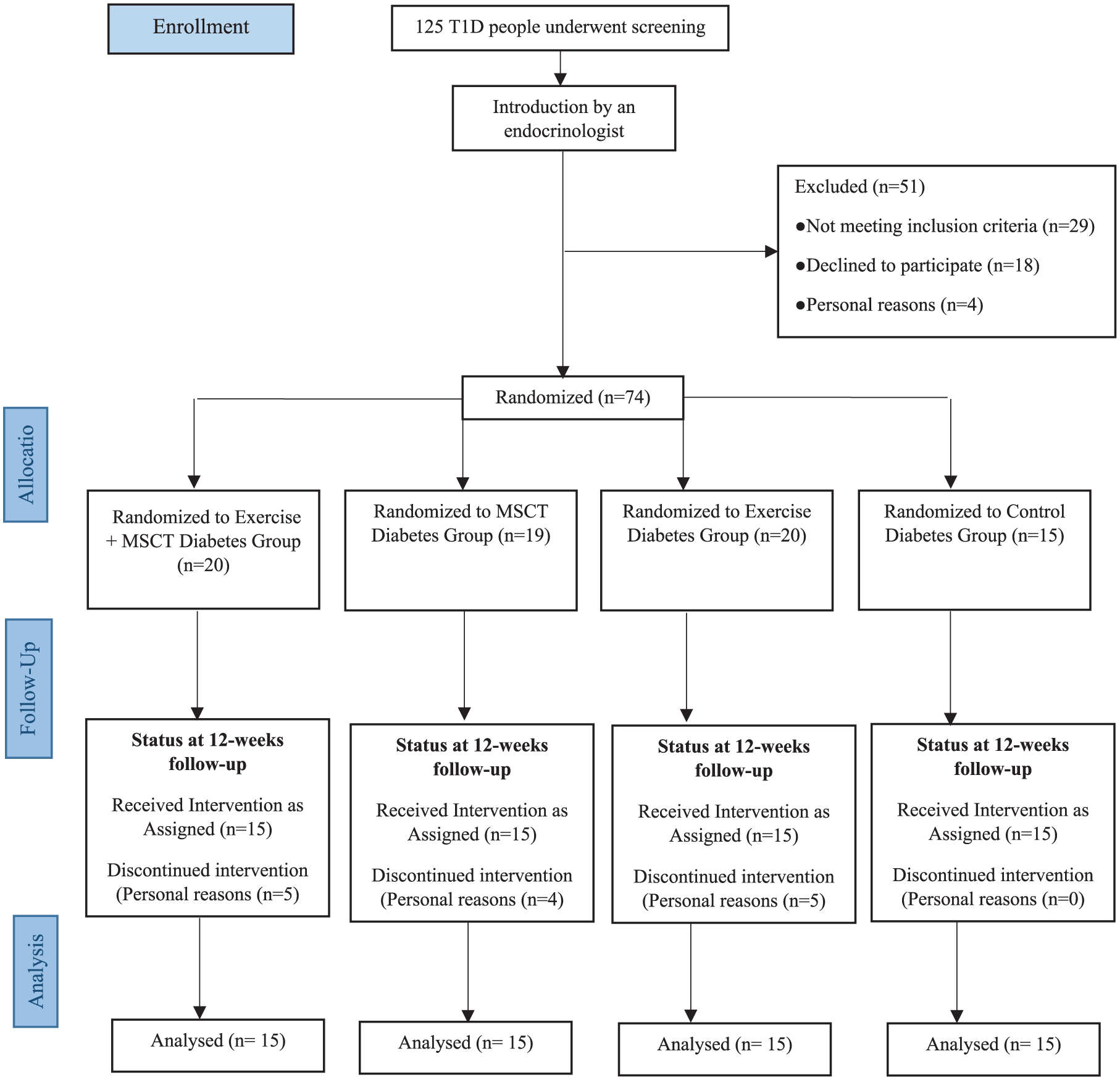
Study flow chart according to CONSORT guidelines.
All participants completed a health screening questionnaire to record state of anxiety (STAI), history of diabetes diagnosis, average minutes of physical activity per day, medication use, and comorbidities (Table 1). Exclusion criteria were diabetic neuropathy (autonomic and peripheral), nephropathy, cardiovascular diseases (history of palpitations, chest pain, and heart failure during exercise), cerebrovascular and respiratory diseases, medications affecting HR, and chronic psychological disorders.
General characteristics of subjects (mean ± SD).

CD, Control Diabetes Group; DD, Diabetic Duration; ED, Exercise Diabetes Group; EMD, Exercise + Mindful self-compassion Diabetes Group; FBS, Fasting Blood Sugar; HbA1c, Hemoglobin A1c; MD, Mindful self-compassion training diabetes Group; SD, Standard Deviation; STAI, State-Trait Anxiety Inventory.
Experimental design
All the tests were performed in an educational medical center from 9:00 am to 11:00 am and 2 h after eating a light breakfast. Participants with T1D had their insulin dose as prescribed by their doctor and were asked to refrain from consuming caffeinated products, alcohol, and participating in vigorous exercise 48 h before the test. To prevent hypoglycemia or hyperglycemia, glucose levels were taken before, at the peak, and after exercise session. Exercise training was terminated if blood glucose reached to less than 5.56 mmol/l or more than 13.9 mmol/l. 20
HRV parameters
Heart rate (HR) and HRV were recorded using a 5-lead Holter monitoring device (18630, Medset GmbH, Hamburg, Germany) according to the gold standard method recommended by the Task Force of the European Society of Cardiology for the 24-h recording. 21 HRV recording was performed by a cardiologist for each participant from 9 am continuously for 24 h (before and after training) with a sampling frequency of 1000 Hz of the ECG signal, with an accuracy of 1 ms for each interval. Ectopic beats and signal artifacts were eliminated using standard procedures. RR intervals considered non-physiological, specifically those longer than 1.5 s or shorter than 0.33 s were excluded. In addition, RR intervals differing by more than 20% from the preceding RR interval or from the overall mean RR interval were removed. Missing segments in the time series were filled using linear spline interpolation. The resulting RR interval series was then resampled at 3.413 Hz (1024 samples per 5-min segment) to obtain an evenly spaced time series suitable for spectral analysis of HRV. During the 24-h monitoring period, participants maintained their usual insulin dosage and routine daily activities (fewer than 5000 steps per day) and were prohibited from strenuous activity. All participants were fitted with a Beurer (Speedbox) pedometer (Beurer, Ulm, Germany) to monitor their motion activity. The following parameters were extracted and calculated in relation to R-R interval changes in the time domain: mean number of adjacent NN intervals (mRR), standard deviation of R-R intervals (SDNN), standard deviation of the 5-min R-R interval mean (SDANN), root mean square difference of consecutive R-R intervals (RMSSD), and percentage of beats with consecutive R-R interval difference > 50 ms (pNN50). Parameters measured in the frequency domain included high frequency (HF), low frequency (LF), very low frequency (VLF) and the ratio of LF to HF (LH/FH).
Maximum exercise capacity (VO2peak)
VO2peak evaluation with maximum Graded Exercise Testing (GXT) was performed according to the modified Bruce protocol with a treadmill (XSCRIBE, Italia TM65, Mortara) at a temperature of 19°C–21°C, relative humidity of 39%–41% and height of 1860 m above sea level. HR was monitored during the GXT by Holter monitoring. Participants were asked to refrain from strenuous physical activity 24 h before GXT. VO2peak was calculated as the greatest average of respiratory VO2 during 20 consecutive seconds. A successful exercise test allowing the determination of VO2peak was defined by at least two of the following criteria: R value ⩾1.1; Maximum HR ⩾85% of maximum predicted (i.e., 208 − (0.7 × age in years)), and a plateau in O2 consumption (<150 mL/min) despite increase in the workload.
Exercise training
The training program consisted of 3 days/week of supervised interval (running) and resistance training (IRT) for 12 weeks. All participants were prohibited from heavy physical activity 24 h before the tests. IRT was performed in the morning with knowledge of the safe range of blood glucose levels (140–250 mg/dL). Each training session began with 10 min of warm-up and stretching, followed by resistance training performed before running to minimize exercise-induced hypoglycemia. Training loads were determined using an indirect 1RM estimation (Holten method), targeting 6–12 repetitions. Each session included bodyweight exercises (lunges and push-ups) and resistance exercises (leg presses, chest presses, leg extensions, seated shoulder presses, biceps curls, and triceps dips), performed in three sets of 8–12 repetitions with 1.5–2 min of rest, lasting 10–15 min. The session then involved 25–50 min of interval running training, and ended with 5 min of cooling down. 22 Figure 2 provides an overview of the exercise intervention program.

Schematic presentation of combined exercise and MSCT training.
Interval training sessions consisted of three to six 5-min running bouts (three bouts in week 1, progressively increased to six bouts by the final week) performed at an intensity of 50%–75% of heart rate reserve (HRR), with 4 min of active recovery at 10%–20% HRR following each bout. HR was continuously monitored during training using a heart rate monitor (Polar H10, Finland) to ensure adherence to the prescribed intensity. Training intensity was adjusted throughout each session to remain within the target heart rate range. Training volume was gradually increased every 3 weeks to prevent physiological adaptation. 23
Laboratory analyses
Thoroughly heated blood samples were centrifuged at 1500°C for 15 min at 4°C, plasma was then collected, frozen, and stored in a −80°C freezer for subsequent batch analysis. Fasting blood sugar (FBS – mg/dl) and hemoglobin A1c percentage (HbA1c%) were determined by the enzymatic method using quality-controlled commercial kits (LDN, Germany).
Psychological intervention
The structure of the psychological protocol was adapted from Germer and Neff’s method 24 (Figure 2). The protocol began with getting to know the MSCT program. It continued with introducing and practicing the theoretical and practical components of mindfulness and training to focus on the present. In the following stage, the subjects tried to discover the core of values that give meaning to life by practicing kindness and cultivating love, practicing self-compassion, and distinguishing self-compassion from the inner critic. In the next step, participants practiced dealing with difficult emotions: regulating emotions, learning to label emotions and a compassionate friend, recognizing and examining two kinds of suffering in relationships, facing unmet needs, and self-compassion. It was then ended with compassion for self and others, mindfulness of positive experiences, and gratitude.
Data analysis and statistics
Mean and standard deviation were used for descriptive statistics. The results of the Shapiro–Wilk test showed that the data distribution was normal (p > 0.05); Homogeneity of variances was confirmed using Levene’s test (p > 0.05). The assumption of equal slopes, equality of covariance matrices, and equal residual variances was met (p > 0.05). Two-way multivariate analysis of covariance (MANCOVA) was used with pre-test values as covariate variables for inferential statistics and examining the effect of interventions (exercise and compassion) between the groups. The Bonferroni corrections for multiple comparisons were applied (Tables 3 and 4). Time-domain variables (ASDNN5, SDNN, RMSSD, and PNN50) and frequency-domain variables (VLF, LF, HF, and LF/HF) were incorporated into two different group analyses. The interaction effects were examined (Tables 3 and 4). The relationship between VO2Peak and LF/HF variables was analyzed using inverse and Bland-Altman plots. All analyses were performed at a significance level of less than 0.05 using SPSS version 26 software. GraphPad Prism version 8.0.2 software (GraphPad Software, San Diego, CA, USA) was used to draw the graphs.
Results
Participants attended approximately 90% of all scheduled training sessions. Throughout the intervention period, no serious adverse events were observed. Absences were attributable solely to non-study-related factors such as routine illness or personal travel; no participant missed a session due to pain, injury, or any condition arising from the training protocol itself. Mild delayed-onset muscle soreness was reported by four participants, predominantly during the initial weeks of training, and these symptoms resolved without treatment. Three participants experienced transient hand discomfort associated with the use of weight-lifting equipment, and in one case, the issue was successfully mitigated by the adoption of protective gloves. Across the duration of the program, participants in the experimental condition demonstrated progressive overload and ultimately increased the resistance used in all prescribed exercises to at least 95% of their baseline training loads.
The results of descriptive and inferential statistics are presented in Tables 2–4, respectively. Tables 3 and 4 present the results of the “ANCOVA,” and in this table, the effects of the research factors alone and in interaction with each other are examined, including the effect of exercise alone (ED), compassion alone (MD), and the interactive effect of exercise and compassion with each other (EMD). Results indicated a significant effect of exercise training on SDNN and RMSSD and a significant effect of compassion on RMSSD and PNN50 (Table 3). Exercise also had a significant effect on all variables, including VLF, LF, HF, and LF/HF, while compassion had a significant effect only on HF and LF/HF (Table 4). Inverse and Bland-Altman graphs supported these findings (Figure 3).
Results of descriptive statistics of participant demographics and variables.
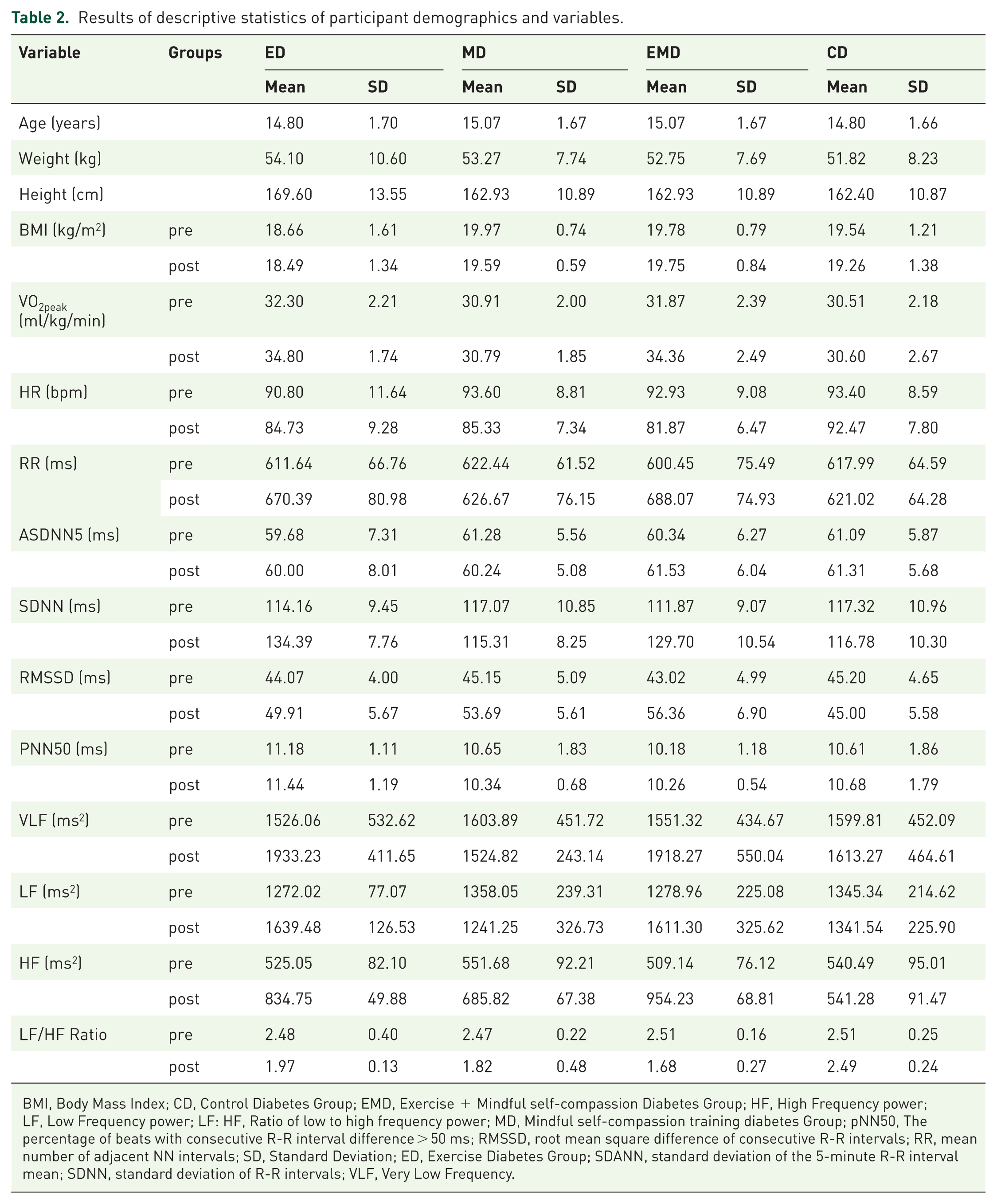
BMI, Body Mass Index; CD, Control Diabetes Group; EMD, Exercise + Mindful self-compassion Diabetes Group; HF, High Frequency power; LF, Low Frequency power; LF: HF, Ratio of low to high frequency power; MD, Mindful self-compassion training diabetes Group; pNN50, The percentage of beats with consecutive R-R interval difference > 50 ms; RMSSD, root mean square difference of consecutive R-R intervals; RR, mean number of adjacent NN intervals; SD, Standard Deviation; ED, Exercise Diabetes Group; SDANN, standard deviation of the 5-minute R-R interval mean; SDNN, standard deviation of R-R intervals; VLF, Very Low Frequency.
Results of multivariate analysis of covariance (MANCOVA) for time-domain variables.

Computed using alpha = .05; bR Squared = 0.721 (Adjusted R Squared = 0.684); cR Squared = 0.744 (Adjusted R Squared = 0.709); dR Squared = 0.546 (Adjusted R Squared = 0.484); eR Squared = 0.583 (Adjusted R Squared = 0.527); Significance level was set at p < 0.05.
ED, Exercise Diabetes Group; EMD, Exercise + Mindful self-compassion Diabetes Group; HF, High Frequency power; LF, Low Frequency power; LF: HF, Ratio of low to high frequency power; MD, Mindful self-compassion training diabetes Group; pNN50, The percentage of beats with consecutive R-R interval difference > 50 ms; RMSSD, root mean square difference of consecutive R-R intervals; SDANN, standard deviation of the 5-minute R-R interval mean; SDNN, standard deviation of R-R intervals; VLF, Very Low Frequency; η, Etta Square (Effect Size).
Results of multivariate analysis of covariance for Frequency-domain variables.

Computed using alpha = .05.bR Squared = .813 (Adjusted R Squared = .788); cR Squared = .707 (Adjusted R Squared = .667); dR Squared = .911 (Adjusted R Squared = .899); eR Squared = .648 (Adjusted R Squared = .601); Significance level was set at p < 0.05.
ED: Exercise Diabetes Group; EMD: Exercise + Mindful self-compassion Diabetes Group; HF: High Frequency power; LF: HF: Ratio of low to high frequency power; LF: Low Frequency power; MD: Mindful self-compassion training diabetes Group; pNN50: The percentage of beats with consecutive R-R interval difference > > 50 ms; RMSSD: root mean square difference of consecutive R-R intervals; SDANN: standard deviation of the 5-minute R-R interval mean; SDNN: standard deviation of R-R intervals; VLF: Very Low Frequency; η: Etta Square (Effect Size).

Inverse and Bland-Altman graph representing the relationship between VO2Peak and LF/HF Ratio data.
Discussion
The study aimed to compare the effect of exercise and MSCT interventions on HRV variables in boys with T1D. The main findings suggest an improved HRV following the exercise training in terms of improved HRV indices associated with autonomic modulation. The MSCT showed an increase in parasympathetic nervous system (PNS) parameters and combined exercise, and MSCT training led to improvement in HRV indices associated with autonomic modulation. Furthermore, exercise intervention led to an increase in the HF, LF, RMSSD, and SDNN and a decrease in LF/HF. Post exercise VO2peak changes were related to the improvement of LF/HF.
Previous studies of male T1D patients have reported increases in the activity of HRV indices associated with autonomic modulation (LF, HF, RMSSD, SDNN) and decreases in LF/HF in exercised groups compared to sedentary counterparts, which are consistent with the results of the present research.25 –28 In a study on children with T1D, Chen et al. reported an increase in LF and HF in the exercise intervention group compared to the no-intervention group. 29 Other studies comparing trained T1D adolescents with the control group reported improvements only in PNS parameters of HRV (HF and RMSSD).30,31 A systematic meta-analysis by Hamasaki reported that exercise training, endurance training in particular, leads to increased PNS and decreased LF/HF activity. 32 Meta-analysis by Chiang et al. reported an increased PNS activity in people with diabetes after 2 to 3 months of regular exercise (3 times/week) and a decrease in SNS activity following > 4 months of exercise training. 33
Regular exercise has been shown to be effective in reducing serum levels of norepinephrine (the most important predictor of cardiac mortality) and N-terminal pro-brain natriuretic peptide. Conversely, exercise increases nitric oxide levels in the paraventricular nucleus (an important factor in cardiac vagal modulation) and reduces the level of angiotensin II. These changes lead to the inhibition of SNS activity and an increase in the PNS activity in diabetic patients.34 –36 Furthermore, exercise could lead to a decrease in serum TNF by increasing blood volume and activating baroreflexes, which are modulated by the activity of the subdiaphragmatic vagus nerve. 37
In the present research exercise intervention led to decreases in HbA1c, HR at rest, and increases in VO2peak. This is in agreement with previous studies supporting the effect of regular exercise in controlling the blood glucose in T1D, potentially due to exercise-induced metabolic adaptation and improved glycemic profile.38,39 The findings of the present study are also in line with previous studies showing a marked VO2peak improvement in the T1D group undertaking the exercise intervention.40,41
Reduced compassion, a condition characterized by reduced access to the comfort system (safety), is associated with reduced HRV activity. 42 It is known from previous research that compassionate mind training can increase baseline HRV and reduce symptoms of depression, anxiety, stress, and fears of self-compassion.43,44 According to the present study, MSCT intervention led to increases in HF, RMSSD, and PNN50 parameters and a decrease in LF/HF indicating an increase in the PNS factors of the ANS and its greater control over the heart at rest. Consistent with these findings, Svendsen et al. found higher levels of self-compassion in individuals with higher HRV and concluded that the induction of a state of compassion increased HRV proportional to the increased positive affect of the soothing system. 45
It is possible that MSCT facilitates behavioral changes through creating care mindfulness, and other processes of inner kindness, which can be construed as a physio-psychological intervention. 46 Alternatively, cultivating compassion could have a soothing effect on the PNS and lead to increased HRV through the safety system. 47
Finding of the present study on the positive impact of compassion intervention in reducing blood glucose level aligns with the results of Friis et al. who reported reduced HbA1c following a self-compassion training program as an indicator of ANS improvement in T1D patients.17,48 Poor glycemic control has been suggested as a contributing factor to reduced HRV parameters and development of ANS dysfunction. 49 This could be described by the occurrence of neuro-metabolic adaptations in these patients, as such a strong glycemic control facilitates increased HRV parameters and reduced ANS disturbance leading to improved PNS factors and greater control over HRV during rest.
Findings of the present study also suggest the occurrence of a reinforcement interaction in T1D following a combined exercise and compassion training. Several studies have reported the effect of regular physical activity in reducing the risk of mortality in patients with diabetes due to enhanced blood glucose and lipid control, improved insulin signaling, reduced inflammation, and improved vascular function.50,51 In addition to physiological markers, diabetes distress is a clinically significant psychosocial stressor that may contribute to the cardiovascular health of individuals with T1D. Hence, psychological care is recognized as a standard component of diabetes care.52,53
Our findings demonstrate a linear relationship between HRV and VO2max, which is significantly influenced by the overall sympathetic-vagal balance, resulting in decreased sympathetic tone, increased PNS tone, and HRV levels. Furthermore, exercise training increases baroreflex sensitivity and HRV, along with improved VO2max, suggesting that physical activity can improve autonomic balance and cardiovascular risk in patients with diabetes.54,55 Concurrent self-compassion training could increase HRV response and potentially strengthen the ability to engage with difficult emotions in psychotherapy. 56 In this way, people with diabetes learn to have more compassion for themselves and to be more aware of their life conditions. Therefore, incorporation of a compassion component into the intervention program to increase mindfulness and self-compassion may lead to more efficient promotion of health-related behaviors, and natural physical and mental health, and ultimately improve self-care behaviors and reduce the glycemic index.
Limitations
The generalizability of the results may be limited because of the relatively controlled blood glucose and diet in T1D patients. Considering the sensitivity of the effect of gender on HRV in the adolescent age group, the present study focused only on male participants. 39 Future studies of female and mature participants are needed to expand relevant knowledge. Data collection, position, and HRV analysis (time, method) were not identical across studies, which may have affected the comparisons.
Conclusion
The findings of the present research suggest that a combined exercise training and focused therapy of compassion may be considered an effective modality for more optimal enhancement in the HRV parameters, parasympathetic components in particular, of adolescents with T1D. Adolescents with T1D may benefit from gaining appropriate exercise skills and self-compassion training methods and encouragement to engage in these activities to improve their health. Parents, healthcare providers, and counselors involved in the management of T1D may consider the amalgamation of exercise and self-compassion training for enhanced blood glucose control and self-care behaviors. Further research is needed to further investigate the effectiveness of this strategy in preventing and slowing down the progression of cardiovascular disease in children and adolescents with T1D.