
Abstract
Background:
Several negative outcomes have been documented post-COVID-19 pandemic, including many cardiometabolic abnormalities associated with metabolic syndrome (MetS).
Objectives:
The study aims to evaluate the prevalence of MetS among Jordanian adults post-COVID-19 and compare these results with previous findings.
Design:
A cross-sectional study.
Methods:
A total of 5188 adults of both sexes (age >18 years) were recruited. Body weight, height, waist circumference (WC), fasting plasma glucose, high-density lipoprotein cholesterol (HDL-C), triglycerides, and blood pressure were measured.
Results:
The crude prevalence of MetS, using both the International Diabetes Federation (IDF) and the Adult Treatment Panel III (ATP III) diagnostic criteria, was 42.9% (32.5% in males and 46.9% in females). There was no change in the crude prevalence of MetS among the total population between 2017 (48.2% and 44.1%) and 2024 (48.1% and 45.0%) by IDF and ATP III criteria, respectively (p > 0.05). In comparison, the age-standardized prevalences were 44.6% (95% CI 43.3%–45.9%) for ATP III and 47.7% (95% CI 46.4%–49.0%) for IDF. The main contributing factors for MetS, according to ATP III, were low HDL-C (65.4%) and enlarged WC (60.4%). However, according to IDF criteria, enlarged WC (76.9%) was followed by low HDL-C (65.4%).
Conclusion:
Although the crude prevalence of MetS stayed relatively stable before and after COVID-19, age-standardized data show a noticeable upward trend, pointing to an increasing cardiometabolic burden. These findings highlight the urgent need for wide-ranging, population-level strategies that emphasize lifestyle modifications, screening, and early intervention to address metabolic risks.
Plain Language Summary
The study investigates the prevalence of metabolic syndrome (MetS) among adults in Jordan after the COVID-19 pandemic and compares it with earlier data. It involved 5,188 participants, measuring weight, height, waist circumference, fasting plasma glucose, cholesterol, triglycerides, and blood pressure. The overall prevalence of MetS was found to be 42.9%, with higher rates in females than males. Key factors contributing to MetS included low HDL cholesterol and enlarged waist circumference. There was no significant change in prevalence between 2017 and 2024, indicating COVID-19 did not impact MetS rates. Further studies are needed to explore related factors and long-term effects.
Introduction
Metabolic syndrome (MetS) ranks as one of the major public health problems; it is a clustering of metabolic disorders, including insulin resistance, central fat accumulation, dyslipidemia, and hypertension. It considerably increases the risk of developing type 2 diabetes (T2D) and cardiovascular disease (CVD).1,2 This complex syndrome is associated with higher morbidity and mortality rates, which has a sizable socioeconomic impact on global health. 3 Despite MetS’s significant progress concerning research, the complex interaction between the genetic and environmental components influencing MetS has remained poorly defined, emphasizing the need for further research to mitigate its impact on public health.1,2
The International Diabetes Federation (IDF) and the National Cholesterol Education Program (NCEP) Adult Treatment Panels III (ATP III) criteria are the most extensively used and appreciated definitions of the MetS. 4 Generally, it is agreed that having three or more of the following conditions is the definition for this syndrome: central adiposity presented by enlarged waist circumference (WC), increased triglycerides (TG), low high-density lipoprotein-cholesterol (HDL-C), increased blood pressure (BP), and elevated fasting plasma glucose (FPG). Together, these parameters define the presence of MetS and help identify a higher risk for CVD and T2D.5,6
Moreover, individuals with MetS, regardless of any previous CVD history, have double the risk of mortality, developing a stroke with a two- to four-fold, and a three- to four-fold higher risk of myocardial infarction compared to those without the syndrome. 7 Diet, smoking, physical inactivity, family history, genetic background, and education can all significantly influence the occurrence of MetS. Similarly, high body mass index (BMI) (>30 kg/m2), accompanied by a sedentary lifestyle, is associated with developing MetS. 8
Over the past few decades, the MetS has become increasingly prevalent worldwide, particularly in developing nations. 9 It has been noted that having multiple MetS components may increase a young adult’s risk of developing MetS later in life. 10 For instance, according to the IDF, approximately 25% of the global population is estimated to have MetS. 11 The prevalence of MetS differs based on the diagnostic criteria, leading to variation across ethnic groups. These estimates are heavily influenced by factors such as sex, age, race, and environmental and socio-cultural conditions. 1
According to the Centers for Disease Control and Prevention, since the term was first coined in the 1980s, the prevalence of MetS has increased by 35% in the United States in 2012. 12 Additionally, the prevalence of MetS differed across countries and study periods. In Turkey, it ranged from 2.2% to 44%, while in Saudi Arabia, it ranged from 16% to 41%. Pakistan saw rates from 14% to 63%, Qatar from 26% to 33%, Kuwait from 9% to 36%, the Emirates from 22% to 50%, Iran from 6% to 42%, and Yemen up to 23%. 13 In Jordan, the prevalence of MetS in 2015 was 51% according to IDF criteria (46.4% and 55.3% in males and females, respectively). 14 In 2020, the crude prevalence according to the IDF criteria was 48.2% (52.9% and 46.2% among males and females, respectively) and 44.1% (51.4% and 41% among males and females, respectively) according to the ATP III criteria. 6
COVID-19 constraints, such as house isolation, have caused individuals worldwide to become less active and adopt worse eating habits in recent years. 15 Researchers found that the most common COVID-19 outcome was obesity, which was influenced by sedentary lifestyles, physical inactivity, high levels of behavioral stress, depression, anxiety, low mood, and poor eating habits. 16 Moreover, COVID-19 modifies energy metabolism, leading to dysglycemia and potentially long-lasting effects, which can exacerbate T2D. 17 Also, there has been growing concern about COVID-19’s potential impact on the cardiovascular system and its relation to arterial hypertension, BP, hyperlipidemia, and cardiovascular autonomic dysfunction. 18 Liu and Lou 19 conclude that the understanding of long-lasting COVID-19 is advancing, but more research is necessary, particularly for patients with MetS. These patients should focus on managing blood sugar and lipids to prevent symptom escalation. Data on the role of MetS in long COVID-19 are vital for improving patient care and public health policies. 19
To the researchers’ knowledge, no studies have been conducted in Jordan to assess the prevalence of MetS among Jordanian adults since the onset of the COVID-19 pandemic. Thus, this study aimed to investigate the “updated” prevalence of MetS post-COVID-19 among Jordanian adults and the degree of difference between pre- and post-COVID-19 prevalences.
Materials and methodology
Study design and participants
Between July 2022 and May 2024, a population-based cross-sectional survey was conducted in the Hashemite Kingdom of Jordan. Three public governmental hospitals in Jordan’s central regions were used to recruit the target sample. Data were gathered from outpatients and/or caregivers who frequently visited these institutions for follow-up care. Participants were randomly selected; Jordanian adults aged 18 or older who were willing to participate were included. Due to the nature of the study, participants, regardless of their health status, were selected, including those with T2D, CVD, hypertension, and dyslipidemia. On the other hand, individuals under 18 years of age, pregnant or nursing females, and non-Jordanian participants were excluded from the study. Furthermore, anyone who met any of the following criteria was also excluded: someone with dementia, terminal disease, deafness, or mental health problems; those who take any medications for chronic diseases had been excluded. Thus, after excluding 771 participants, the remaining sample comprised 5188 participants (1462 males and 3726 females).
The Hashemite University’s Institutional Review Board (No. 19/1/2022/2023) and the Jordanian Ministry of Health (MBA, IRB, 20219-1/12/2022) reviewed and approved the study protocol by the Helsinki Declaration. Each willing and qualified subject provided informed written consent before enrolling in the study and received a clear explanation of the research goals and procedures, potential risks and benefits, and information about confidentiality and the right to withdraw. Following participant consent, a face-to-face interview was completed to collect socio-demographic data using a standardized questionnaire. Data on overall health and inquiries about any other health problems were included. During these interviews, anthropometric measurements were taken. However, the biochemical data and BP measurements were collected from Hakim Medical Records.
Data collection
Under the lead investigator’s guidance, a competent nutritionist conducted face-to-face interviews, collected the required information, and verified the accuracy of the collected anthropometric data. The daily activities, including moderate- and high-level activities, were assessed and considered to meet physical activity (PA) requirements if participants performed 150 min per week of moderate-intensity PA, 75 min per week of vigorous-intensity PA, or an equivalent combination of both. 20 The participant’s height (in cm) and weight (in kg) were measured to calculate their BMI using Quetelet’s method. 21 The World Health Organization categories were then used to classify the BMI results. 22 The WC was measured to the nearest 0.1 centimeters using non-stretchable tape at the narrowest point between the umbilicus and the rib cage at the end of a normal expiration. FPG levels and serum lipids (TG and HDL-C) in mg/dL were obtained from Hakim’s online medical system (Government Medical Archive Program for Jordanians). BP measurements were also obtained from patients’ hospital medical records.
MetS determination
Clinical criteria for the diagnosis of MetS were established by the Adult Treatment Panel III (ATP III) of the NCEP. According to the ATP III, MetS requires no single factor for diagnosis. Instead, they made the presence of three of the five factors the basis for establishing the diagnosis, and these components were assessed for each participant. The components include enlarged WC: ⩾102 cm for males and ⩾88 cm for females; FPG ⩾100 mg/dL or using of hypoglycemic agents, elevated BP; systolic BP ⩾130 mmHg or diastolic BP ⩾85 mmHg or on BP-lowering medication, TG ⩾150 mg/dL or using medication for elevated TG, and HDL-C <40 mg/dL for males and <50 mg/dL for females or taking any medication for lower HDL-C levels. 10 On the other hand, the IDF modified the ATP III definition. 23 The IDF clinical definition requires abdominal obesity for diagnosis. When such is present, two additional components originally listed in the ATP III definition are sufficient for diagnosis. Thus, IDF recognized and emphasized ethnic differences in the correlation between abdominal obesity and other MetS components. For this reason, criteria for abdominal obesity were specified by nationality or ethnicity based on the best available population estimates. For people of European origin (Europid), the IDF specified thresholds for abdominal obesity to be WC ⩾94 cm in males and ⩾80 cm in females. 23
Statistical analysis
Missing data were assessed for all study variables before analysis. Participants with missing values for the exposure, outcome, or key covariates were excluded from the relevant analyses using a complete-case approach. The overall proportion of missing data was low (<5% across variables); therefore, no imputation was performed. All analyses were conducted using available complete observations. Data were analyzed using IBM SPSS Statistics (IBM SPSS Statistics for Windows, Version 23.0, IBM Corp, Armonk, NY). A chi-square (χ2) was performed to test the differences in socio-demographic and lifestyle factors between subjects who have MetS and those who do not have MetS, as well as for the presence of any abnormality of each MetS component. The age-standardized prevalence rates were calculated to enable comparisons across surveys and with studies from other countries, using the world population as the standard. All estimates are presented with 95% confidence intervals (95% CI) to indicate their precision. Findings with a p-value of <0.05 were considered to be statistically significant.
Results
The general characteristics of the study participants are shown in Table 1. The majority of participants were females (71.8%), married (72.3%), and had an education level <B.Sc. (72.0%), as well as 39.4% of the participants were within the age group of 36–50 years, 44.4% had a family income less than 300 JD, 39.3% were classified as former and negative smokers, and 59.1% were physically inactive. Based on BMI, the prevalence of normal body weight, overweight, and obesity was 20.4%, 28.9%, and 48.9%, respectively.
General characteristics of the study population.

Current smoker: An individual who has smoked at least 100 cigarettes in their lifetime and who currently smokes cigarettes, either daily or on some days, at the time of assessment.
BMI classification: Thinness (BMI <18.5 kg/m2); Normal weight (BMI between 18.5–24.9 kg/m2); Overweight (BMI between 25–29.9 kg/m2); Obese I (BMI between 30–34.9 kg/m2); Obese II (BMI between 35–39.9 kg/m2); and Obese III (BMI >40 kg/m2).
BMI, body mass index; B.Sc., Bachelor’s degree; JDs, Jordanian Dinars (1 JD = 1.4 US dollars).
Table 3 presents the socio-demographic characteristics and the crude prevalence of MetS according to the ATP III and IDF criteria. The crude prevalence of MetS based on both criteria (ATP III and IDF) has been significantly higher among females (76.8% vs 77.3%), age group 36–50 years (42.9% vs 43.1%), being married (78.7% vs 78.9%), an educational level less than B.Sc. degree (77.9% vs 76.8%), family income less 300 JD (52.7% vs 51.4%), former and negative smokers (41.2% vs 41.3%), physically inactive (62.8% vs 62.0%), overweight (24.8% vs 28.4%), obese I (33.2% vs 33.1%), and obese II (22.9% vs 21.5%), as defined by ATP III versus IDF criteria, respectively (p < 0.001). In contrast, prevalence rates were significantly lower among males, the youngest, singles, those with higher educational attainment, those earning over 600 JD, non-smokers, physically active individuals, those with a lower BMI, and those with a normal body weight (p < 0.001).
As presented in Table 2, based on IDF, the age-standardized prevalence for the total population was 47.7 (46.4–49.0), for males 38.7% (36.3–41.4), and 50.9% (49.3–52.5) for females, while according to the ATP III criteria, the total age-standardized prevalence was 44.6 (43.3–45.9); 37.3% (35.0–39.7), and 47.2% (45.6–48.8), for males and females, respectively.
Age-standardized sex-specific prevalence rates of MetS and its components in Jordan, using ATP III and IDF criteria.
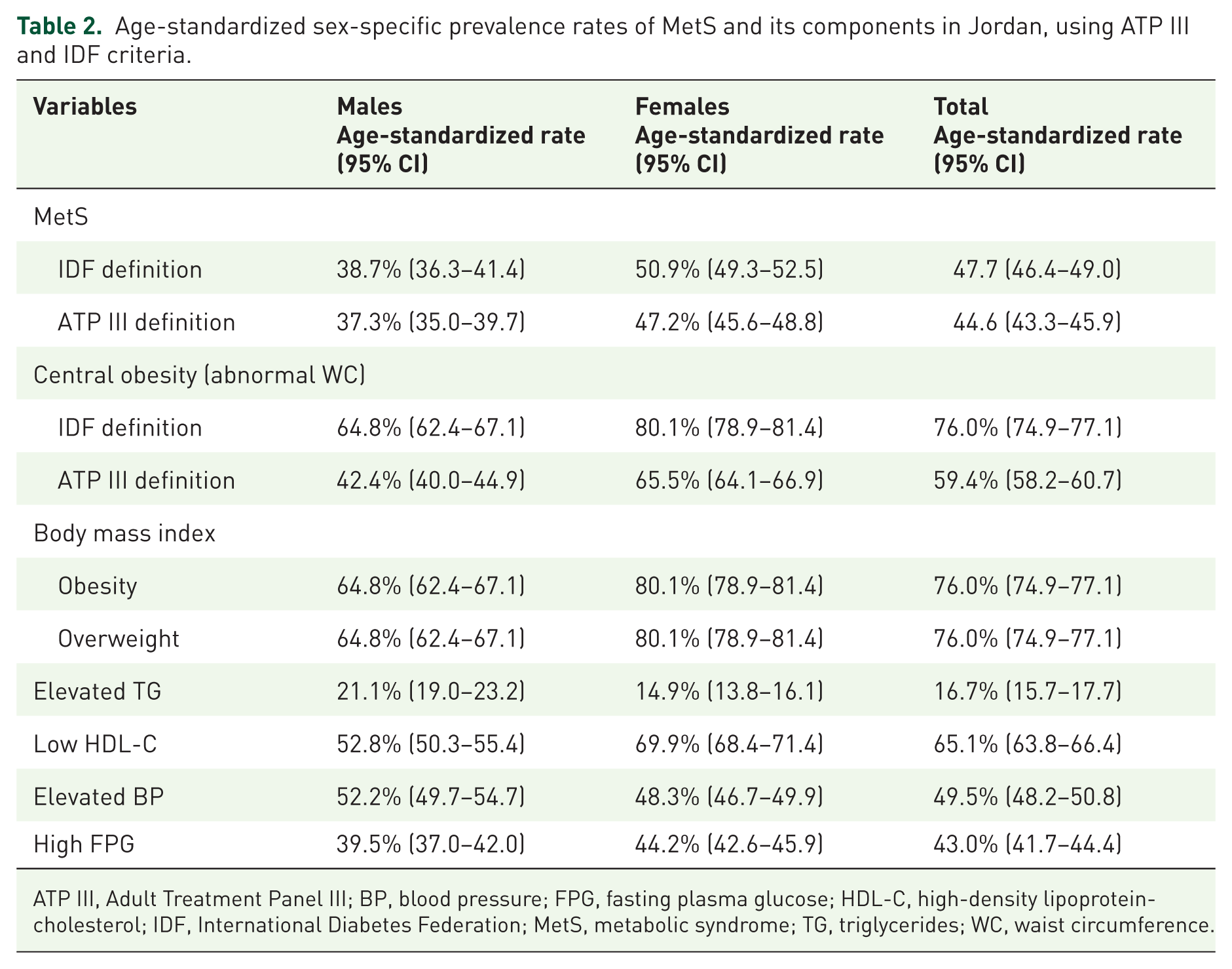
ATP III, Adult Treatment Panel III; BP, blood pressure; FPG, fasting plasma glucose; HDL-C, high-density lipoprotein-cholesterol; IDF, International Diabetes Federation; MetS, metabolic syndrome; TG, triglycerides; WC, waist circumference.
The crude prevalence of MetS and its associated metabolic abnormalities among the study population, stratified by sex and age, is summarized in Table 3. The highest MetS prevalence age group was identical for both criteria; it was at age 36–50 years among males (46.0% and 48.1%), while females were in the age group of 51–65 years (65.3% and 67.5%) for ATP III and IDF criteria, respectively (p < 0.001). The prevalence of MetS among females increased significantly with age, according to both criteria (ATP III and IDF), until age 65 (p < 0.001). It tends to rise from 26.8% in females aged 19–35 years to 65.3% in those aged 51–65 years and then declined to 48.3% in those aged >65 years by the ATP III criteria (p < 0.001), while with depending on IDF criteria, the MetS prevalence was 31.6% in those aged 19–35 years and continued to rise to 67.5% in 51–65 years age group and eventually dropped at age 65 years to reach 50.6% (p < 0.001) (Table 4).
The socio-demographic characteristics and the crude prevalence of MetS based on ATP III and IDF criteria definitions.
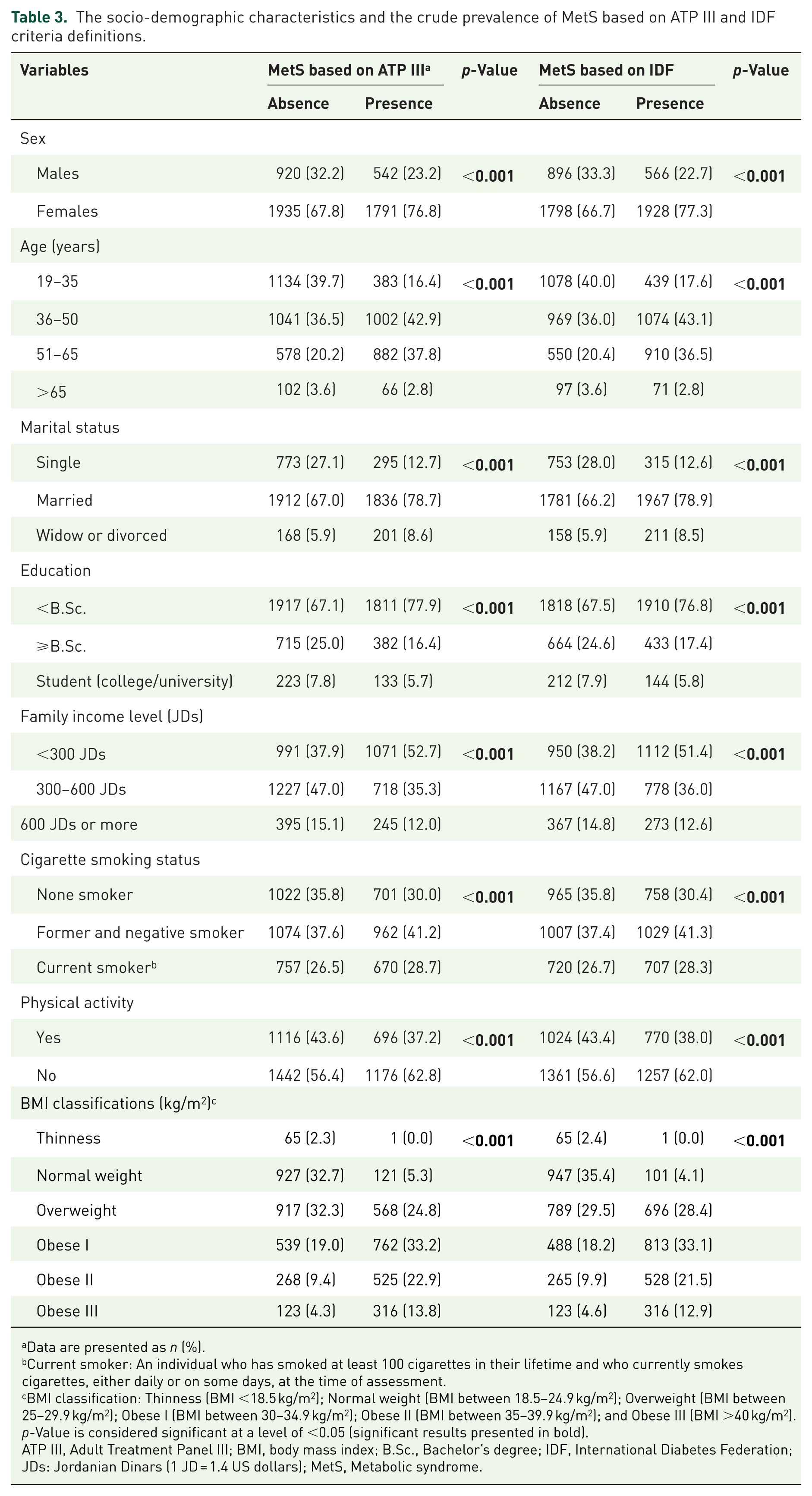
Data are presented as n (%).
Current smoker: An individual who has smoked at least 100 cigarettes in their lifetime and who currently smokes cigarettes, either daily or on some days, at the time of assessment.
BMI classification: Thinness (BMI <18.5 kg/m2); Normal weight (BMI between 18.5–24.9 kg/m2); Overweight (BMI between 25–29.9 kg/m2); Obese I (BMI between 30–34.9 kg/m2); Obese II (BMI between 35–39.9 kg/m2); and Obese III (BMI >40 kg/m2).
p-Value is considered significant at a level of <0.05 (significant results presented in bold).
ATP III, Adult Treatment Panel III; BMI, body mass index; B.Sc., Bachelor’s degree; IDF, International Diabetes Federation; JDs: Jordanian Dinars (1 JD = 1.4 US dollars); MetS, Metabolic syndrome.
The crude prevalence of MetS and its abnormal components stratified by age and sex based on IDF and ATP III criteria. a .

The data represent the abnormal measures.
Data are presented as n (%).
p-Value is considered significant at a level <0.05 (significant results presented in bold).
ATP III, Adult Treatment Panel III; BP, blood pressure; FPG, fasting plasma glucose; HDL-C, high-density lipoprotein cholesterol; IDF, International Diabetes Federation; MetS, metabolic syndrome; TG, triglycerides; WC, waist circumference.
In the 36–50-year age group, both males and females have the highest prevalence of high FPG levels (48.1% and 51.3%, respectively) (p < 0.001). Additionally, within the same age group, 59% of males have low HDL-C (p < 0.001), the highest proportion, whereas among females aged 65 years and older, 79.8% have low HDL-C (p = 0.001). Hypertriglyceridemia and high BP were significantly higher in the age group of 51–65 years for both sexes (p < 0.001). Based on ATP III criteria, the prevalence of enlarged WC increased with age in males and females (p < 0.001), as did the prevalence of enlarged WC defined by the IDF criteria in females. Still, males aged 51–65 years have the highest proportion of enlarged WCIDF, at 75.4% (p < 0.001; Table 4).
Figure 1(a) and (b) compares the MetS crude prevalence across various years according to the IDF and ATP III in Jordan. Until the development of this manuscript, no studies on the recent prevalence of MetS (post-COVID-19) were available, although multiple studies had been conducted before the COVID-19 pandemic. In this study, in 2024, the total crude prevalence based on IDF is 48.1% (38.7% for males and 51.7% for females), compared to 51.0% (46.4% for males and 55.3% for females) in 2015 (pre-COVID-19), 14 and 48.2% (52.9% for males and 46.2% for females) in 2017 (pre-COVID-19). 6 There was no substantial difference in the crude prevalence of MetS, as defined by the IDF, between 2015 and 2024 (p = 0.6713; p = 0.321 for males and p = 0.432 for females). Based on ATP III (Figure 1(b)), the total current prevalence (post-COVID-19) is 45.0% (37.1% for males and 48.1% for females), compared to 37.4% (31.7% for males and 41.0% for females) in 2011, 24 and 44.1% (51.4% for males and 41.0% for females) in 2017 (pre-COVID-19). 6 Remarkably, across years (2011–2024), these proportions did not show statistically significant differences in the crude MetS prevalence defined by the ATP III criteria (p = 0.252), nor among males (p = 0.463) or females (p = 0.321).

Comparison of the MetS crude prevalence based on (a) IDF and the MetS prevalence in Jordan based on ATP III (b) across various years.
Table 5 presents the overlap in MetS prevalence using two criteria: IDF and ATP III. The prevalence of MetS among Jordanian adults has varied across studies conducted before and after the COVID-19 pandemic. Post-COVID-19 findings from the current study showed similar crude estimates: 48.1% (38.7% males; 51.7% females) according to IDF and 45.0% (37.1% males; 48.1% females) according to ATP III. When applying both criteria simultaneously, the crude prevalence was 42.9% (32.5% males; 46.9% females). However, after age-standardization, the prevalence increased to 47.7% (95% CI: 46.4–49.0) using IDF criteria and 44.6% (95% CI: 43.3–45.9) using ATP III, indicating a clear rise compared with earlier standardized estimates from 2017 (44% IDF; 39.9% ATP III).
Prevalence of MetS among Jordanian adults by year of data collection, pre- and post-COVID-19 pandemic.

ATP III, Adult Treatment Panel III; IDF, International Diabetes Federation; MetS, metabolic syndrome.
Discussion
The age-standardized prevalence for the total population was 44.6% (95% CI 43.3%–45.9%) according to ATP III, and 47.7% (95% CI 46.4%–49.0%) according to the IDF. In comparison, the crude prevalence for both criteria was 42.9% (32.5% for males and 46.9% for females). According to the ATP III, 45.0% of individuals have MetS, with key contributing factors including low HDL-C (65.4%) and enlarged WC (60.4%). The IDF criteria showed a slightly higher prevalence of 48.1%, with enlarged WC being the most common abnormality at 76.9%. The prevalence was notably higher among women, those aged 36–50, married individuals, less-educated people, lower-income families, former smokers, and those who were inactive or obese. The study found that the age-standardized prevalence was higher than previously reported, increasing from 44% to 47.7% (IDF criteria) and from 39.9% to 44.6% (ATP III criteria).
In Jordan, pre-COVID-19 studies reported crude MetS prevalence ranging from 36.3% to 48.2% using ATP III or IDF definitions. Early estimates included 37.4% (31.7% in males; 41.0% in females) reported by Yasein and Masa’d (2004), 36.3% (28.7% males; 40.9% females) by Khader et al. (2005), and 36.3% (38.7% males; 30.6% females) among adult employees in Obeidat et al. (a) (2007). Obeidat et al. (b) later reported a higher crude prevalence of 51.0% according to IDF criteria. Ajlouni et al. (2020) reported an age-standardized prevalence was 44.0% (95% CI: 42.7–45.4) for the IDF definition and 39.9% (95% CI: 39.6–41.2) for the ATP III definition. Immediately before the pandemic, Al-Shami et al. (2018–2019) documented a crude MetS prevalence of 42.5% (38.5% males; 47.1% females).6,14,24-27 Compared with Alajlouni et al.’s findings, the current age-standardized prevalences are higher. Contrary to these findings, Kang et al. reported a significant decrease in the prevalence of MetS among Korean adults before and after the COVID-19 pandemic, from 26.7% to 30.2% (p = 0.001). They hypothesized that these differences might have been caused by changes in dietary and PA patterns during the pandemic. 28 Interestingly, in Korea, Jeong et al. found that, despite no clinically significant changes in body weight or BMI, MetS, its components, and fat distribution worsened dramatically following the adoption of social distancing and lockdowns. 29 However, Mamudu et al. found that the odds of metabolic conditions increased only among certain subgroups of US adults during the pandemic. 30
Consistent with these findings, Auriemma et al. reported that, at the end of the COVID-19 lockdown, the prevalence of MetS increased significantly from 14.9% to 27.0% (p < 0.0001) and concluded that the outbreak led to a rapid increase in MetS prevalence in Italy. 31 Moreover, Hsieh et al. estimated that MetS prevalence among Taiwanese healthcare workers significantly increased from 20.9% to 28.7% during the pandemic (p < 0.001). 32 This was also reflected among the Chinese population; Xu et al. found that the prevalence of MetS in 2020 was 18.6%, which is notably higher than the 15.7% observed before the pandemic. Moreover, following the COVID-19 lockdowns, the number of abnormal MetS components was significantly higher than in 2018 and 2019. However, changes in all MetS components, including DBP, did not differ notably between men and women in 2019–2020 and 2018–2019. 33
Regardless of the pandemic, the overall prevalence of MetS among Jordanian adults is recognized as high relative to that in other countries. Depending on the definition, the prevalence of MetS ranged from 12.5% (95% confidence interval (CI): 10.2–15.0) to 31.4% (95% CI: 29.8–33.0) worldwide, with the Americas and the Eastern Mediterranean regions having notably higher prevalence. 34 Using the IDF criteria, the prevalence of MetS was 31.6% and 39.9% by the ATP III criteria in Saudi Arabia. 35 Meanwhile, in Vietnam, the pooled MetS prevalence among adults was 16.1%. 36 Also, the incidence of MetS ranged from 17.2% to 27.2% across different criteria in Iran. 37 It is important to highlight the crucial role ethnicity plays in the variation in MetS prevalence, as shown in multiple studies.23,38,39
Consistent with this finding, among Jordanian adults, Obeidat et al., Ajlouni et al., and Al-Shami et al. identified lower HDL-C as the most common abnormality in their study populations (56.2%, 59.1%, and 66.0%, respectively), all using the ATP III criteria.6,26,40 Earlier, Yasein and Masa’d documented the enlarged WC as the highest prevalent MetS component in the total sample (61.6%) by the ATP III criteria. 24 Using the IDF criteria, Obeidat et al. and Ajlouni et al. revealed that the prevalence of enlarged WC in the total sample was 71.6% and 74.6%, respectively.6,14 Internationally, Dang et al. found that the most prevalent components were low HDL-C (34.1%) and high TGs (33.3%) among the Vietnamese population. 36
The prevalence trend for males declined over the years (pre- and post-COVID-19), whereas it increased significantly among females. Females had a substantially higher prevalence of MetS in the Jordanian adult population, as documented by numerous studies.14,24,26,27 Additionally, several studies have been reported worldwide.36,37 Mamudu et al. found no significant differences in metabolic conditions between males and females in U.S. adults during and before the pandemic. 30 The same result was reported by Jeong et al. in Korea. 29
Regarding age, Khader et al. and Yasein and Masa’d reported that the prevalence generally increased with age in the total sample and among both sexes using the ATP III criteria.24,27 Obeidat et al. documented that MetS prevalence positively correlated with age in both sexes, using the ATP III criteria; they highlighted that individuals aged 45–54 years were 3 times more likely to have MetS than younger age groups in a sample of Jordanian employees. 40 Consistent with Obeidat and colleagues, the MetS prevalence increased significantly with increasing BMI (25.5 ± 4.3 kg/m2 without MetS vs 31.4 ± 5.1 kg/m2 with MetS). 14 A consistent finding across studies is that the prevalence of MetS is strongly weight-dependent.36,41
In line with the present findings, Obeidat et al. found that the odds ratio for MetS among Jordanian adults was significantly higher with increasing age, among current smokers, and among those with higher BMI, which aligns with our results. 40 Furthermore, significant decreases in PA were observed with the exacerbation of all MetS components. 29 Besides, Mamudu et al. documented that former smokers were more likely to have metabolic problems before and during the pandemic, respectively, than those who had never smoked; furthermore, compared to people who participated in at least one moderate-intensity PA per week during the pandemic, the prevalence of metabolic conditions was greater among those who did not. 30
The COVID-19 pandemic has had a profound impact on the social, psychological, and physical health of people worldwide. Therefore, the documented increase in MetS prevalence following COVID-19 is well established in the literature. We believe that the overall minimal or fixed increase in prevalence among Jordanians may be attributable to the interval between the outbreak and the study, which may have provided sufficient time to adopt healthier lifestyles, reduce weight, address modifiable risk factors, or manage individual metabolic abnormalities. All of these actions can help lower or stabilize the prevalence of MetS.
Strengths and limitations
This will be the first study identifying the recent prevalence of MetS and its components among Jordanian adults, which could help broaden our understanding of the impact of the COVID-19 pandemic on MetS, assess the role of socio-demographic variables in MetS occurrence, evaluate the efficiency of using different criteria to define the MetS in sharpening the picture of the actual MetS situation in Jordan, help with the design of appropriate health treatments, the creation of focused educational initiatives, and to evaluate the effectiveness of such interventions. However, the current study is limited by its cross-sectional design, which precludes establishing both a causal relationship and a historical link between the variables under study and the disease outcome. Additionally, this study did not account for dietary and other psychological and social factors. At the same time, the study sample is derived from out-patient clinic attendees; therefore, it is not representative of the general population, is sex-imbalanced, and lacks dietary and psychological data. Data on COVID-19 infection history and vaccination status were not collected, and their incorporation into the analysis was not investigated.
Conclusion
This study shows that MetS is very common and increasing among Jordanian adults after COVID-19, with age-standardized rates of 44.6% (ATP III) and 47.7% (IDF)—both higher than crude estimates and previous national figures. Central obesity and low HDL-C were the most common issues, especially under the IDF criteria. MetS was more frequent in females, adults aged 36–50, people with lower socioeconomic and educational levels, those who are physically inactive, and overweight or obese individuals. While crude MetS prevalence remained relatively stable before and after COVID-19, age-standardized data reveal a clear upward trend, indicating a growing cardiometabolic burden. These results underscore the urgent need for broad, population-level strategies focused on lifestyle changes, screening, and early treatment of metabolic risk factors. The study also emphasizes the importance of targeted prevention efforts and public health campaigns to address the rising rates of MetS. Healthcare providers can enhance overall health worldwide by increasing awareness of MetS risk factors and implementing effective interventions. This research is expected to deepen our understanding of MetS, leading to more effective treatment and prevention strategies.
Supplemental Material
sj-docx-1-tae-10.1177_20420188261431012 – Supplemental material for Trends in the prevalence of metabolic syndrome among Jordanian adults following COVID-19
Supplemental material, sj-docx-1-tae-10.1177_20420188261431012 for Trends in the prevalence of metabolic syndrome among Jordanian adults following COVID-19 by Islam Al-Shami, Buthaina Alkhatib, Lana Agraib and Asem Taher Shawabkeh in Therapeutic Advances in Endocrinology and Metabolism