
Abstract
Objectives:
Previous studies present conflicting evidence on the relationship between hepatocellular damage biomarkers and dementia risk. While elevated serum transaminases have been associated with mild cognitive impairment, other studies link lower transaminase levels and reduced high-density lipoprotein-cholesterol levels to increased risk of cognitive decline. This study investigated the association between serum transaminase-to-high-density lipoprotein-cholesterol ratios and probable dementia among people living with HIV on antiretroviral therapy.
Methods:
We conducted a secondary data analysis using a dataset from a cross-sectional study conducted among 377 people living with HIV on dolutegravir-based antiretroviral therapy in southwestern Uganda. Probable dementia was screened using the brief Community Screening Instrument for Dementia and defined as a Community Screening Instrument for Dementia cognitive score ⩽4. Serum alanine aminotransferase/high-density lipoprotein-cholesterol and aspartate aminotransferase/high-density lipoprotein-cholesterol ratios were calculated from the respective serum transaminases and high-density lipoprotein-cholesterol divided into tertiles. We used logistic regression to assess the association between the independent variables and probable dementia.
Results:
The median age of the study participants was 44 years (interquartile range: 30–59), with 56.2% being female. The median total cholesterol/high-density lipoprotein-cholesterol levels were significantly higher in participants with probable dementia compared to those without (3.86 versus 3.22, p = 0.03). Aspartate aminotransferase/high-density lipoprotein-cholesterol and alanine aminotransferase/high-density lipoprotein-cholesterol levels were also higher among participants with probable dementia compared to those without, although the differences did not reach statistical significance. In the fully adjusted model, compared to participants in the first tertile of aspartate aminotransferase/high-density lipoprotein-cholesterol ratio, the odds of probable dementia were higher in the second tertile (adjusted odds ratio: 1.71; 95% confidence interval: 0.62–4.74; p = 0.301) and significantly elevated in the third tertile (adjusted odds ratio: 4.48; 95% confidence interval: 1.15–17.46; p = 0.031).
Conclusions:
The findings suggest that an elevated aspartate aminotransferase/high-density lipoprotein-cholesterol ratio is significantly associated with probable dementia among people living with HIV on dolutegravir-based antiretroviral therapy. A high aspartate aminotransferase/high-density lipoprotein-cholesterol ratio is potentially associated with cognitive decline in this population.
Keywords
Introduction
The increasing availability of antiretroviral therapy (ART) has transformed HIV from a fatal disease to a manageable chronic condition.1–3 However, the longer lifespan of people living with HIV (PLWH) has revealed new challenges, particularly the increasing prevalence of non-communicable diseases, including metabolic syndrome (MetS), neurodegenerative diseases, and liver dysfunction.4–7 One area of growing concern is the risk of cognitive impairment, specifically mild cognitive impairment (MCI) and dementia, among PLWH on ART.8–11 This concern extends to those on dolutegravir (DTG)-based regimens. DTG, an integrase strand transfer inhibitor (INSTI), has been praised in some studies as a highly effective drug. However, other studies indicate that DTG and other INSTIs are associated with significant weight gain and a higher incidence of dyslipidemia compared to non-nucleoside reverse transcriptase inhibitors such as efavirenz.12,13 Further still, MCI, often considered a transitional stage between normal aging and dementia, particularly Alzheimer’s disease,14,15 has been linked to various metabolic and liver biomarkers.15–18 This association suggests the potential for using these biomarkers to predict cognitive decline and dementia risk.
PLWH on ART, especially those on DTG, exhibit higher risks of developing MetS,19–21 a cluster of conditions including central obesity, dyslipidemia, hypertension, and insulin resistance.12,22 These metabolic abnormalities have been implicated in both cardiovascular disease and liver dysfunction, particularly non-alcoholic fatty liver disease (NAFLD).23–26 The presence of NAFLD in PLWH, coupled with altered lipid metabolism, contributes to liver enzyme elevation, commonly measured through serum alanine aminotransferase (ALT), aspartate aminotransferase (AST), and gamma-glutamyl transferase (GGT). Elevated levels of these enzymes have long been associated with liver damage and metabolic derangements.23–25
Liver biomarkers have been increasingly correlated to cognitive health.16,27–34 Some studies suggest that elevated serum ALT and AST levels are associated with an increased risk of MCI and dementia,33,35 possibly through mechanisms involving oxidative stress and neuroinflammation. 36 However, other studies contradict these findings, showing that lower ALT and AST levels might increase the risk of dementia, raising questions about the role of liver enzymes in neurodegenerative diseases.36,37 These conflicting findings indicate the need to explore further the relationship between liver biomarkers and cognitive impairment further, particularly in populations with high MetS and NAFLD prevalence, such as PLWH on ART.
High-density lipoprotein-cholesterol (HDL-C) has also emerged as a key biomarker in dementia research.38–40 Higher HDL-C levels are known to provide protective vascular and neuroprotective effects, including reducing inflammation, promoting endothelial nitric oxide synthase activity, and inhibiting the accumulation of amyloid-beta protein, which is involved in Alzheimer’s disease pathology.40–42 Low HDL-C levels, conversely, have been associated with an increased risk of dementia, particularly in individuals with metabolic disorders.40,43 This has led researchers to propose that HDL-C may serve as a biomarker for dementia, especially in conjunction with liver enzymes, given their shared roles in lipid metabolism and inflammation.
We hypothesized that transaminase-to-HDL-C ratios, such as ALT/HDL-C and AST/HDL-C, are associated with dementia and hence potential valuable tools in the prediction, diagnosis, monitoring, and early detection of dementia and cognitive decline in Southwestern Uganda, where the burden of dementia is increasing but diagnostic and predictive tools remain limited. To the best of our knowledge, no study in Uganda has assessed the relationship between transaminase-to-HDL-C ratios and dementia. Therefore, the main purpose of our study was to assess the association between serum transaminase-to-HDL-C ratios and probable dementia among PLWH on ART.
Materials and methods
Study design, population, and variables
We conducted a secondary data analysis using a dataset generated from a cross-sectional study 44 conducted among 377 PLWH on DTG-based ART. The current study was conducted from December 10, 2024 to January 30, 2025. In the primary study, 44 patients aged 18 years and above who had been on DTG-based ART for at least 12 months and had provided informed consent were enrolled. Individuals with missing clinical records, pregnant women, those on interrupted treatment, and those who visited due to an acute illness including hepatitis were excluded. Those who were on diabetes treatment, lipid-lowering medication, corticosteroids, or oral contraceptive pills were also excluded from the study. 44
Several variables including probable dementia and biochemical parameters were collected in the primary study. 44 In the secondary analysis, probable dementia was selected as the primary dependent variable. Dementia was screened in the primary study 44 using the Brief Community Screening Instrument for Dementia (CSID), which is suitable for use by non-specialists in low-resource settings. 45 The screening interview has two sections, with one interview for the person suspected of having dementia, which is used to determine the CSID cognitive score (seven items; range 0–9, higher score being better); and a separate informant section for a caregiver or close relative, which is used to determine the CSID informant score (six items; range 0–6, higher score being worse). Probable dementia was defined as A CSID cognitive score ⩽4.44,45
The major independent variables in the secondary analysis were calculated: AST/HDL-C ratio and ALT/HDL-C ratio. Other independent variables considered in the secondary analysis include anthropometric and biochemical parameters (waist circumference (WC), body mass index (BMI) GGT/HDL-C ratio, GGT/ALT ratio, alkaline phosphatase (ALP)/HDL-C ratio, ALP/ALT ratio, total cholesterol (TC)/HDL-C ratio, triglyceride (TG)/HDL-C ratio, fasting plasma glucose (FBG), FBG/HDL-C ratio, triglyceride–glycemic index (TyG), TyG–BMI index, fatty liver index (FLI), sodium/potassium ratio, blood pressure, electrolyte imbalance, and dyslipidemia. The demographic variables that were considered include age, sex, marital status, education level, residence, employment status, religion, smoking status, and alcohol consumption status.
Operational definitions and parameter calculation
Dyslipidemia: Derangement in at least one of the four lipid parameters (low-density lipoprotein-cholesterol ⩾130 mg/dL, TC ⩾200 mg/dL, TG ⩾150 mg/dL, and HDL-C <40 mg/dL for male, <50 mg/dL for female). 46
Electrolyte imbalance: Derangement in at least one of the serum electrolytes sodium, potassium, or chloride. The normal ranges for serum electrolytes were sodium (135–145 mmol/L), potassium (3.5–4.5 mmol/L), and chloride (96–106 mmol/L). 44
Blood pressure: Considered high if systolic blood pressure ⩾140 mmHg and/or diastolic blood pressure ⩾90 mmHg. 47
BMI: Calculated as weight in kilograms divided by the square of height in meters and classified <25, 25–29.9, and ⩾30 kg/m2. 48
TyG: Surrogate marker of insulin resistance calculated using the formula: TyG = Ln (TG (mg/dL) × FPG (mg/dL)/2) 49 and TyG–BMI index = TyG × BMI. 50
FLI: An algorithm based on BMI, WC, TGs, and GGT is a simple and accurate predictor of fatty liver. 51 It was calculated as

Sample size and data collection
For the secondary analysis, a sample size calculation was based on the prevalence of probable HIV-associated dementia (64.4%) reported in a cross-sectional study in a similar population in Uganda 52 using the Kish–Leslie formula (1965) with a 5% margin of error and a 95% confidence interval (CI) n = 1.962 × 0.644 (1 − 0.644)/0.052 = 352. Since the primary study 44 enrolled 377 participants, this sample size was adequate for the secondary data analysis.
Socio-demographic, clinical, and behavioral data were collected using a semi-structured questionnaire incorporating standardized tools. 44 Anthropometric measurements were obtained using calibrated equipment. 44 Medical records were reviewed to extract information on the duration of HIV infection, recent viral load, duration on ART and DTG-based ART, history of diabetes mellitus diagnosis, prescribed medications, and ART adherence. 44 Biochemical analyses were conducted using the HumaStar 100 clinical chemistry analyzer (Human Diagnostics, Germany). 44
Statistical analysis
Data was analyzed using STATA Statistical Software (release 17; StataCorp LLC, College Station, TX, USA). Continuous variables were tested for normality using the Shapiro–Wilk normality test. We used median (interquartile range (IQR)) to summarize the continuous variables as they were not normally distributed across the study participants. The distribution of the continuous biochemical parameters between participants with and those without probable dementia was compared using the Mann–Whitney-U test. A p < 0.05 was taken to be statistically significant. Categorical variables were summarized using frequencies and proportions.
A logistic regression model was used to assess association between serum transaminases/HDL-C ratios and probable dementia. All independent variables including the primary exposure variables at bivariate level were compared with binary probable dementia. The associations were measured using odds ratios (ORs) together with their 95% CIs, and the statistically significant ORs were indicated by a p < 0.05 at the bivariate level. The variables that were clinically and/or statistically significant at this level were assessed in the multivariable model to adjust for confounding effects. The multivariate model was adjusted for precision by removing some variables that were not statistically significant and those that were collinear in the full model. Hosmer–Lemeshow test was used to test the suitability of the final multivariate model in predicting probable dementia. A p value of 0.6873 was obtained indicating good goodness of fit for the final selected model. In the final multivariable model, associations were considered significant at a p < 0.05.
Results
Socio-demographic characteristics of study participants
Data from a total of 377 participants living with HIV on DTG-based ART was analyzed (Table 1). The median age was 44 years (IQR: 30–59), with 56.2% being female. Most participants were married or cohabiting (57.3%) and had attained tertiary education (40.1%). Urban residents constituted 57.3% of the sample. Regarding religion, Protestants were the majority (36.6%), followed by Catholics (29.7%). Employment was high, with 84.1% engaged in work, while 15.9% were unemployed.
Socio-demographic characteristics of the study participants.

Note. This table presents the socio-demographic characteristics of the study participants, including age, sex, marital status, education level, residence, religion, and employment status. Data are expressed as median (IQR) for continuous variables and as frequencies (%) for categorical variables.
IQR: interquartile range; N: number of participants.
Distribution of biochemical parameters and their ratios between participants with and without probable dementia
The median TC/HDL-C levels were significantly higher in participants with probable dementia compared to those without (3.86 versus 3.22, p = 0.03). AST/HDL-C and ALT/HDL-C levels were also higher among participants with probable dementia compared to those without although the differences did not reach statistical significance (Table 2).
Biochemical parameter ratios stratified by probable dementia stratus.
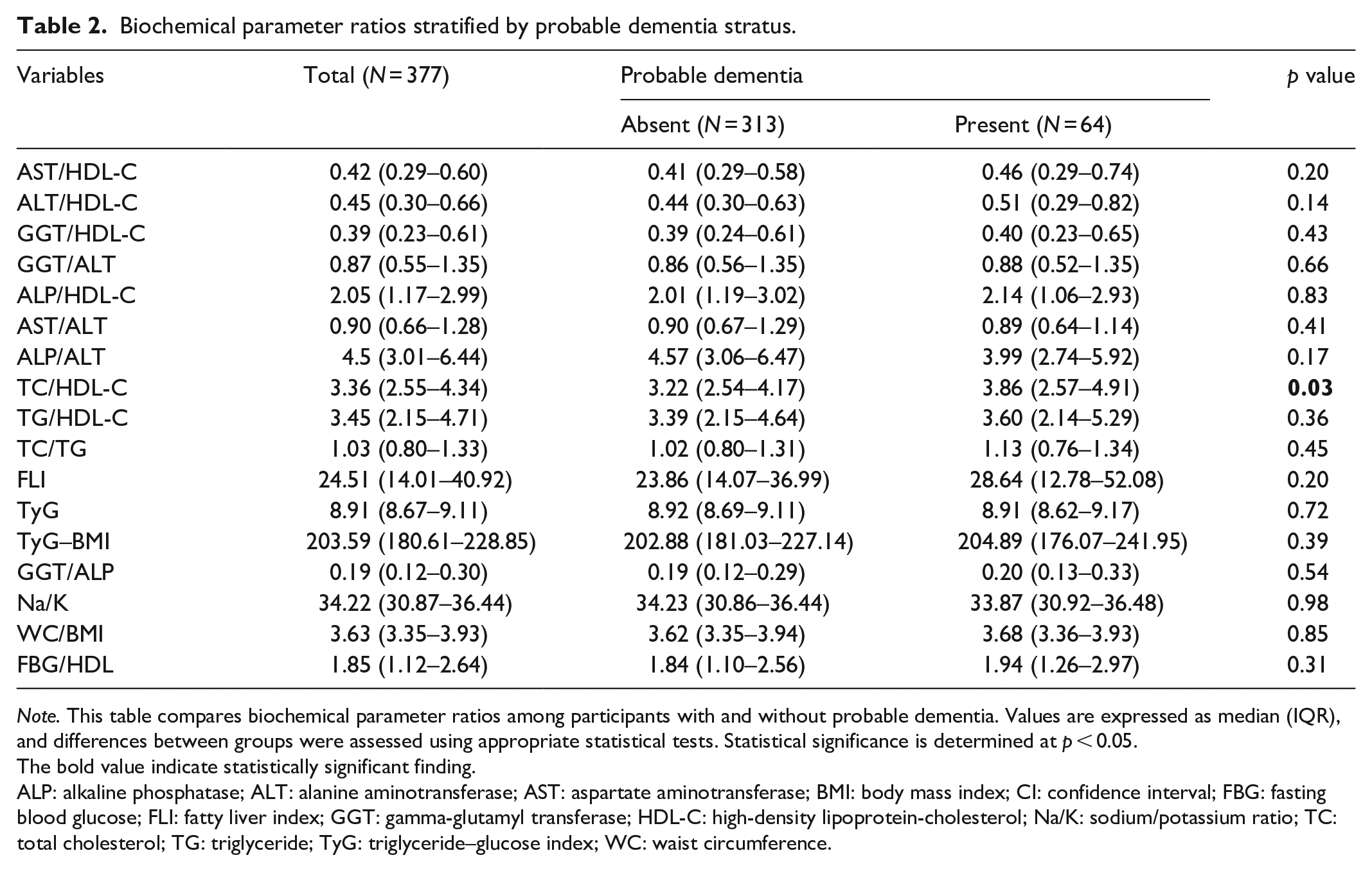
Note. This table compares biochemical parameter ratios among participants with and without probable dementia. Values are expressed as median (IQR), and differences between groups were assessed using appropriate statistical tests. Statistical significance is determined at p < 0.05.
The bold value indicate statistically significant finding.
ALP: alkaline phosphatase; ALT: alanine aminotransferase; AST: aspartate aminotransferase; BMI: body mass index; CI: confidence interval; FBG: fasting blood glucose; FLI: fatty liver index; GGT: gamma-glutamyl transferase; HDL-C: high-density lipoprotein-cholesterol; Na/K: sodium/potassium ratio; TC: total cholesterol; TG: triglyceride; TyG: triglyceride–glucose index; WC: waist circumference.
Association between serum AST/HDL-C ratio and probable dementia
In the adjusted analysis, compared to participants in the first tertile of AST/HDL-C ratio, the odds of probable dementia were higher in the second tertile (adjusted OR (aOR): 1.71; 95% CI: 0.62–4.74; p = 0.301) and significantly elevated in the third tertile (aOR: 4.47; 95% CI: 1.15–17.44; p = 0.031; Table 3). Age was independently associated with probable dementia, with each additional year increasing the odds by 11% (aOR: 1.11; 95% CI: 1.08–1.15; p < 0.001). At bivariate analysis, TG/HDL-C; crude OR (cOR): 1.14 (95% CI: 1.01–1.29; p = 0.036), TC/HDL-C; cOR: 1.21 (95% CI: 1.04–1.41; p = 0.013), FLI; cOR: 1.01 (95% CI: 1.00–1.02; p = 0.049), TyG–BMI index; cOR: 1.004 (95% CI: 1.0004–1.009; p = 0.038) were also significant predictors of probable dementia (Table 3).
Association between serum AST-to-HDL-C ratios with probable dementia.

Note. This table explores the association between serum AST/HDL-C ratio and probable dementia using bivariate and multivariate analyses. Results are presented as cORs and aOR with 95% CIs. Key variables include biochemical markers, age, sex, lifestyle factors, metabolic indicators, and blood pressure. Statistical significance is determined at p < 0.05.
The bold value indicate statistically significant finding.
ALP: alkaline phosphatase; ALT: alanine aminotransferase; AST: aspartate aminotransferase; aOR: adjusted odds ratio; BMI: body mass index; CI: confidence interval; cOR: crude odds ratio; DBP: diastolic blood pressure; FBG: fasting blood glucose; FLI: fatty liver index; GGT: gamma-glutamyl transferase; HDL-C: high-density lipoprotein-cholesterol; Na/K: sodium/potassium ratio; SBP: systolic blood pressure; TC: total cholesterol; TG: triglyceride; TyG: triglyceride–glucose index; WC: waist circumference.
The analysis of the association between BMI and probable dementia shows no statistically significant relationship in either bivariate or multivariate models. In the unadjusted analysis, overweight individuals (BMI 25–29.9 kg/m2) had an OR of 1.22 (95% CI: 0.65–2.31; p = 0.538), and obese individuals (BMI ⩾30 kg/m²) had an OR of 2.10 (95% CI: 0.87–5.06; p = 0.100), suggesting a possible trend toward increased dementia risk. However, after adjusting for potential confounders, the aORs decreased to 0.96 (95% CI: 0.35–2.60; p = 0.936) for the overweight group and 0.48 (95% CI: 0.06–4.23; p = 0.511) for the obese group, indicating no significant association (Table 3).
Discussion
Our study highlights a significant association between higher AST/HDL-C ratios and probable dementia among PLWH on DTG-based ART. Specifically, participants in the third tertile of AST/HDL-C ratio had a 4.47-fold increased likelihood of probable dementia compared to those in the first tertile, suggesting that elevated AST/HDL-C ratios may serve as a potential biomarker for cognitive decline. Clinically, these findings emphasize the importance of routine evaluation of liver function and lipid profiles in PLWH to enable early identification of at-risk individuals and timely interventions to reduce cognitive impairment. Given the higher prevalence of MetS, liver dysfunction, and dyslipidemia in PLWH,21,53–55 the observed findings emphasize the importance of integrated care approaches that address both metabolic and neurological health in this population. Our study findings are consistent with related studies that associated elevated AST levels and low HDL-C levels38,40,43 to increased risk of cognitive impairment and dementia.
The biological plausibility of these findings lies in the relationship between metabolic dysfunction and neurodegeneration.56,57 Elevated AST levels may indicate liver hypofunction or systemic inflammation, which are known contributors to cognitive decline.30,35 About 80% of AST is present in the mitochondria of hepatocytes, while ALT is mainly present in the non-mitochondria of hepatocytes and other body tissues. When liver cells are damaged, AST and ALT are released into the serum, resulting in elevated serum AST and ALT levels. 58 On the other hand, as liver function declines, so does the AST clearance rate. 59 Therefore, serum AST level becomes significantly higher than serum ALT level. Low HDL-C levels have been implicated in reduced clearance of amyloid-beta, impaired neurovascular health, and oxidative stress—pathways that are central to dementia development.38,40 Thus, the AST/HDL-C ratio reflects an interplay of hepatic and lipid-related mechanisms underlying cognitive decline.
Age was another key predictor of probable dementia, with each additional year increasing the odds by 11%.60,61 This study also revealed significant associations between metabolic markers (TC/HDL-C ratio, TG/HDL-C ratio, TyG/BMI ratio, and FLI) and dementia risk among PLWH on DTG-based ART. Biologically, these markers reflect dyslipidemia, MetS, insulin resistance, and hepatic steatosis62–65—conditions linked to neurodegeneration through mechanisms such as oxidative stress, systemic inflammation, and cerebrovascular dysfunction.38,66–68 Elevated TC/HDL-C and TG/HDL-C ratios indicate lipid imbalance, which impairs neurovascular integrity, while the TyG–BMI index and FLI highlight metabolic and hepatic dysfunction that exacerbate cognitive decline.
Globally, studies have identified dyslipidemia and liver dysfunction as independent predictors of cognitive decline,28,29,40,56 aligning with our findings. Research in Sub-Saharan Africa has highlighted cognitive impairment among PLWH,11,69 but studies on the AST/HDL-C ratio and other biochemical parameter ratios are limited. Variations in study design, population characteristics, and baseline risks explain discrepancies in findings, emphasizing the need for context-specific research to validate these markers and integrate them into clinical practice.
The findings from the study suggest that BMI is not independently associated with probable dementia. While the unadjusted analysis indicated a possible increased risk of dementia among individuals with obesity (OR: 2.10), this association did not reach statistical significance (p = 0.100). Furthermore, when potential confounding factors were taken into account in the multivariate model, the aORs for both overweight and obese individuals dropped significantly (aOR: 0.96 and 0.48, respectively), and the associations remained statistically non-significant (p values 0.936 and 0.511, respectively). These results highlight a few important considerations. While obesity has been linked to cognitive decline in previous research, 70 this study does not support a direct and independent link between elevated BMI and dementia risk. The notable attenuation of the association after adjustment for confounding variables suggests that other factors possibly age, glucose metabolism, lipid profiles, or liver function markers may play a more central role in dementia risk than BMI itself.
A major strength of this study lies in the fact that this study was adequately powered during sample size calculation. Also, we generated associations while putting other possible confounders into consideration. However, the study has some limitations that should be considered when interpreting the findings. First, as a secondary analysis of a cross-sectional study dataset, it provides only a snapshot of the associations between AST/HDL-C ratio and probable dementia, limiting our ability to establish causality or the temporal sequence of these associations. Additionally, the generalizability of our findings is limited to PLWH on DTG-based ART in Uganda, and may not apply to other populations or ART regimens.
Conclusion
The findings of this study reveal a significant association between high AST/HDL-C ratio and probable dementia among PLWH on DTG-based ART. Specifically, participants in the highest tertile of AST/HDL-C ratio had significantly increased odds of probable dementia compared to those in the lowest tertile, even after adjusting for potential confounders. These results suggest that a high AST/HDL-C ratio is potentially associated with cognitive decline in this population.
Recommendations
We recommend conducting longitudinal studies to establish causal relationships between AST/HDL-C ratios and dementia in PLHIV on DTG-based ART. Future research should also explore the association between various lipoprotein ratios and cognitive decline. Additionally, we recommend that future studies incorporate genetic factors, such as Apolipoprotein E ε4 genotype for a better understanding of the association of serum transaminase-to-HDL-C ratios with cognitive decline in this population. Additionally, implementing routine lipid and liver enzyme monitoring in clinical settings could facilitate early detection and intervention for cognitive decline, enhancing patient care in Uganda.
Footnotes
Acknowledgements
We express our deepest gratitude to the principal investigator for permitting a secondary data analysis on their study.
Ethical considerations
Ethical clearance for the primary study was obtained from the Research Ethics Committee (REC) of Mbarara University of Science and Technology (REC number; MUST-2024-1575). In the primary study, participants were explicitly asked consent for use of the data for secondary analysis for which they approved.
Consent to participate
In the primary study, all participants provided informed written consent prior to enrollment. The consent forms were translated into the local language (Runyankore) to ensure comprehension. Formally educated participants gave consent by signing the written forms. For participants with no formal education, the written informed consent form was read aloud in Runyankore, followed by administration of the comprehension screening tool approved by MUST Research Ethics Committee. Only participants who demonstrated understanding were allowed to consent by placing a thumbprint on the informed consent form.
Consent for publication
All authors have consented to the publication of this work.
Author contributions
All authors played a significant role in this study, including contributions to methodology, writing the original draft, and review and editing of the final draft of the article. They also participated in investigation, formal analysis, and interpretation of the findings.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The analyzed datasets are available from the corresponding author upon reasonable request.