
Abstract
Background:
Atherosclerosis (AS) is an important risk factor for macrovascular complications in diabetes mellitus and also serves as an independent risk factor for adverse cardiovascular and cerebrovascular events.
Objectives:
This study aims to investigate the association between serum meteorin-like protein (Metrnl) levels and carotid artery plaques in patients with type 2 diabetes mellitus (T2DM).
Design:
This study is a cross-sectional study that recruited patients with type 2 diabetes from our hospital’s endocrinology department and healthy subjects from the physical examination center. Carotid ultrasound and glucose tolerance test were performed, and subjects were grouped and analyzed based on the results of the carotid ultrasound and glucose tolerance test.
Methods:
A total of 208 participants were enrolled in this study. Serum Metrnl concentrations were measured using an enzyme-linked immunosorbent assay. The predictive value of Metrnl for carotid plaque development in T2DM patients was evaluated using receiver operating characteristic (ROC) curve analysis.
Results:
Serum Metrnl levels were elevated in the T2DM with carotid plaque group compared to those without (p < 0.05). Multivariate stepwise regression analysis revealed that Metrnl was an independent influencing factor for carotid intima-media thickness. Logistic regression analysis demonstrated that serum Metrnl remained independently associated with carotid plaque formation after adjusting for multiple confounders. ROC curve analysis indicated that the area under the curve for Metrnl in predicting carotid plaque in T2DM patients was 0.724 (95% confidence interval: 0.648–0.800), with a sensitivity of 71.3% and specificity of 67.9%.
Conclusion:
Elevated Metrnl levels are a risk factor for carotid plaque formation in T2DM patients, suggesting a potential role of Metrnl in the initiation and progression of carotid atherosclerosis in diabetic individuals.
Plain language summary
Serum Metrnl levels were significantly higher in T2DM patients with carotid plaques (P < 0.05). Metrnl, age, fasting glucose, and systolic blood pressure emerged as independent predictors of carotid intima-media thickness (CIMT). ROC analysis demonstrated Metrnl’s predictive value for plaque formation (AUC: 0.724, sensitivity: 71.3%, specificity: 67.9%).
Introduction
In recent years, the global incidence of diabetes has been steadily increasing due to population aging and lifestyle changes. Poor control of blood glucose, lipids, and blood pressure can lead to a series of diabetic complications.1,2 Cardiovascular complications have gradually become the leading cause of death among diabetic patients, accounting for more than half of the mortality rate in this population. 3 Atherosclerosis (AS) plays a critical role in the development of cardiovascular diseases and serves as the primary pathological basis for macrovascular complications in diabetes. 4 The thickening of carotid intima-media thickness (CIMT) often indicates the formation of carotid plaques, which reflect systemic AS and are closely associated with the occurrence of cardiovascular and cerebrovascular events.5,6 Therefore, identifying objective indicators for the early diagnosis of carotid atherosclerosis and implementing intervention measures are crucial for improving the prognosis of patients with type 2 diabetes mellitus (T2DM).
Meteorin-like protein (Metrnl) belongs to the family of neurotrophic regulatory factors, which includes meteorin. 7 Research has shown that Metrnl is the sole gene located at the terminal end of chromosome 17q, and notably, the 17q25.3 locus is a susceptibility region for cardiovascular diseases. 8 In 2014, Li et al. 9 identified Metrnl as a novel adipokine through gene array and bioinformatics analysis. In the same year, Rao et al. proposed that Metrnl is a circulating factor secreted after muscle exercise and cold stimulation of adipose tissue. Increased expression of Metrnl significantly stimulates eosinophil-dependent IL-4 expression and promotes the selective activation of adipose tissue macrophages, thereby enhancing thermogenesis in subcutaneous and visceral brown/beige fat and the expression of anti-inflammatory genes, stimulating energy expenditure, and improving glucose tolerance. 10 In a case-control study, Liu et al. found that serum Metrnl levels were significantly reduced in patients with metabolic-associated fatty liver disease (MAFLD). As serum Metrnl levels increased, the incidence of MAFLD showed a downward trend. 11 Currently, there is limited research on the relationship between serum Metrnl levels and carotid plaques in T2DM patients, both domestically and internationally. Therefore, this study aims to explore the relationship between serum Metrnl levels and carotid plaques in T2DM patients, with the goal of providing new clinical evidence for the prevention and early diagnosis of diabetic macrovascular complications.
Research design and methods
Study population
All participants in this cross-sectional study were recruited from the outpatient clinic, inpatient ward, or physical examination center of the Endocrinology Department at the Affiliated Hospital of Jiangsu University, Jiangsu Province, China, during the period from 2017 to 2022. A total of 208 adults were recruited for this study, including 40 healthy subjects and 168 subjects with T2DM. The definition of T2DM is based on the WHO diagnostic criteria (Fasting plasma glucose (FPG) ⩾126 mg/dL (7.0 mmol/L): A FPG level of 126 mg/dL or higher indicates diabetes. Fasting means that the individual has not consumed any food or beverages other than water for at least 8 h prior to the test. 2-H plasma glucose ⩾200 mg/dL (11.1 mmol/L) during an Oral Glucose Tolerance Test (OGTT): An OGTT involves drinking a glucose solution after fasting overnight, then testing blood glucose levels 2 h later. A result of 200 mg/dL or higher indicates diabetes.) 12 Exclusion criteria were as follows: (1) type 1 diabetes or special types of diabetes; (2) gestational diabetes; (3) acute complications of diabetes; (4) chronic complications of diabetes; (5) severe hepatic or renal insufficiency; (6) macrovascular diseases unrelated to diabetes; (7) malignancy, long-term bed rest, or recent history of traumatic surgery; (8) the person with missing data has been excluded.
The formula for calculating sample size used in this study is: n =
CIMT was measured by professional ultrasonographers using a color Doppler ultrasound diagnostic instrument (measuring the perpendicular distance between the intima and the interface between the media and adventitia of the vascular wall). Simultaneously, the presence of plaques in the carotid arteries of the patients was observed (in this study, a carotid plaque was defined as a local protrusion exceeding 0.5 mm into the arterial lumen, or exceeding 50% of the surrounding CIMT value, or a CIMT greater than 1.5 mm). Based on the results of carotid ultrasound measurements, T2DM patients were divided into 2 groups: 81 patients in the T2DM group without carotid plaques and 87 patients in the T2DM group with carotid plaques. This study was approved by the Biomedical Ethics Committee of our hospital.
Anthropometric and biochemical measurements
The personal information and usage details of hypoglycemic medications for all participants were collected through questionnaires administered by physicians in our department. Measurements of height, weight, waist circumference (WC), hip circumference (HC), and blood pressure were also taken. Body mass index (BMI) was calculated as weight (in kilograms) divided by the square of height (in meters); waist-to-hip ratio (WHR) was calculated as WC (in centimeters) divided by HC (in centimeters). An OGTT and an insulin release test were conducted. Fasting C-peptide (FC-P) was measured using radioimmunoassay; fasting insulin (FIns) was determined using chemiluminescence immunoassay; glycosylated hemoglobin A1c (HbA1c) was assayed using high-performance liquid chromatography; and FPG was measured using the glucose oxidase method. High-density lipoprotein cholesterol (HDL-C), triglycerides (TG), total cholesterol (TC), low-density lipoprotein cholesterol (LDL-C), and blood urea nitrogen (BUN) were assayed using enzymatic methods. Blood uric acid (UA) was measured using an automated biochemical analyzer.
The homeostasis model assessment of insulin resistance (HOMA-IR): HOMA-IR = FPG × FIns/22.5.
The homeostasis model assessment of β-cell function (HOMA-β): HOMA-β = FIns × 20/(FPG-3.5).
The TG-glucose product index (TyG): TyG = ln[TG (mg/dL) × FBG (mg/dL)/2].
Enzyme-linked immunosorbent assay (ELISA) was used to detect the level of Metrnl in serum samples. First, purified Metrnl antibodies were coated onto a 96-well microplate to form solid-phase antibodies. Then, standards, serum sample supernatants, biotinylated Metrnl antibodies, and horseradish peroxidase (HRP)-labeled avidin were added in sequence, followed by washing. After washing, the substrate tetramethyl benzidine (TMB) was added for color development. TMB was converted to a blue color by HRP and then turned yellow under acidic conditions. The intensity of the color was positively correlated with the concentration of Metrnl in the serum samples. The optical density was measured at a wavelength of 450 nm using a microplate reader, and the Metrnl concentration in the serum samples was calculated based on a standard curve. The Metrnl ELISA kit was purchased from Wuhan Huamei Bioengineering Co., Ltd (Cusabio; CSB-EL013718HU, Wuhan, China), with an inter-assay coefficient of variation (CV) ⩽10% and an intra-assay CV ⩽8%. The assay was conducted strictly in accordance with the kit’s instruction manual, including setting up the standard curve gradients, calculating the standard curve formula (Supplemental Figure 1), and subsequently determining the Metrnl levels based on the established standard curve.
Statistical analysis
Statistical analysis was performed using SPSS 26.0 software (Armonk, NY: IBM Corp.). Normally distributed data were described as mean ± standard deviation (x- ± SD), while non-normally distributed data were described as median and interquartile range (M (Q25, Q75)). For normally distributed continuous variables, independent sample t tests were used for comparisons between two groups, and one-way ANOVA was used for comparisons among multiple groups. For non-normally distributed data, non-parametric tests were used for comparisons between two groups, and the Kruskal–Wallis test was used for comparisons among multiple groups. Spearman’s correlation was used to investigate the relationship between serum Metrnl levels and biochemical and clinical indicators. All indicators of the study subjects were compared based on tertile grouping of serum Metrnl levels from low to high. With CIMT as the dependent variable, multiple stepwise regression analysis was used to explore the influencing factors of CIMT. Binary logistic regression analysis was used to explore the influencing factors of carotid plaque occurrence in T2DM patients. ROC curves were used to evaluate the predictive value of serum Metrnl levels for the occurrence of carotid plaques in T2DM patients. p-Value <0.05 (two-tailed) was considered statistically significant.
Results
Comparison of general clinical data and biochemical indicators among three groups
The T2DM group was further divided into the T2DM without carotid plaque group and the T2DM with carotid plaque group. Statistically significant differences were observed among the groups in terms of age, WC, WHR, systolic blood pressure (SBP), diastolic blood pressure, BUN, TG, TC, HDL-C, FPG, 2-hPG, HbA1c, FIns, 2-h postprandial C-peptide (2hC-P), HOMA-IR, HOMA-β, TyG, and Metrnl (p < 0.05). No statistically significant differences were found in gender, BMI, alanine aminotransferase (ALT), aspartate aminotransferase (AST), UA, LDL-C, 2hIns, and FC-P (p > 0.05). Specifically, compared to the T2DM without carotid plaque group, the T2DM with carotid plaque group showed significant increases in age, WC, SBP, TG, TC, urine albumin-to-creatinine ratio, and TyG, as well as a significant decrease in HDL-C, with statistical significance (p < 0.05; see Table 1). All study participants were divided into two groups based on gender: males (n = 112) and females (n = 96). The results showed that the serum Metrnl level was significantly higher in females compared to males (0.591 (0.285, 0.920) vs 0.319 (0.203, 0.656) ng/mL), with a statistically significant difference (p < 0.01; Supplemental Figure 2).
Comparison of general clinical data and biochemical indexes among the three groups.
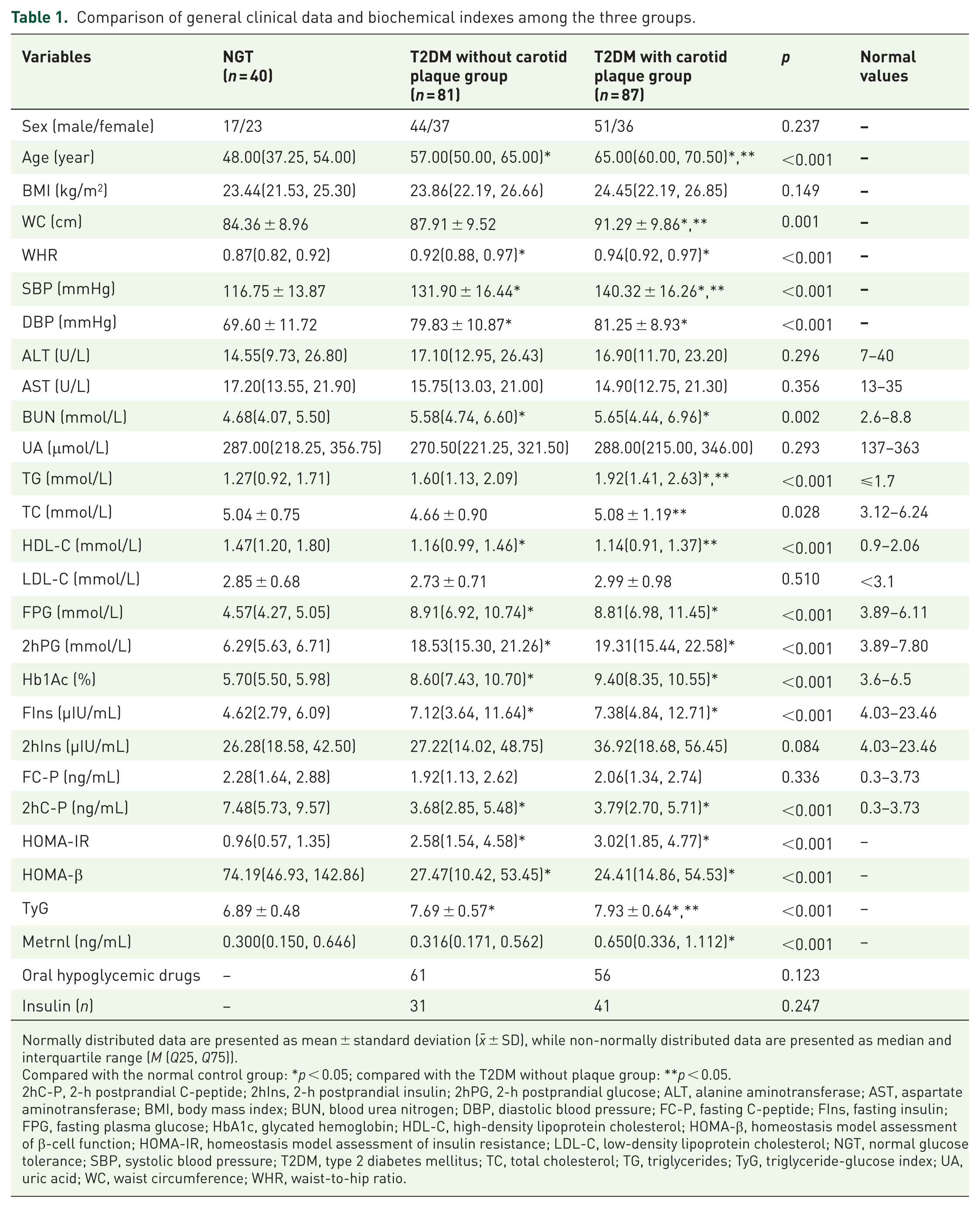
Normally distributed data are presented as mean ± standard deviation (x- ± SD), while non-normally distributed data are presented as median and interquartile range (M (Q25, Q75)).
Compared with the normal control group: *p < 0.05; compared with the T2DM without plaque group: **p < 0.05.
2hC-P, 2-h postprandial C-peptide; 2hIns, 2-h postprandial insulin; 2hPG, 2-h postprandial glucose; ALT, alanine aminotransferase; AST, aspartate aminotransferase; BMI, body mass index; BUN, blood urea nitrogen; DBP, diastolic blood pressure; FC-P, fasting C-peptide; FIns, fasting insulin; FPG, fasting plasma glucose; HbA1c, glycated hemoglobin; HDL-C, high-density lipoprotein cholesterol; HOMA-β, homeostasis model assessment of β-cell function; HOMA-IR, homeostasis model assessment of insulin resistance; LDL-C, low-density lipoprotein cholesterol; NGT, normal glucose tolerance; SBP, systolic blood pressure; T2DM, type 2 diabetes mellitus; TC, total cholesterol; TG, triglycerides; TyG, triglyceride-glucose index; UA, uric acid; WC, waist circumference; WHR, waist-to-hip ratio.
Comparison of clinical data and biochemical indicators among groups based on tertiles of serum Metrnl levels
After dividing all study participants into tertiles based on their serum Metrnl levels, the groups were designated as T1 (Metrnl <0.289 ng/mL, n = 70), T2 (0.289–0.650 ng/mL, n = 70), and T3 (Metrnl >0.650 ng/mL, n = 68) in ascending order. Statistically significant differences were observed among the three groups in terms of gender, age, TC, and CIMT (p < 0.05). Compared with the T1 group, the T2 group showed a significant increase in age, while the T3 group exhibited significant increases in age and CIMT (p < 0.05). Compared with the T2 group, the T3 group demonstrated significant increases in TC and CIMT (p < 0.05; Table 2).
Comparisons of clinical indicators of patients in each group according to serum Metrnl tertiles.

Compared with group T1: *p < 0.05, compared with group T2: **p < 0.05.
2hC-P, 2-h postprandial C-peptide; 2hIns, 2-h postprandial insulin; 2hPG, 2-h postprandial glucose; ALT, alanine aminotransferase; AST, aspartate aminotransferase; BMI, body mass index; BUN, blood urea nitrogen; CIMT, carotid intima-media thickness; DBP, diastolic blood pressure; FC-P, fasting C-peptide; FIns, fasting insulin; FPG, fasting plasma glucose; HbA1c, glycated hemoglobin; HDL-C, high-density lipoprotein cholesterol; HOMA-β, homeostasis model assessment of β-cell function; HOMA-IR, homeostasis model assessment of insulin resistance; LDL-C, low-density lipoprotein cholesterol; SBP, systolic blood pressure; T2DM, type 2 diabetes mellitus; TC, total cholesterol; TG, triglycerides; TyG, triglyceride-glucose index; UA, uric acid; WC, waist circumference; WHR, waist-to-hip ratio.
Correlation analysis between serum Metrnl levels and various indicators
A correlation analysis was conducted between Metrnl and various indicators. The results showed that, in all participants, serum Metrnl levels were positively correlated with age, SBP, TG, FPG, 2hPG, HbA1c, HOMA-IR, and TyG (r values were 0.408, 0.150, 0.149, 0.225, 0.137, 0.174, 0.188, 0.148, and 0.175, respectively, with p < 0.05). No significant correlations were found between Metrnl and clinical indicators in normal individuals. However, in patients with T2DM, Metrnl was positively correlated with age and CIMT (r values were 0.394 and 0.270, respectively, with p < 0.05; Table 3).
Correlation analysis between serum Metrnl levels and various indicators.

2hC-P, 2-h postprandial C-peptide; 2hIns, 2-h postprandial insulin; 2hPG, 2-h postprandial glucose; ALT, alanine aminotransferase; AST, aspartate aminotransferase; BMI, body mass index; BUN, blood urea nitrogen; CIMT, carotid intima-media thickness; DBP, diastolic blood pressure; FC-P, fasting C-peptide; FIns, fasting insulin; FPG, fasting plasma glucose; HbA1c, glycated hemoglobin; HDL-C, high-density lipoprotein cholesterol; HOMA-β, homeostasis model assessment of β-cell function; HOMA-IR, homeostasis model assessment of insulin resistance; LDL-C, low-density lipoprotein cholesterol; NGT, normal glucose tolerance; SBP, systolic blood pressure; T2DM, type 2 diabetes mellitus; TC, total cholesterol; TG, triglycerides; TyG, triglyceride-glucose index; UA, uric acid; UACR, urine albumin-to-creatinine ratio; WC, waist circumference; WHR, waist-to-hip ratio.
Multivariate stepwise regression analysis of factors influencing CIMT
With CIMT as the dependent variable and age, blood pressure, WHR, Metrnl, TG, FPG, and HOMA-IR as independent variables, a multivariate stepwise regression analysis was performed. The results indicated that Metrnl, age, FPG, and SBP were independent factors influencing CIMT (Table 4).
Multiple stepwise regression analysis of CIMT in T2DM.

CI, confidence interval; CIMT, carotid intima-media thickness; FPG, fasting plasma glucose; SBP, systolic blood pressure; SE, standard error; T2DM, type 2 diabetes mellitus; β, non-standardized coefficient; β′, standardized coefficient.
Binary logistic regression analysis of factors influencing carotid plaque formation
To further explore the correlation between serum Metrnl levels and carotid plaque, a binary logistic regression analysis was conducted with the presence of carotid plaque in patients with T2DM as the dependent variable. The results showed that, after adjusting for age, duration of diabetes, BMI, WC, SBP, TG, antidiabetic agents, and duration of diabetes, serum Metrnl levels remained associated with carotid plaque (Table 5).
Logistic regression analysis of factors associated with carotid plaque formation.

CI, confidence interval; Metrnl, meteorin-like protein; OR, odds ratio; SE, standard error; TG, triglycerides; β, partial regression coefficient.
Diagnostic value of serum Metrnl levels for carotid plaque in patients with T2DM
Receiver operating characteristic (ROC) curve analysis was performed. The results showed that the area under the ROC curve for serum Metrnl in predicting the occurrence of carotid plaque in T2DM patients was 0.724 (95% confidence interval: 0.648–0.800). With an optimal cutoff value of 0.392 ng/mL, the sensitivity, specificity, positive predictive value, negative predictive value, positive likelihood ratio, and negative likelihood ratio for predicting the occurrence of carotid plaque were 71.3%, 67.9%, 66.7%, 66.7%, 1.86, and 0.47, respectively (Figure 1).

ROC curve of Metrnl for predicting carotid plaque in T2DM patients.
Discussion
The findings of this study demonstrated that serum Metrnl levels were significantly elevated in patients with T2DM compared with those in the NGT. Notably, T2DM patients with carotid plaques exhibited higher serum Metrnl concentrations than those without carotid plaques. A positive correlation was observed between serum Metrnl levels and CIMT in T2DM patients. Furthermore, serum Metrnl levels were identified as an independent influencing factor for CIMT thickening in this population. Binary logistic regression analysis revealed that elevated serum Metrnl levels remained significantly associated with carotid plaque formation in T2DM patients after adjusting for potential confounders. ROC curve analysis demonstrated that serum Metrnl possesses satisfactory independent predictive value for carotid plaque development in T2DM patients. This is consistent with the recent research results that Metrnl has a good predictive value for carotid atherosclerosis assessed by CIMT (ROC curve shows that the area under the curve is 0.742, the sensitivity is 77.6%, and the specificity is 58.8%). 13 This study demonstrates superiority over Li et al.’s research in several aspects. First, while their study focused solely on diabetics, ours is more comprehensive, incorporating a healthy control group for comparison. Second, our study uses clear carotid artery plaque presence for grouping and includes CIMT analysis, whereas theirs is limited by using only CIMT as the grouping criterion. Finally, our study features a larger sample size and provides supplementary analysis on hypoglycemic drugs. These results collectively suggest that Metrnl may serve as a potential biomarker for early prediction and assessment of atherosclerotic plaque formation in this high-risk population.
Carotid plaque is a typical manifestation of atherosclerosis and is closely related to the occurrence of cardiovascular and cerebrovascular events.5,6 CIMT is a novel biomarker for early clinical AS and a predictor of impending cardiovascular events. An increase in CIMT often indicates the formation of carotid plaques. 14 Genome-wide association studies have identified Metrnl as a candidate gene related to CIMT in whole-blood gene expression. 15 The results of this study demonstrate a positive correlation between Metrnl and CIMT (r = 0.270, p < 0.001). Furthermore, when all study participants were divided into tertiles based on serum Metrnl levels, the CIMT in the T3 group was significantly higher than that in the T1 and T2 groups. Logistic regression analysis revealed that, after adjusting for age, diabetes duration, BMI, WC, SBP, and TG, serum Metrnl levels remained associated with carotid plaque formation (β = 0.792, p = 0.014), serving as an independent risk factor for carotid plaque formation in patients with T2DM. El-Ashmawy et al. 16 reported a negative correlation between serum Metrnl levels and atherosclerosis-related parameters, suggesting that Metrnl may be a potential surrogate marker for endothelial dysfunction and AS. Liu et al. found that decreased serum Metrnl concentrations were significantly associated with coronary heart disease (CHD), and regression analysis indicated an optimal cutoff value of 123.5 pg/mL for Metrnl in predicting CHD, with low sensitivity (44.04%) but high specificity (95.51%). In addition, they used the Gensini scoring system to assess disease severity based on luminal stenosis and lesion location, revealing a significant negative correlation between serum Metrnl levels and the number of diseased vessels and the Gensini score. 17 These findings suggest that serum Metrnl may play a crucial role in the onset and progression of AS.
Hyperglycemia can damage vascular endothelial cells, disrupt the normal function of the vascular wall, increase vascular permeability, and reduce nitric oxide production, thereby promoting the formation of AS plaques. 18 In clinical studies, there is no consensus on the changes in serum Metrnl levels in T2DM patients and the relationship between serum Metrnl and blood glucose. El-Ashmawy et al. 16 found that serum Metrnl levels in T2DM patients were significantly lower than those in subjects with normal glucose tolerance, and further analysis showed a negative correlation between serum Metrnl levels and FBP, 2hFBP, and HbA1c. Onalan et al. observed that serum Metrnl levels were significantly lower in newly diagnosed T2DM patients and long-term diagnosed T2DM patients compared to the control group. A negative correlation between serum Metrnl levels and FPG was observed in both newly diagnosed and long-term diagnosed T2DM patients, but no significant correlation was found in the normal control group. 19 In contrast, Wang et al. 20 reported that serum Metrnl levels were significantly higher in impaired glucose tolerance patients compared to those with normal glucose tolerance, and the highest levels were observed in T2DM patients, with a significant positive correlation between serum Metrnl levels and FBP, 2hFBP, and HbA1c. The results of this study are consistent with those of Wang et al., showing that serum Metrnl levels (447.39 (261.76, 846.69) pg/mL) in T2DM patients are significantly higher than those in the normal control group (300.59 (149.67, 645.59) pg/mL), and there is a significant positive correlation between serum Metrnl levels and FPG, 2hPG, and Hb1Ac. These differences in results may be attributed to various influencing factors in clinical investigations, such as the effects of medication, ethnic differences, and varying disease states. Tuncer Kara et al. recruited 30 healthy volunteers and 30 newly diagnosed T2DM patients, and administered metformin treatment to the newly diagnosed diabetic patients for 3 months. The study showed that plasma Metrnl levels were higher in the metformin-treated group than in the control group, while salivary Metrnl levels were lower. 21 Furthermore, physical exercise significantly increases Metrnl expression in human skeletal muscle. 22 Some studies have also indicated that serum Metrnl levels are higher during exercise in warm water compared to cold water. 23 Therefore, in addition to considering the treatment modalities received by patients, exercise and temperature are also factors influencing the relationship between serum Metrnl levels and T2DM, and large-scale, prospective, multicenter clinical studies are still needed in the future. Furthermore, physical exercise significantly increases Metrnl expression in human skeletal muscle.
Studies have shown that lipid metabolism disorders and insulin resistance play important roles in the onset and progression of AS. 24 Wang et al. 20 reported a positive correlation between serum Metrnl levels and TG, which is consistent with the findings of this study. In the study by Chung et al., 25 serum TG and TC levels were lower in T2DM patients than in the normal control group, and plasma Metrnl concentrations were negatively correlated with TG. The reasons for these differing results may be related to the use of lipid-lowering drugs by diabetic patients. This study showed that compared to the T2DM group without carotid plaques, the HOMA-IR values and TyG index in the T2DM group with carotid plaques exhibited an upward trend and were positively correlated with serum Metrnl levels. One study reported that serum Metrnl levels were significantly higher in the T2DM group compared to the normal glucose tolerance group. Furthermore, after adjusting for age, sex, BMI, SBP, TG, HDL-C, and diabetes duration in T2DM patients, a significant positive correlation was observed between serum Metrnl levels and HOMA-IR. 26 Consistent with the findings of the current study, Wang et al. 20 reported a positive correlation between serum Metrnl levels and HOMA-IR across their study population. However, conflicting results have emerged from other investigations. Onalan et al. 19 and Timurkaan et al. 27 demonstrated an inverse relationship between serum Metrnl levels and HOMA-IR in their respective studies. Notably, Loffler et al. observed significantly elevated Metrnl expression in adipocytes of obese children compared to controls, which positively correlated with FIns levels. Their experimental findings revealed that Metrnl overexpression suppressed adipocyte differentiation and PPARγ expression, potentially contributing to adipose tissue inflammation and hyperinsulinemia. 28 In contrast, Hu et al. 29 demonstrated in MIN6 mouse insulinoma cells that Metrnl ameliorated high glucose-induced impairment in insulin secretion while promoting β-cell proliferation and insulin production. These paradoxical findings may partially explain the observed positive association between serum Metrnl levels and HOMA-IR in certain populations. Although the precise relationship between Metrnl and insulin resistance remains controversial, accumulating evidence suggests that serum Metrnl likely participates in carotid plaque formation and progression through mechanisms potentially involving insulin resistance modulation.
Limitations
This study also has several limitations. First, due to the cross-sectional design employed, it is not possible to dynamically observe changes in serum Metrnl levels during the development and progression of carotid artery plaques in patients with T2DM. Second, serum Metrnl levels may exhibit individual variations and could be influenced by factors such as treatment modalities and disease duration. Future research should aim to design more rigorous experiments and consider other potential influencing factors to provide a more comprehensive understanding of the relationship between serum Metrnl and carotid artery plaques in T2DM patients. This knowledge could help establish Metrnl as a potential therapeutic target, offering more precise and effective strategies for the clinical management of macrovascular complications in T2DM patients.
Conclusion
In summary, elevated serum Metrnl levels in T2DM patients are a risk factor for carotid artery plaque formation, suggesting that Metrnl may be involved in the development of macrovascular complications in T2DM. High serum Metrnl levels might represent a defensive response to metabolic stress. However, the mechanisms by which Metrnl influences glucose and lipid metabolism and macrovascular complications in T2DM patients require further in-depth investigation.
Supplemental Material
sj-docx-1-tae-10.1177_20420188261419199 – Supplemental material for Clinical significance of meteorin-like protein in type 2 diabetes mellitus and its association with carotid plaque complications
Supplemental material, sj-docx-1-tae-10.1177_20420188261419199 for Clinical significance of meteorin-like protein in type 2 diabetes mellitus and its association with carotid plaque complications by Xia Deng, Zhongmin Yang, Yu Qin, Xunan Wu, Ziyan Sun, Ling Yang and Guoyue Yuan in Therapeutic Advances in Endocrinology and Metabolism
Supplemental Material
sj-tif-2-tae-10.1177_20420188261419199 – Supplemental material for Clinical significance of meteorin-like protein in type 2 diabetes mellitus and its association with carotid plaque complications
Supplemental material, sj-tif-2-tae-10.1177_20420188261419199 for Clinical significance of meteorin-like protein in type 2 diabetes mellitus and its association with carotid plaque complications by Xia Deng, Zhongmin Yang, Yu Qin, Xunan Wu, Ziyan Sun, Ling Yang and Guoyue Yuan in Therapeutic Advances in Endocrinology and Metabolism
Footnotes
Acknowledgements
We sincerely thank the volunteers of this study. We also wish to express our gratitude to all the authors who have made contributions to this study. X.D., Z.Y., and Y.Q. contributed equally to this work.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.