
Abstract
Background and aims:
During the COVID-19 pandemic confinement, virtual care strategies were implemented for individuals with type 2 diabetes (T2D). During the recovery process, hybrid care schemes (combining in-person and virtual care) continued, with limited information available on the results. This study aims to describe the metabolic parameters, lifestyle, self-care behaviors, and mental health of patients treated in the hybrid comprehensive care program.
Methods:
This is a descriptive and longitudinal observational study in patients with T2D who attended the hybrid comprehensive care program, comprising baseline (face-to-face), 3-month follow-up (face-to-face), 1-year follow-up (virtual), and 2-year follow-up (face-to-face). Metabolic and mental health variables were obtained (presence of anxiety, affective and eating disorders, quality of life questionnaires, Hospital Anxiety and Depression Scale for depression and anxiety, problem areas in diabetes, and empowerment) as well as self-care variables: calories consumed, exercise time, self-monitoring blood glucose, and foot checks.
Results:
Data from 104 patients were analyzed from October 2018 to November 2022, with a mean age of 55 (48–61) years, a female predominance of 49%, and a time since diagnosis of T2D of 2 (0–3) years. Metabolic parameters improved at 3 months, 1 year, and 2 years of follow-up. In self-care behaviors, the differences in minutes per week of exercise increased (baseline: 0 (0–180), 3 months: 175 (60–330), 1 year: 0 (0–150), and at 2 years: 90 (0–195); p < 0.0001). In self-care activities, we observed an increase in the proportion of patients who checked their feet and performed glucose self-monitoring (p < 0.001). A good quality of life, without distress and empowerment, has also improved.
Conclusion:
During a comprehensive care hybrid program, patients could maintain metabolic control goals, engage in self-care behaviors, mainly foot care and glucose self-monitoring, and improve their mental health parameters.
Plain language summary
This study aims to observe changes in the metabolic, self-care, and mental health characteristics of patients with type 2 diabetes mellitus who participated in a multidisciplinary hybrid diabetes education program. The first part of the program was in-person (the first 3 months), followed by virtual follow-up at 1 year due to the COVID-19 pandemic, and then returned to in-person care at 2 years of follow-up. Patients were observed to maintain their diabetes management goals under hybrid care.
Introduction
Type 2 diabetes mellitus (T2D) is a major global public health problem associated with disabling complications and macrovascular complications: coronary artery disease (CAD), cerebrovascular disease, and peripheral artery disease (PAD). Diabetes also affects vessels in the microcirculation, causing microvascular diseases such as nephropathy, retinopathy, neuropathy, and cardiomyopathy. Both macro and microvascular diseases are responsible for high morbidity and mortality in these patients.1–3 It affects people regardless of country, age, group, or sex. 4 The global prevalence of type 2 diabetes (T2D) in 2021 was 10.5%, rising to 12.2% by 2045 5 . The ENSANUT, Mexico’s national health and nutrition survey, shows an increase in the prevalence of diabetes over time: in 2006, it was 7%. In 2012, the rate was 9.2%; in 2016, it was 13.7% 6 ; in 2018, it was 16.8%; in 2020, it was 15.7% 7 ; and in 2022, it was 18.3%. 8 The International Diabetes Federation (IDF) reported that in 2021, Mexico was among the 10 countries with the highest prevalence of diabetes worldwide, ranking seventh. The four countries with the highest prevalence of diabetes were China, India, Pakistan, and the United States of America. 9
T2D is a condition predominantly managed by a person with diabetes, with the support and guidance of health care professionals. To make informed choices about diabetes self-management—including taking medications as prescribed, engaging in physical activity while reducing sedentary time, following an individualized exercise and diet plan, learning to measure blood glucose and interpret the results, and undergoing regular foot checks—people with diabetes need to receive structured education that outlines these key components to achieve optimal diabetes control and prevent complications. 10 For example, structured programs such as the Diabetes Self-Management Program incorporate these elements to empower patients with the practical skills needed for effective self-care. Self-management education and support (DSMES) are critical elements of care for all people with diabetes. 11 DSMES aims to equip people with diabetes with the knowledge, skills, and confidence to take responsibility for their self-management. This includes making informed decisions, solving problems, and developing personal goals and action plans to enhance health outcomes, the quality of care, and the overall quality of life for patients with diabetes. In the long term, these help reduce expenses and positively change lifestyle and self-care management. 12 Implementing lifestyle interventions in newly diagnosed patients with type 2 diabetes mellitus (T2D) improves cardiometabolic parameters, offering long-term benefits for health and well-being.
During the COVID-19 pandemic, confinement measures were implemented to prevent infections and reduce overall morbidity and mortality in the population.13,14 Notably, for patients with type 2 diabetes, these restrictions limited access to routine healthcare, disrupted established self-management practices, reduced opportunities for physical activity, and altered dietary behaviors—factors that together exacerbated challenges in maintaining glycaemic control and increased the risk of diabetes-related complications. 15 The adoption of telehealth requires changes in both patient-related and clinical care processes. Health professionals offer scheduled outpatient video visits integrated into the patient portal of the electronic health record, allowing patients to interact with their clinicians from personal computers or smartphones using platforms and telephonic communication. 16 Health professionals requested that patients take their vital signs or weight measurements at home using their own devices for clinical assessment. Health professionals requested that patients measure vital signs, including weight, at home using their devices for clinical assessment; however, patients often encountered challenges such as inaccurate readings due to non-calibrated equipment, unfamiliarity with proper measurement techniques, and technical difficulties that could compromise the reliability of the data. If they required cabinet studies, patients were asked to take the necessary measures (use of face masks) to the laboratories for blood sampling and to send their results by mail, in addition to evaluations being carried out using validated instruments, such as questionnaires. 17 Implementing virtual care models was a care strategy in patients with T2D, showing favorable results in self-care and metabolic control.14,18
We evaluate the long-term effectiveness of the hybrid care model in patients with T2D. The hybrid model refers to the consultation that combines in-person care and virtual care. In this case, the first phase of the program was conducted in person for the first 3 months, the 1-year follow-up was held virtually, and the 2-year follow-up was held in person. This study aimed to describe the metabolic parameters, lifestyle, self-care behaviors, and mental health of patients treated in a comprehensive care hybrid program.
Methods
Studying design
This is a retrospective study analyzing existing data from the CAIPaDi program. The age range of the patients with T2D was 18–70 years old, with a median of 54 ± 8.7 years. CAIPaDi is a multidisciplinary program with interventions designed to provide education and empowerment techniques (using simple, low-cost interactive tools). The program consists of two phases. The first phase consists of a basal visit and three monthly visits. The second phase consists of annual evaluations. On each visit, patients are examined by nine different healthcare professionals, including endocrinologists, diabetes educators, nutritionists, physical activity instructors, foot care experts, psychologists, liaison psychiatrists, ophthalmologists and optometrists, nurses, and dentists. These interventions were divided into medical, mental health, and self-care behaviors. 2
The objective of the CAIPaDi program is to provide patients with the necessary tools to be independent and make informed decisions about their long-term self-care. For this reason, they undergo an annual review of each intervention to adjust the treatment and reinforce diabetes education. The reasons for changing in-person visits to virtual evaluations were due to measures taken by health authorities in response to the COVID-19 pandemic. For this study, data were collected from patients who attended their first annual virtual consultation to investigate the long-term maintenance of metabolic control, self-care, and mental health goals when they returned for their in-person visit the following year.
Data collection and measurements
During each visit, laboratory studies (fasting glucose, glycated hemoglobin, lipid profile, creatinine, and liver function tests) were obtained at the CAIPaDi center as part of the face-to-face care. For virtual care, we asked participants to send recent laboratory studies by email. Patients forwarded via email the file with their study results, which was sent directly from the laboratory. Specific questionnaires were administered to all the participants to complete the evaluation. During the COVID-19 pandemic, the questionnaires were answered in digital form. The questionnaires above included the Mini-International Neuropsychiatric Interview (MINI), Diabetes Empowerment Scale-Short Form (DES-SF), Hospital Anxiety and Depression Scale (HADS), Diabetes Quality of Life (DQoL) Questionnaire, Problem Areas in Diabetes (PAID) Scale, International Activity Questionnaire (IPAQ) 19, and a 3-day food record to document the daily calorie intake.
Procedures
During the COVID-19 pandemic, consultations changed to a virtual modality. The virtual consultation was conducted through Google Meet or, if that was not possible, via a video call on WhatsApp. This study considered patients who received hybrid care, with follow-up conducted face-to-face at baseline and at 3 months and virtually at 1 year and 2 years. All visits were held from 2018 to 2022.
Participants
This study included adult patients with T2D diagnosed less than 10 years ago, nonsmokers without any disabling chronic complications, and who had hybrid attention in the CAIPaDi program.
Statistical analysis
The statistical analysis was performed using SPSS software, version 25 IMB USA. Only participants with complete data were included in the analysis. The data were recorded in the general database of the CAIPaDi program. For this analysis, only the variables of interest at the relevant time points (baseline, 3 months face-to-face, 1 year virtual, and 2 years face-to-face) were considered. Specifically, the identified outliers were reviewed directly in the clinical records, where they were found to be incorrect and subsequently corrected prior to the analysis. The identification of outliers was performed through exploratory data analysis, including distribution plots and summary statistics. Outliers were flagged when values fell outside physiologically plausible ranges or were inconsistent with the clinical context.
Each flagged data point was cross-checked against the original clinical records. When transcription or entry errors were confirmed, corrections were made accordingly. If no clear explanation or source documentation was available, the data point was treated as missing and excluded from the relevant analysis. These steps were taken prior to any statistical modeling to ensure the integrity and reproducibility of the results.
Variables are reported as medians and interquartile ranges (25–75) according to the normality of their distribution. Normality was evaluated with the Kolmogorov-Smirnov test. Statistical significance was determined using the Friedman test. Categorical variables were analyzed using frequencies and percentages. Statistical significance was determined using the Q Cochran test.
A post hoc analysis was performed using Bonferroni-adjusted pairwise comparisons, following the Friedman test for quantitative variables and Cochran’s Q test for qualitative variables, to identify the time point at which the most significant changes occurred.
Results
We evaluated 104 patients from October 2018 to November 2022, comprising 51 (49%) women, with a mean age of 54 ± 9 years, 2 (0–3) years of T2D diagnosis, and a BMI of 30.4 ± 6.3 kg/m2. Table 1 shows the changes in metabolic parameters.
Metabolic parameters.
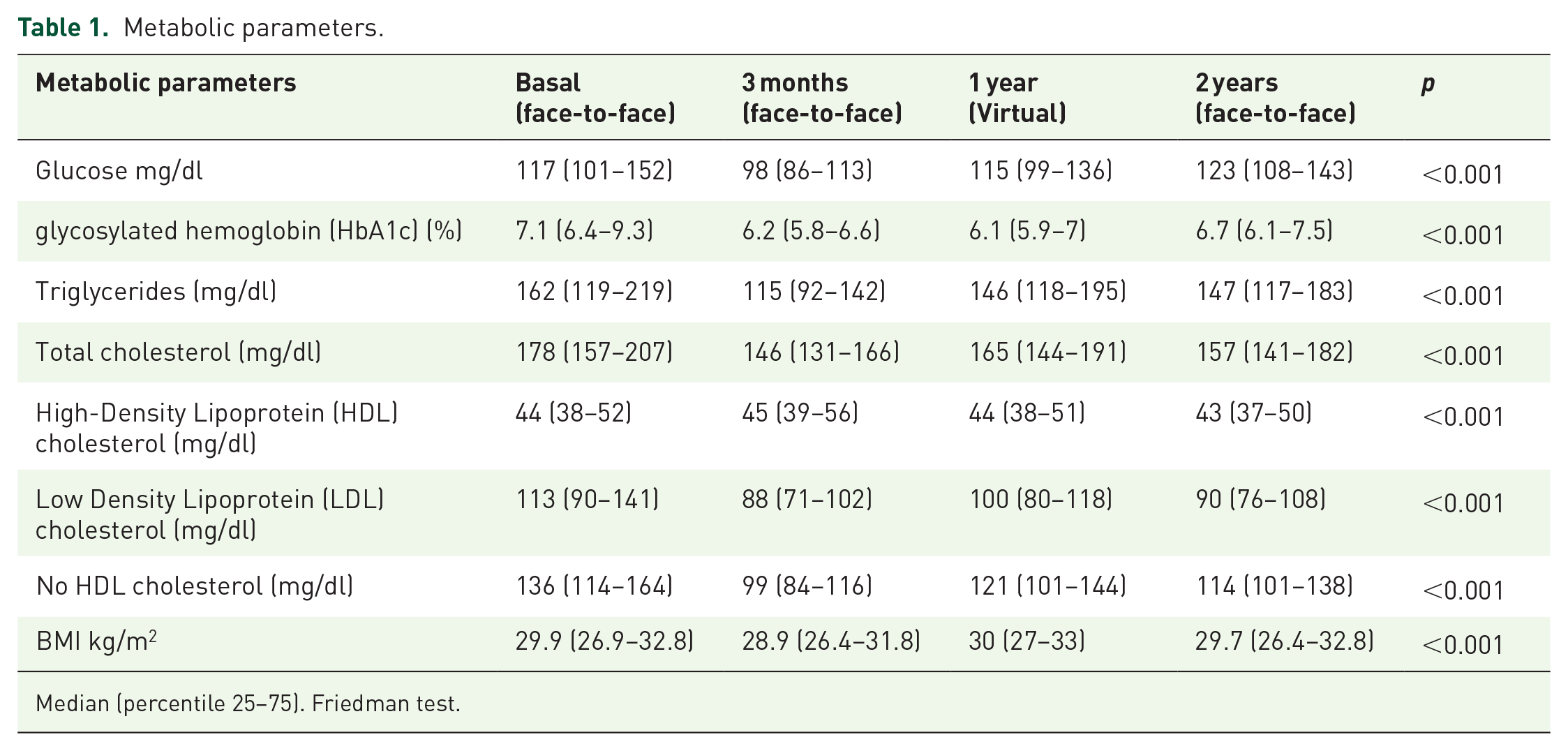
Median (percentile 25–75). Friedman test.
Table 2 shows the results of self-care activities. The percentage of patients who performed self-monitoring and foot examinations increased and was statistically different (p < 0.001).
Lifestyle and self-care variables.

Median (percentile 25–75). Friedman test. (%) Q Cochran test.
SMBG, self-monitoring blood glucose.
Regarding lifestyle changes, the calories consumed in the 3-day food record decreased over time compared to baseline (p < 0.02). The minutes of exercise reported in the IPAQ increased notably for the 3-month follow-up, 175 (60–300) min/week, and in the annual consultations, they decreased, with the difference being greater in the virtual visit at 1 year of follow-up, 0 (0–150) min/week.
In mental health variables, we observed that the percentages of people with severe anxiety and depression symptoms decreased between baseline, 23 (24.1%) and 9 (8.7%), and at 3 months of follow-up, 8 (7.7%) and 4 (3.8%), respectively (Table 3). In 1 year (virtual consultation), the percentages increased by 12 (11.5%) and 9 (8.7%). For the 2 years of follow-up (face-to-face). They decreased significantly by 10 (9.6%) (p < 0.001) and 2 (1.9%) (p < 0.001). There is an increase in the percentage of the presence of anxious syndrome, affective syndrome, and eating disorders for the annual consultation (virtual) compared with the 3-month follow-up. The affective syndrome maintained an increasing trend, while the other percentages decreased for the 2-year follow-up (face-to-face).
Mental health variables.

(%) Q Cochran test.
DQoL, Diabetes Quality of Life; HADS, Hospital Anxiety and Depression Scale; PAID, Problem Areas in Diabetes.The results of the post hoc analysis showed that for metabolic and exercise-related variables, the most significant changes occurred at the 3-month follow-up (in-person), compared to both the 1-year (virtual) and 2-year (in-person) follow-ups, with statistically significant differences (p < 0.001).
For self-care variables, significant changes were observed when comparing baseline values (in-person) with those at 3 months (in-person), 1 year (virtual), and 2 years (in-person), all with p < 0.001. Similar findings were observed for the PAID questionnaire and DQoL measures, which reflect mental health outcomes. Empowerment showed a statistically significant improvement only when comparing the baseline (in-person) with the 2-year follow-up (in-person) (p = 0.007).
Discussion
This article presents a long-term follow-up of individuals with diabetes who were initially cared for in the CAIPaDi program in person for the first 3 months and then transitioned to virtual care after 1 year of follow-up. The results have already been published, concluding that the virtual mode can be used to improve results, educate patients, and prevent acute or chronic complications in patients with type 2 diabetes, 19 so we wanted to observe metabolic, lifestyle, and mental health characteristics of these patients when they returned for their face-to-face annual evaluation.
A systematic review revealed that DSME effectively reduced HbA1c among T2DM patients. The mean difference in HbA1c was −0.604% (95% confidence interval (CI) = −0.854, −0.353, I2 = 90.3, p < 0.001). 20 The face-to-face CAIPaDi program reported that after 2 years, 61% of patients maintained glycated hemoglobin levels below 7%. 21 In this study, patients showed a decrease of 1% at 1 year (virtual) and 0.4% at 2 years (face-to-face) in HbA1c. A non-randomized controlled trial of a continuous type 2 diabetes intervention program via telemedicine demonstrated that the lipid profile improved at 1 year. 22 In this study, we observed the maintenance of the lipid profile under control at 2 years of follow-up.
There is little evidence of hybrid care for patients with type 2 diabetes. Tourkmani demonstrated the effectiveness of a hybrid care program (virtual and face-to-face) for patients with uncontrolled diabetes, the average time of diabetes diagnosis was 13.8 ± 8.5 years in which the hybrid model significantly reduced HbA1c from 10.47 ± 1.23% to 7.87 ± 1.59% (mean difference of reduction 2.59% (95% CI = 2.34–2.85), p < 0.001), for 4 months. 23 In this study, we take recent diabetes diagnosis patients. The follow-up was longer than the Turkmani study, and patients’ glucose levels improved over time. Both studies confirm the effectiveness of hybrid programs in reducing glucose levels.
For self-care variables, we observe a significant decrease in exercise time at the 1-year follow-up (virtual care) during the COVID-19 pandemic. It has been described as a substantial decrease in global physical activity levels during the period of social isolation adopted worldwide to contain the spread of the coronavirus disease 2019.24,25 For self-care variables, we observed a significant decrease in exercise time at 1 year of follow-up (virtual care) during the COVID-19 pandemic. The decrease in exercise during the virtual consultation can be attributed to the fact that patients were unable to exercise outdoors due to confinement. In Addition, the 6-min walk and strength tests could not be performed during the virtual consultation, and participants did not receive feedback regarding their physical condition. There is a level increase for the 2-year follow-up (face-to-face). During those years, 2021 and 2022, some activities began to be resumed, but many patients reported that they were afraid of going out and catching COVID-19. It also draws attention to the remarkable increase in SMBG patients taking care of their feet with an educational diabetes program.26,27
Our study shows a long-term improvement in mental health variables. This finding is consistent with the literature, which has highlighted the value of multidisciplinary interventions, with mental health specialists playing a crucial role in diabetes management, particularly during the COVID-19 pandemic.28,29
This study shows that the implementation of hybrid care programs can help improve the follow-up of patients with type 2 diabetes and reinforce diabetes education since, in this way, the patient can save time and money on travel to the care center without leaving aside the in-person evaluation that is more detailed and specific, in addition to the fact that they can have a more continuous follow-up, especially in those patients who have uncontrolled glucose as proposed by Tourkmani. 23
One of the strengths of this study is that it is the first to provide information on the outcomes of people treated in a long-term hybrid diabetes education program. In addition, the main factors that must be considered in treating T2D were investigated: metabolic control, lifestyle changes, and mental health.
Among the study’s limitations, we found that for the data from the virtual consultations, patients had to send their results from different laboratories, as they could not visit CAIPaDi to conduct their studies, unlike in face-to-face consultations, due to measures taken to reduce infections.
Our study’s findings open several avenues for future research, including the exploration of a hybrid multidisciplinary evaluation in diabetes management that combines in-person and telehealth components. Such studies could assess its impact on glycemic control, patient adherence to self-management strategies, and overall quality of care.
Conclusion
During the CAIPaDi hybrid program, patients were able to maintain metabolic control goals and self-care behaviors, primarily in foot care and SMBG, while also improving mental health parameters. In-person or virtual interventions have helped maintain control of goals. Regardless of the strategy used, patients can achieve their objectives.
Footnotes
Acknowledgements
Group of study CAIPaDi: Denise Arcila-Martínez, Rodrigo Arizmendi-Rodríguez, Humberto Del Valle-Ramírez, Arturo Flores García, Mariana Granados-Arcos, Héctor Infanzón-Talango, María Victoria Landa-Anell, Claudia Lechuga-Fonseca, Angélica Palacios-Vargas, Marco Antonio Melgarejo-Hernández, Liliana Pérez-Peralta, David Rivera de la Parra, Francis Rojas-Torres, Sandra Sainos-Muñoz, José Luis Cárdenas-Fragoso, Maureen Alexis Acosta-Mireles, Arely Hernández-Jasso, María Guadalupe Soto-Gutiérrez, Nubia Pamela López-Jiménez Andrea Villegas-Narváez, Adriana Siboney Araujo-González, Carlos A. Aguilar-Salinas, Francisco J Gómez-Pérez and José Sifuentes-Osornio.