
Abstract
Background:
Vitamin D (VD) deficiency has become a global public health problem, and published studies have demonstrated that patients with subacute thyroiditis (SAT) have worse VD nutritional status and that VD supplementation may alleviate thyroid-related diseases by fighting against infections and mediating autoimmunity.
Objectives:
This study explored the correlation between serum VD levels and the risk and extent of disease in patients with SAT.
Design:
A case-control study.
Methods:
We included patients with SAT diagnosed at the First People’s Hospital of Jining City between September 2021 and September 2023 and a healthy population during the same period. We collected clinical and laboratory data to determine differences in VD levels between the two populations and identify risk factors for the onset and extent of SAT.
Results:
The 25(OH)D level of SAT patients was significantly lower than that of the healthy population (p < 0.05). Multifactorial logistic regression analysis showed that low 25(OH)D level, low body mass index (BMI), elevated leukocytes, and low lymphocyte count were independent risk factors for SAT. No significant difference was noted in VD levels between patients with mild SAT and those with moderately severe SAT (p > 0.05). Additionally, fever, thyroid tenderness, high BMI, and elevated free thyroxine (FT4) were independent risk factors for SAT severity; serum 25(OH)D levels were positively correlated with FT4/FT3 levels in SAT patients.
Conclusion:
VD levels are lower in patients with SAT than in healthy controls, and low VD levels increase SAT risk. Although VD levels are not related to SAT severity, adequate VD inhibits the conversion of FT4 to FT3, likely playing a protective role in SAT development.
Plain language summary
Introduction
Subacute thyroiditis (SAT) is the most common painful thyroid disease characterized by the destruction of thyroid follicles; infiltration of inflammatory cells such as neutrophils, lymphocytes, multinucleated giant cells, eosinophils, and plasma cells; and formation of granuloma. The pathogenesis of SAT has not yet been elucidated and is currently being considered related to immunity and infections: genetically susceptible individuals with certain types of human leukocyte antigen (HLA) 1 are susceptible to SAT following infection with upper respiratory tract viruses (occurring approximately 2–6 weeks prior). 2
Vitamin D (VD) is an essential fat-soluble vitamin, and serum 25(OH)D level is the best indicator for evaluating VD nutritional status. The classical physiological role of VD is to maintain calcium-phosphorus homeostasis, and in recent years, the extra-skeletal effects of VD and its analogues have continued to be discovered, such as with diabetes mellitus, cardiovascular disease, neoplasms, immune disorders, and infectious diseases. 3 Active VD calcitriol not only maintains cellular tight junctions to reduce the risk of infection but also encodes proteins required for the formation of gap junctions, tight junctions, and adherens junctions, which protects the integrity of cellular junctions from viral interference. 4 Inadequate levels of VD have been found to reduce immunity and increase the frequency and severity of viral infections, 5 while adequate VD levels have been found to also significantly reduce the risk of respiratory infections. 6
In recent years, an increasing number of studies have been conducted on the relationship between VD and thyroid-related diseases. However, there are relatively few studies on the relationship between VD and SAT diseases, and the results are inconsistent, with two studies reporting that serum 25(OH)D levels of SAT patients were lower than those of healthy populations,7,8 and the other study concluding that there was no difference in VD levels in SAT compared with those of the healthy populations. 9 Therefore, this study aimed to further understand the VD nutritional status of SAT patients and preliminary investigate the correlation between VD levels and SAT to provide a basis for the relationship between VD and SAT disease.
Subjects and methods
Subjects
The case group comprised patients with newly confirmed SAT selected from the outpatient or inpatient department of the Division of Endocrinology and Metabolism of the First People’s Hospital of Jining City from September 2021 to September 2023. The inclusion criteria were as follows: compliance with the diagnostic criteria for SAT in the Chinese Diagnostic Guidelines for Thyroid Diseases—Thyroiditis 10 ; all patients were informed of the nature of the study, following which written informed consent was obtained. The exclusion criteria were as follows: recent use of drugs interfering with thyroid function and VD level; use of non-steroidal anti-inflammatory drugs (NSAIDs), glucocorticoids, and immunosuppressive drugs; pregnant and lactating women; combination of chronic hepatic and renal insufficiency; parathyroid disease; adrenal disease; anorexia nervosa; post-gastrectomy; and nutrient metabolism and absorption disorders. As for sample size calculation, the proportion of VD deficiency in our population is approximately 70%, consistent with that in literature, 11 calculated according to the following formula:

Test efficacy was considered as 0.9, with an odds ratio of 3.0; based on calculation using PASS 15 software, 66 people were included from at least 66 cases of SAT; finally, 141 patients with SAT met the criteria for nadir exclusion. The control group was selected from the general medical checkup population from the same health checkup center, with “age, gender, and quarter of medical checkup” as the matching items, with a matching tolerance of 0.01; based on calculation using SPSS 25.0 software, propensity score matching was performed to match the SAT group with the control group in a 1:1 ratio, and 141 pairs were successfully matched. Laboratory tests of all participants were subject to quality control at the Department of Laboratory Medicine, Jining No. 1 People’s Hospital.
Research methods
General medical information including sex, age, medical history, height (cm), weight (kg), and body mass index (BMI; weight in kg/height in m2) was collected. In SAT patients, the presence of fever, the maximum temperature during fever, enlargement of the thyroid gland, and tenderness of the thyroid gland were recorded. Additionally, complete blood count, erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), 25 (OH)D, free triiodothyronine (FT3), free thyroxine (FT4), thyroid-stimulating hormone (TSH), thyroperoxidase antibodies (TPOAb), 25(OH)D, thyroglobulin antibodies (TGAb), neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR), and free thyroxine/free triiodothyronine (FT4/FT3) data were recorded in SAT patients. The severity of SAT was scored as follows 12 : fever—none, <38°C, and >38°C (0, 1, and 2 points, respectively); tenderness—none, mild, and severe (0, 1, and 2 points, respectively); goiter palpation—none and yes (0 and 1 point, respectively); and ESR—normal, 21–50 mm/h, and >50 mm/h (0, 1, and 2 points, respectively). A score of <3 and ⩾3 was defined as mild SAT and moderately severe SAT, respectively. After the SAT diagnosis, according to the treatment guidelines of the Chinese and American Thyroid Association,10,13 patients with mild SAT were advised general treatment (adequate rest and plenty of drinking water) or oral NSAIDs, and glucocorticoid hormone treatment was provided for other bodily symptoms such as persistent high fever, thyroid pain, enlarged thyroid gland with marked tenderness, or ineffective treatment with NSAIDs.
Statistical analysis
EpiData 3.1 software was used to establish the database, and SPSS (version 26.0; IBM Corporation, Armonk, NY, USA) was used to organize and analyze the study data. Measurement data were expressed as mean ± standard deviation, and the t test was used for comparison between two groups of variables with a normal distribution. Non-normally distributed data were expressed as median M (P25, P75), and the rank-sum test was used for comparison between groups. Count data were expressed as numbers (percentages), and their distribution was compared using the Chi-square test. Spearman analysis and multiple linear regression were used to analyze associations, and multifactorial logistic regression was used to analyze influencing factors. Variance inflation factor >10 indicated severe multicollinearity, and p < 0.05 was considered to indicate statistically significant differences.
Results
Comparison of general information and blood indices between the SAT and control groups
The 25(OH)D level, lymphocyte count, and BMI in the SAT group were significantly lower than those in the healthy control group (p < 0.05), while the counts of leukocytes, neutrophils, monocytes, and platelets, and the NLR and PLR were significantly higher than those in the healthy control group (p < 0.001; Table 1).
Comparison of general information and serum indices between the SAT and control groups.

25(OH)D, 25-hydroxyvitamin D; BMI, body mass index; NLR, neutrophil-to-lymphocyte ratio; ns, not statistically significant; PLR, platelet-to-lymphocyte ratio; SAT, subacute thyroiditis.
Risk factor analysis for the occurrence of SAT
The indicators that were significant differences between groups were selected, and after covariate analysis, neutrophils, monocytes, NLR, and PLR with covariates were removed, and multifactorial logistic regression was performed with five factors, namely BMI, leukocytes, lymphocytes, platelets, and 25(OH)D, as independent variables and the occurrence or non-occurrence of SAT as the dependent variable. The results showed that low 25(OH)D (p < 0.05), low BMI (p < 0.05), elevated leukocytes (p < 0.001), and decreased lymphocytes (p < 0.05) were independent risk factors for the development of SAT (Table 2).
Logistic regression analysis of risk factors for SAT development.

25(OH)D, 25-hydroxyvitamin D; BMI, body mass index; CI, confidence interval; OR, odds ratio; SAT, subacute thyroiditis.
Comparison of general information and blood indices between mild SAT and moderately severe SAT
Of the 141 SAT patients included, 43 had mild SAT and 98 had moderate-to-severe SAT. The average age of the mild SAT group was 48.51 ± 17.37 years, and 72.09% were female, and the average age of the moderate-to-severe SAT group was 47.91 ± 10.53 years, and 67.35% were female. There was no statistically significant difference between mild and moderate-to-severe SAT cases in terms of age and sex (p > 0.05). The proportions of patients with fever, goiter, and thyroid tenderness, as well as BMI, leukocytes, neutrophils, platelets, NLR, PLR, ESR, CRP, and FT4, in the moderate-to-severe SAT group were significantly higher than those in the mild SAT group (p < 0.05); TSH was significantly lower than that in the mild SAT group (p < 0.001); and 25(OH)D levels, lymphocytes, monocytes, FT3, TPOAb, and TGAb levels were not statistically significant (p > 0.05) in both groups (Table 3).
Comparison of general data and serum indices in patients with different severities of SAT.

25(OH)D, 25-hydroxyvitamin D; BMI, body mass index; CRP, C-reactive protein; ESR, erythrocyte sedimentation rate; FT3, free triiodothyronine; FT4, free thyroxine; NLR, neutrophil-to-lymphocyte ratio; ns, not statistically significant; PLR, platelet-to-lymphocyte ratio; SAT, subacute thyroiditis; TGAb, thyroglobulin antibodies; TPOAb, thyroperoxidase antibody; TSH, thyroid-stimulating hormone.
Risk factors for the severity of SAT
The indicators with significant differences among SAT patients with different severities of disease were selected, and after removing leukocytes, NLR, PLR, CRP, and TSH, which were covariate diagnostics, the remaining nine factors, namely goiter, fever, thyroid tenderness, BMI, neutrophils, platelets, ESR, FT4, and 25(OH)D, were considered as independent variables the severity of SAT as the dependent variable. The results showed that VD was not a risk factor for the severity of SAT, and fever, thyroid tenderness, elevated BMI, and elevated FT4 were independent risk factors for the severity of SAT (p < 0.05; Table 4).
Logistic regression analysis of risk factors for the severity of SAT.

25(OH)D, 25-hydroxyvitamin D; BMI, body mass index; CI, confidence interval; ESR, erythrocyte sedimentation rate; FT4, free thyroxine; OR, odds ratio; SAT, subacute thyroiditis.
Correlation analysis of 25(OH)D with inflammatory parameters and thyroid function
Spearman’s correlation analysis suggested that 25(OH)D levels did not correlate with leukocytes, neutrophils, lymphocytes, monocytes, ESR, CRP, NLR, PLR, FT3, FT4, TSH, TPOAb, and TGAb (p > 0.05) but showed a significant positive correlation (r = 0.168, p < 0.05) with FT4/FT3 (Table 5 and Figure 1). Scatter plots were generated with 25(OH)D as the independent variable and inflammatory parameters and thyroid function as the dependent variables, and the indices that retained the relationship of linear changes in the scatter plots were leukocytes, neutrophils, lymphocytes, monocytes, platelets, NLR, FT3, FT4, and FT4/FT3. The results of one-dimensional linear regression analysis showed that the correlations between 25(OH)D and leukocytes, neutrophils, lymphocytes, monocytes, platelets, NLR, FT3, FT4, and FT4/FT3 were not significantly correlated (Table 6).
Correlation analysis of serum 25(OH)D levels with inflammatory parameters and thyroid function.

25(OH)D, 25-hydroxyvitamin D; CRP, C-reactive protein; ESR, erythrocyte sedimentation rate; FT3, free triiodothyronine; FT4, free thyroxine; NLR, neutrophil-to-lymphocyte ratio; PLR, platelet-to-lymphocyte ratio; TGAb, thyroglobulin antibodies; TPOAb, thyroperoxidase antibody; TSH, thyroid-stimulating hormone.

Scatterplot of serum 25(OH)D levels versus FT4/FT3.
Linear regression analysis of serum 25(OH)D with thyroid function and inflammatory parameters.
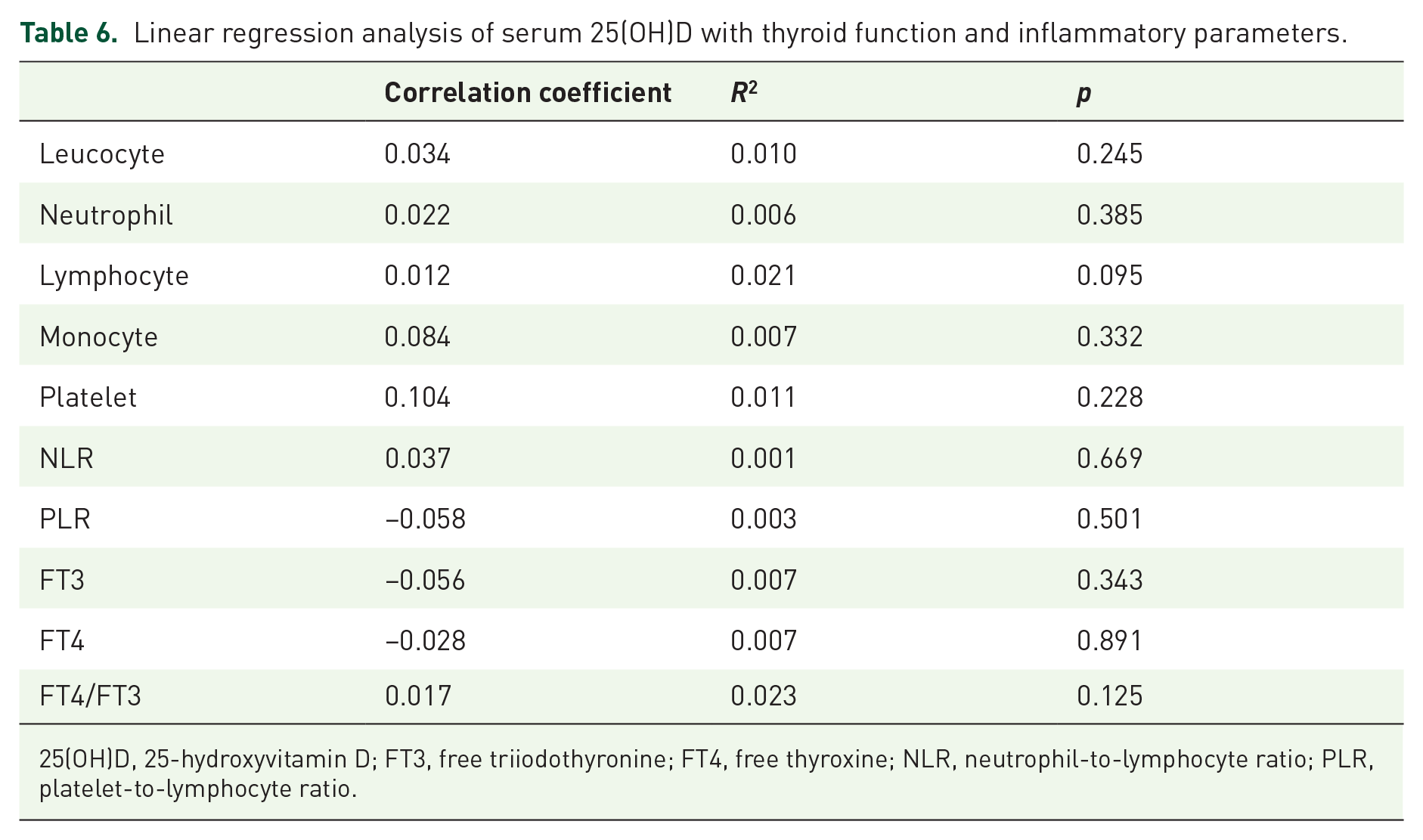
25(OH)D, 25-hydroxyvitamin D; FT3, free triiodothyronine; FT4, free thyroxine; NLR, neutrophil-to-lymphocyte ratio; PLR, platelet-to-lymphocyte ratio.
Discussion
VD plays a wide range of roles; in addition to its function of regulating calcium and phosphorus metabolism and maintaining bone health, it is also involved in tissue cell differentiation, proliferation, and immune regulation. 14 However, VD deficiency and insufficiency have now become one of the most common global public health problems. An increasing number of studies have shown that VD deficiency is closely related to the development of thyroid-related diseases. It has been found that patients with thyroid disorders such as Hashimoto’s thyroiditis, Graves’ disease, hypothyroidism, and thyroid tumors have significantly lower levels of VD than the healthy population,15–19 and increasing VD levels may reduce the risk of thyroid disorders. 20 There are few studies on the relationship between VD and SAT, and the conclusions are inconsistent. Therefore, this study aimed to assess VD levels in patients with SAT and conduct a preliminary investigation on the relationship between VD levels and the onset and extent of SAT.
SAT is a painful thyroid disorder that usually occurs after an upper respiratory viral infection. VD, a steroid hormone, is also an important immunomodulatory.21,22 VD deficiency disrupts the integrity of the tight junctions in the body’s cells, leading to viral invasion 4 thus increasing the prevalence of upper respiratory tract infections. 23 The occurrence of SAT may be associated with HLA-B*35 24 and recent studies have also observed that the presence of HLA-B*18:01, HLA-DRB1*01, HLAC*04:01, and HLA-A02:09 are associated with an increased risk of genetic susceptibility to SAT. 1 HLAs are a group of proteins encoded by histocompatibility complex genes, located on the distal part of the short arm of human chromosome 6, that recognize antigens presented to T lymphocytes to regulate adaptive immune responses. 25 VD receptor (VDR) response elements are present in the promoter region of some HLA alleles, and VD may play a role in the pathogenesis of SAT by binding to VDR to regulate HLA gene expression and thus SAT susceptibility genes.26–28 Regulatory T cells are a class of CD4+ T cell subpopulation that can inhibit the function of T cells and antigen-presenting cells by secreting cytokines such as interleukin-10, reducing the production of inflammatory factors and antibodies, and exerting immunosuppressive effects. 29 The number of regulatory T cells is reduced in the peripheral blood of SAT patients, but their expression is elevated in the thyroid gland, and this redistribution state may be an important factor in the pathogenesis of SAT. 30 In addition, VD enhances innate immunity, suppresses adaptive immunity, and induces immune tolerance in the body 31 ; it also reduces monocyte adhesion and antigen presentation, decreases the expression and secretion of interleukin-12 in macrophages and dendritic cells, 32 and directly inhibits the proliferative and secretory capacity of interleukin-2 and γ-interferon in T-lymphocytes. 33 VD also directly affects B cell homeostasis, including the inhibition of plasma cell production and the promotion of apoptosis in immunoglobulin-producing B cells. 34 In our study, we found that 25(OH)D levels were significantly lower in SAT patients than in healthy controls, and that low levels of 25(OH)D were an independent risk factor for the development of SAT.
There are few studies on the relationship between SAT and VD with inconsistent conclusions. In a study by Korkmaz et al. 1 and Calapkulu et al., 7 SAT patients were found to have significantly lower 25(OH)D levels than healthy controls (13.3 ± 5.1 vs 18.6 ± 9.3 ng/mL, p < 0.001), and similarly, a retrospective study reported lower 25(OH)D levels in SAT patients (13.5 ± 1.8 vs 16.7 ± 2.0 ng/mL, p < 0.001). However, a study by Stasiak and Lewiński 2 and Xiaoli et al. 9 did not observe a significant difference in VD levels between SAT patients and healthy controls. It is well known that the detection level of 25(OH)D is greatly influenced by the season, light duration, and lifestyle habits, and reasons for the inconsistency of the above studies are related to the time of inclusion of cases and the failure to consider the above-influencing factors. However, we hypothesize that VD is involved in the development of SAT and that adequate VD may be a means of preventing SAT, which needs to be further verified by future studies with larger samples.
The clinical guidelines of the American Thyroid Association recommend prioritizing the use of NSAIDs in patients with mild SAT and glucocorticoids in those with moderate-to-severe SAT. 13 In this study, subgroup analyses were conducted with and without glucocorticoid application, and the results suggested that the proportions of fever, neck pain, goiter, and thyroid tenderness, as well as the leukocyte counts, neutrophil counts, platelet counts, NLR, PLR, ESR, CRP, and FT4 were significantly higher in moderate-to-severe SAT than in mild SAT (p < 0.05). The levels of TSH were significantly lower in moderate-to-severe SAT than in mild SAT (p < 0.05). These results are consistent with the clinical characteristics of SAT patients: moderate-to-severe SAT has a more severe inflammatory response, more destruction of thyroid follicular epithelial cells, and more extracellular release of thyroid hormones. Surprisingly, the BMI of mildly ill patients in our study was significantly lower than that of moderate-to severe ill patients (p < 0.05) based on the theory that moderate-to-severe SAT patients with a longer duration of illness and more pronounced symptoms of thyrotoxicosis would have a lower BMI than mildly ill patients. In response to these results, we analyzed the following possibilities: first, we did not include the baseline BMI of the patients before disease onset, as if we had compared the difference between the BMI at the time of consultation and before the onset of the disease, the results may have been different. Second, the sample size of patients with mild SAT was relatively small, and the sample size of patients with moderate-to-severe SAT was relatively large, which might be related to the fact that some of the patients with mild SAT who showed self-limiting improvement did not present to the hospital for consultation. Third, there is a close relationship among BMI, leptin, and immunity. High BMI is associated with a high concentration of leptin, which activates the STAT3/NF-κB signaling pathway and secretes a large amount of pro-inflammatory factors, triggering a storm of inflammatory factors and leading to disease progression.35–38 Another study found that the expression of the leptin receptor was increased in the orbital tissues of patients with thyroid-associated ophthalmopathies and promotes collagen fibrillogenesis and inflammatory cell infiltration, aggravating thyroid-related eye disease. 39 We hypothesize that leptin may play a role in SAT.
Next, we explored the relationship between VD and the extent of SAT. There was no statistically significant difference in VD levels between patients with mild SAT and those with moderately severe SAT. Logistic regression analysis showed that VD levels were not a risk factor for the severity of SAT (p > 0.05). This is inconsistent with our speculation; as of now, there are no similar related studies for comparative reference. We consider that general VD deficiency in the included SAT population and the generally low baseline level of 25(OH)D have a certain impact on the results of this study, so the next step is to continue to expand the sample size and stratify the analysis of SAT patients with the onset of disease in different seasons to further confirm and validate our results. The results of this study suggest that fever, thyroid tenderness, elevated BMI, and elevated FT4 are risk factors for severe SAT (p < 0.05), and that severe SAT has a higher inflammatory response and a more pronounced thyrotoxic response, whereas the findings of recurrent fever and/or high fever peaks, pronounced thyroid tenderness, and high blood FT4 levels are consistent with the clinical characteristics of more severe disease.
The present study further explored the correlation of VD with inflammatory parameters and indicators of thyroid function. Spearman’s correlation analysis showed that 25(OH)D levels were significantly and positively correlated with FT4/FT3 (p < 0.05). The synthesis and secretion of thyroid hormones are mainly subject to feedback regulation by the hypothalamic-pituitary-thyroid axis. The pituitary secretes thyrotropin, which stimulates the thyroid gland to produce thyroxine (T4) and triiodothyronine (T3), of which T4 is the main hormone produced and released by the thyroid gland, which is further converted to T3 through deiodination of deiodinase, and the free state of T3 and T4 enters the cell to exert physiological effects. 40 As the thyroid hormone receptor has a 10-fold higher affinity for T3 than for T4, T4 must be converted to T3 to produce potent biological activity, and the FT4/FT3 ratio reflects the efficiency of the conversion of FT4 to FT3, which is considered a surrogate for evaluating the degree of deiodination of peripheral thyroxine and the activity of deiodinase. 41 Chen et al. 42 first reported the relationship between FT3/FT4 and VD levels as an inverted U-shaped relationship between FT3/FT4 and serum VD levels in the U.S. population, with FT3/FT4 decreasing with increasing VD levels when VD levels exceeded 25.43 ng/mL. More VD binds to the VDR on thyroid cells and reduces the number of TSH receptors in a concentration-dependent manner, resulting in the inability of TSH to bind to enough TSH receptors to fully exert its thyroxine-promoting effects, thus rendering TSH insensitive to changes in peripheral FT4; it has also been found that high levels of VD in hyperthyroidism inhibit TSH secretion, thereby decreasing T4 synthesis and secretion, and if there is not enough T4 to be converted to T3, the relative decrease in FT3 will be greater. 42 Combined with the results of the present study, in which higher levels of 25(OH)D were associated with higher FT4/FT3 ratios, we hypothesized that appropriately high levels of VD in patients with SAT might inhibit the conversion of FT4 to FT3, thereby attenuating the body’s thyrotoxicosis. However, linear regression analysis of 25(OH)D did not correlate with thyroid function and inflammation indices, and the r value of Spearman’s analysis was low. We analyzed that it might be related to the higher incidence of VD insufficiency in the population included in SAT, the generally low baseline level of VD, and the low number of cases of mild SAT. With the results of the above analysis, we hypothesized that VD plays a certain protective role in the development of SAT, perhaps not by reducing inflammatory response but by affecting the deiodinase activity and inhibiting the conversion of FT4 to FT3 to improve the condition of SAT patients.
This study has some limitations. First, this study is a single-center case-control study, which may have biased the results to some extent given the restricted geographical area and study population. Second, this study did not follow up the patients with SAT, and it is not known if there is a relationship between the VD nutritional status and the recurrence of SAT. Third, this study did not involve the interventional therapy study of VD supplementation. Despite these limitations, to our knowledge, this is the first time the relationship between VD and the risk of SAT and the extent of disease has been explored, which provides new ideas for the next steps into in-depth research on the relationship between the two and the related mechanisms.
Conclusion
Our study found that patients with SAT had significantly lower VD levels than healthy controls and that reduced VD levels were an independent risk factor for the development of SAT. There was no statistically significant difference in VD levels between patients with mild SAT and those with moderately severe SAT. VD levels were not related to the degree of SAT disease, but 25(OH)D levels were positively correlated with FT4/FT3, and we hypothesized that adequate VD levels inhibited the conversion of FT4 to FT3, attenuated the symptoms related to hyperthyroidism in patients with SAT, and played a protective role in SAT progression. This preliminary study investigated the correlation between VD and SAT and provided a partial basis for future research on the relationship between the two, which still needs further verification by multicenter large-scale randomized controlled trials.
Supplemental Material
sj-doc-1-tae-10.1177_20420188251321600 – Supplemental material for Analysis of vitamin D nutritional status and disease risk factors in patients with subacute thyroiditis
Supplemental material, sj-doc-1-tae-10.1177_20420188251321600 for Analysis of vitamin D nutritional status and disease risk factors in patients with subacute thyroiditis by Rongrong Wang, Dehuan Kong and Xiaoqing Ma in Therapeutic Advances in Endocrinology and Metabolism
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.