
Abstract
Background:
The aldosterone-to-renin ratio (ARR) is commonly used for screening primary aldosteronism (PA) in patients with difficult-to-control hypertension. Various thresholds have been proposed for the confirmatory tests, leading to inconsistency in the results.
Objectives:
This study aimed to elucidate the performance of ARR screening in hypertensive patients.
Design:
Systemic review and meta-analysis.
Data sources and methods:
PubMed, Embase, and the Cochrane Library were systematically searched from inception to January 2024. Studies that used the ARR to screen for PA and provided a comprehensive probability panel specifically focusing on hypertensive individuals were considered for enrollment. Pooled diagnostic efficacy was evaluated, and subgroup analyses and meta-regression were conducted based on different demographic and clinical parameters.
Results:
Eighteen observational studies encompassing 7150 participants were included in the meta-analysis. The overall prevalence of PA in the hypertensive cohort was 15.2%, and pooled sensitivity and specificity were 81.6% and 93.3%, respectively, resulting in a diagnostic odds ratio of 62.0. Fagan’s nomogram showed that a positive ARR increased the post-test probability to 80% from a pre-test probability of 25%. Summary receiver operating characteristic curve analysis revealed an area under the curve of 94.7%. Notably, analysis of variability demonstrated that the diagnostic performance was consistent across either ARR based on plasma renin activity or direct renin concentration, geographic region, sex, mean age, potassium level, and systolic blood pressure.
Conclusion:
ARR was validated as a viable screening methodology for PA in hypertensive individuals. Moreover, its diagnostic efficacy remained unchanged across diverse clinical contexts. Future studies are warranted to refine ARR methodologies and enhance diagnostic accuracy.
Trial registration:
PROSPERO ID number CRD42023493680.
Infographics
ARR, aldosterone-to-renin ratio; BP, blood pressure; DRC, direct renin concentration; hsROC, hierarchical summary receiver operating characteristic; PA, primary aldosteronism; PRA, plasma renin activity.

Plain language summary
Primary aldosteronism constitutes a significant etiology of secondary hypertension. However, historical under-recognition has resulted in delayed diagnosis and compromised prognoses. The aldosterone-to-renin ratio is universally recommended as the primary screening tool for primary aldosteronism. This meta-analysis systematically reviewed existing literature to evaluate the diagnostic accuracy of aldosterone-to-renin ratio. Subgroup analyses and meta-regression incorporating covariates demonstrated consistent performance across diverse demographic and clinical contexts. These findings support the broader implementation of aldosterone-to-renin ratio screening in hypertensive patients.
Introduction
Primary aldosteronism (PA) is increasingly recognized as the primary etiology of secondary hypertension worldwide. Global epidemiological studies have reported a prevalence of PA ranging from 5.9% to 11.2% in patients with hypertension, and up to 20% in those with resistant hypertension.1,2 Elevated blood pressure, hypokalemia, and metabolic alkalosis are the hallmark presentations of PA. Compared with essential hypertension, the poor outcomes associated with PA are not exclusively attributed to high blood pressure, but also to systemic complications of excessive circulating aldosterone. Associations between PA with various conditions including atherosclerosis, myocardial remodeling, cerebrovascular events, and renal insufficiency have been reported, 3 and a prompt diagnosis remains pivotal to facilitating targeted PA treatment and improving the prognosis.
The indications for PA screening are traditionally limited to patients with difficult-to-treat hypertension. The diagnosis of PA is traditionally based on consequential screening and confirmatory tests. Although the methodologies used to evaluate aldosterone suppression to confirm PA are heterogeneous, the aldosterone-to-renin ratio (ARR) remains the most widely applied screening tool for PA since its introduction in 1981, 4 due to its ease of use in the outpatient setting. Although race and ethnicity have been addressed as important factors for hypertension and its etiologies, 5 ARR has been endorsed globally by guidelines from the Endocrine Society, 6 Europe, 7 Taiwan, 8 Korea, 9 Japan, 10 and North America 11 and widely applied to detect PA in European, 12 Asian, 13 North, 14 and South American 15 cohort studies with fair consistency. However, the cutoff values used in previous studies and targeted cohorts have varied, leading to discordant diagnostic performance. Therefore, the undetermined efficacy of screening tests remains an unmet clinical need, as it may diminish or amplify the PA confirmation rate.
Previous pooled analyses regarding PA diagnosis are also either out of date or involve pronounced bias. With the increase in the number of observational studies, revisiting the literature related to PA screening and further comprehensive diagnostic meta-analyses are important to elucidate the accuracy of ARR as a screening test for PA. Therefore, the aims of this study were to elucidate the performance of ARR screening in hypertensive patients and investigate the performance of screening tests across different patient phenotypes to validate their applicability.
Methods
Search strategy
PubMed/Medline, Embase, and the Cochrane Library were searched from inception to January 2024 using the keywords “aldosterone-to-renin ratio” and “primary aldosteronism.” No language restrictions were implemented, and only human studies were included. Gray literature including conference abstracts was not considered. Study enrollment was carried out following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) algorithm. The inclusion criterion was studied that used the ARR to screen for PA. Studies that applied other parameters for PA screening, did not target adult hypertensive patients, did not perform subsequent confirmatory tests to diagnose PA, reported incomplete probability panels, and those with only one patient were excluded. The protocol of this study was registered on PROSPERO (ID number CRD42023493680).
Data extraction
Respective titles and abstracts of the enrolled studies were screened independently by two authors (T.-W.K., Z.-W.C.). The manuscripts and references were subsequently reviewed by all study investigators to determine eligibility for final inclusion. Any disputes were resolved based on consensus. The study design, baseline demographic and clinical characteristics of the cohorts, ARR, reported cutoff values, and true positive, false positive, true negative, and false negative results were extracted directly from full-text studies.
Statistical analysis
We used a 2 × 2 table to report the patient numbers with true positive, false positive, true negative, and false negative findings based on the cutoff point specified in the included studies. This table enabled us to calculate sensitivity, specificity, and diagnostic odds ratio (DOR) for each study. A bivariate model was used to aggregate sensitivity, specificity, and DOR across all of the included studies. 16 Higher DOR indicates that the examined test could better dichotomously distinguish the presence or absence of the event. 17 Besides, Fagan’s nomograms were composed to determine the post-test probability of PA screening test based on estimated pre-test probabilities. We also performed a hierarchical summary receiver operating characteristic (ROC) curve analysis, taking the threshold effect into consideration, to illustrate the overall diagnostic performance of the screening test. 18 We further evaluated potential publication bias through the visual examination of funnel plots.
Analysis of variability was carried out to elucidate the impact of clinical contexts on the performance of ARR screening regarding substantial heterogeneity among studies. We conducted a sensitivity analysis by excluding two studies in which antihypertensive agents were not discontinued before the screening test and one study in which the status of antihypertensive agents was not specified. Covariate subgroup analyses and meta-regression were performed, respectively, on categorical (ARR based on two measurement methodologies: plasma renin activity (PRA) or direct renin concentration (DRC), geographic region of the study, and methodologies for aldosterone measurement: radioimmunoassay and chemiluminescent immunoassay) and continuous (male proportion, mean age, mean serum level of potassium, systolic blood pressure) variables. A two-sided p value <0.05 was considered statistically significant. The bivariate model was performed using SAS version 9.4 (SAS Institute, Cary, NC, USA) and the recommended “METADAS” macro (version 1.3) by the Cochrane Diagnostic Test Accuracy Working Group. Utilizing R software version 4.3.2 with the “meta4diag” package (version 2.1.1), we conducted the ROC analysis and generated funnel plots based on Bayesian inference with 5000 posterior samples.
Quality of evidence and risk of bias
The Quality Assessment of Diagnostic Accuracy Studies-2 tool was used to evaluate the risk of bias among the included studies (Supplemental Figure 1). 19 Deeks’ funnel plots were used to evaluate publication bias.
Results
Search results
During the initial search, a total of 305 articles were screened, of which 16 were excluded after removing duplicates, and another 216 were excluded due to irrelevant titles and/or abstracts. The remaining 73 studies were reviewed for eligibility, of which 30 were analyzed for quality. Eventually, a total of 18 studies were included for meta-analysis20–37 (Figure 1).
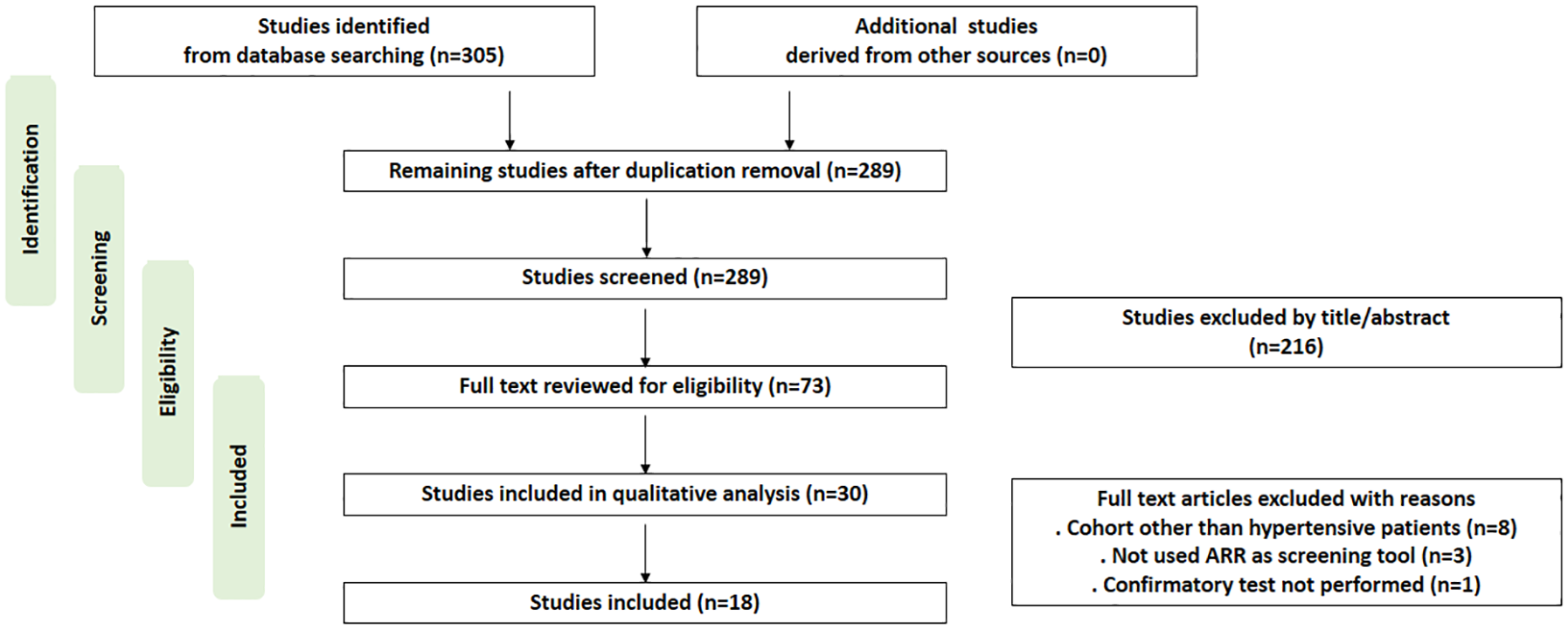
Flowchart of study inclusion.
Study characteristics
All the included studies were observational cohort studies published from 2000 to 2023. Among the included 7150 hypertensive subjects, the prevalence of PA was 15.2%. ARR was measured after discontinuation of potential interfering drugs, except in three studies: one that did not specify the status of antihypertensive agents, and two in which all medications were purposely continued (Supplemental Table 1). The sample sizes ranged widely from 55 to 1125 subjects. Seven, four, and eight of the studies were conducted in Europe, America, and Asia (China and Japan), respectively. Most of the patients were normokalemic, and the hypertensive statuses included resistant, difficult-to-treat, newly diagnosed, and in general. ARR was calculated based on PRA in 12 studies and DRC in 5 studies. One study reported probability profiles of ARR with both PRA and DRC. The cutoff values varied widely between different institutions. Detailed demographic and clinical parameters of the included studies are listed in Table 1.
Baseline demographic and clinical characteristics.
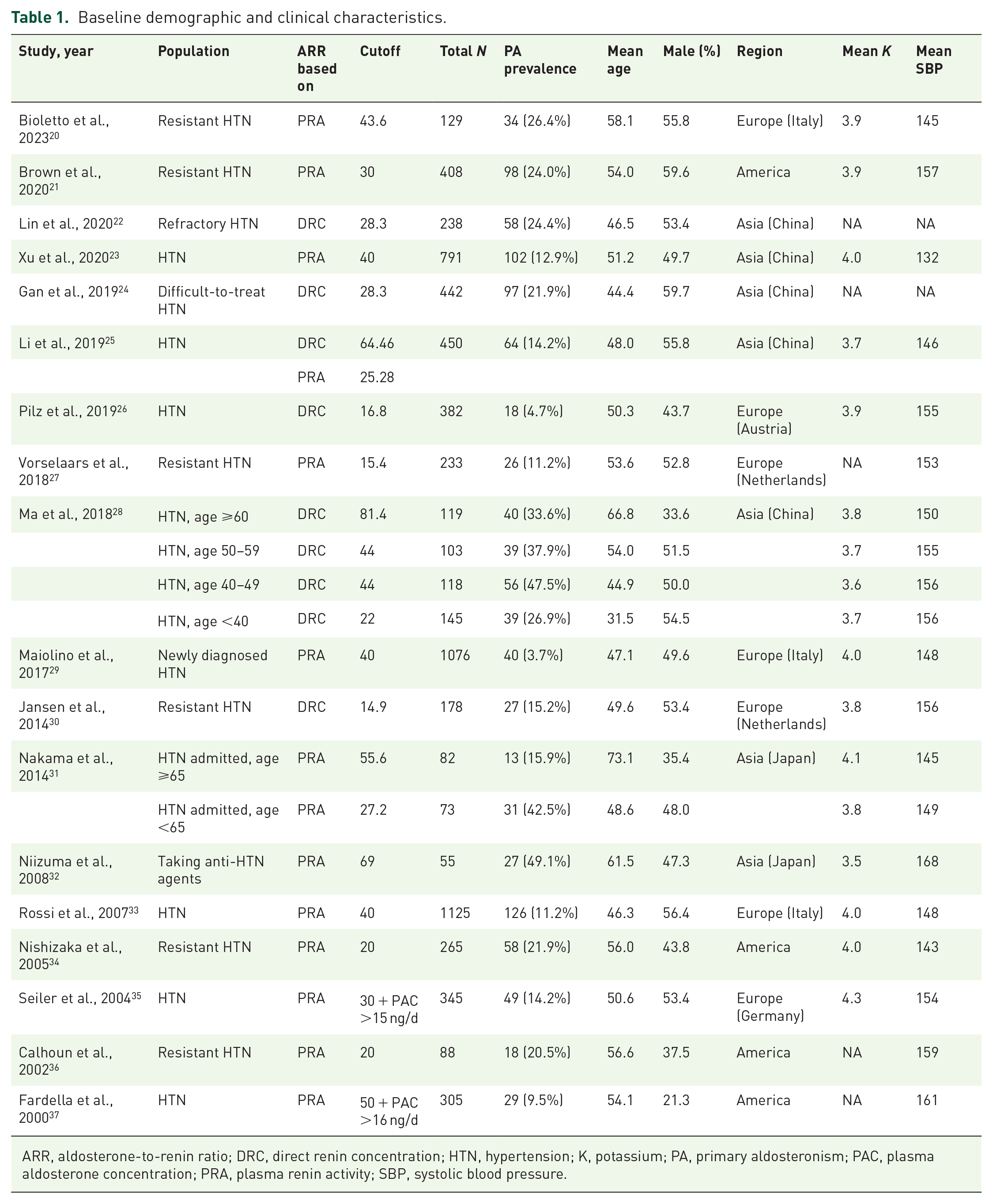
ARR, aldosterone-to-renin ratio; DRC, direct renin concentration; HTN, hypertension; K, potassium; PA, primary aldosteronism; PAC, plasma aldosterone concentration; PRA, plasma renin activity; SBP, systolic blood pressure.
Pooled sensitivity and specificity
Derived from the reported cutoff values in the included studies, the pooled sensitivity was 81.6% (95% confidence interval (CI), 69.6%–89.5%) and the pooled specificity was 93.3% (95% CI, 88.2%–96.3%) (Figure 2). Overall, the DOR was 62.0 (95% CI, 33.3–115.3). In addition, Fagan’s nomograms showed that a positive ARR increased the post-test probability to 80%, 92%, and 97% from a pre-test probability of 25%, 50%, and 75%, respectively (Figure 3). The estimated areas under the ROC curves were 95.0% (95% CI, 91.6%–96.6%) for all studies, 93.8% (95% CI, 89.0%–96.1%) for studies with the ARR based on PRA, and 96.6% (95% CI, 89.9%–98.9%) for studies with the ARR based on DRC (Figure 4).

Pooled sensitivity and specificity of included studies. 95% confidence intervals were expressed by error bars.

Fagan nanogram of screening tests by designating pre-test probability as (a) 25%, (b) 50%, and (c) 75%.

Rutter and Gatsonis’s hierarchical summary receiver operating characteristic curve. The circles represented observed estimates of respective studies, with size proportional to weight. (a) All studies. (b) Studies with ARR based on PRA. (c) Studies with ARR based on DRC.
Analysis of variability
After excluding three studies in which the antihypertensive agents were not discontinued, the sensitivity analysis showed similar pooled sensitivity, specificity, and DOC. Subgroup analyses and meta-regression were performed to investigate the performance of the screening tests across heterogeneous clinical contexts of the included cohorts (Table 2). In the studies using ARR based on PRA as a reference, there were no significant differences in the relative sensitivity (1.06, 95% CI, 0.94–1.20), specificity (1.00, 95% CI, 0.97–1.03), and DOR (1.39, 95% CI, 0.61–3.14) using ARR based on DRC. Regarding the geographic region of the study, numerically lower sensitivity and slightly higher specificity of ARR were found in the American studies, yielding a reduced DOR. However, there were no statistically significant differences in relative sensitivity, specificity, and DOR. Regarding the methodologies for aldosterone measurement, the relative sensitivity (1.10, 95% CI, 0.90–1.35), specificity (1.02, 95% CI, 0.92–1.13), and DOR (2.84, 95% CI, 0.54–14.54) for radioimmunoassay, compared to chemiluminescent immunoassay, remained similar.
Overall, sensitivity and stratified analysis of categorical subgroups and meta-regression of continuous variables.

Two studies in which the antihypertensive agents were not discontinued and one study in which the status of antihypertensive agents was not specified were excluded.
ARR, aldosterone-to-renin ratio; CI, confidence interval; CLIA, chemiluminescent immunoassay; DOR, diagnostic odd ratio; DRC, direct renin concentration; PRA, plasma renin activity; RIA, radioimmunoassay; SBP, systolic blood pressure.
The impacts of continuous variables were assessed by meta-regression (Table 2). Eighteen studies reported the sex and mean age of the included cohort. The relative probability panel remained unchanged for every 10% of the male proportion or for every 5 years of age. Regarding electrolyte status, 14 studies reported mean serum levels of potassium. The performances of the screening tests were comparable for every 0.1 mEq/L. Finally, for systolic blood pressure, 17 studies were pooled for every 5 mmHg, and no remarkable differences were found. To study whether ARR based on PRA or DRC affected the outcomes of meta-regression, we performed analyses further stratified by these two groups, which again revealed no remarkable differences.
Risk of bias was otherwise low except for a remarkable risk of bias in participant selection. The likelihood of publication bias was low, with non-significant asymmetry (all: p = 0.641; studies with ARR based on PRA: p = 0.144; studies with ARR based on DRC: p = 0.335; Supplemental Figure 2).
Discussion
This study is the most recent and extensive meta-analysis to analyze the diagnostic performance of PA screening using ARR in patients with hypertension. The analysis involved 7150 hypertensive subjects, and there were 4 key findings. First, substantial heterogeneity was found among the studies regarding optimal cutoff values and patient characteristics. Second, overall fair sensitivity and specificity of ARR screening were found across the studies, with high area under the curve (AUCs). Third, no notable disparity was found in ARR screening efficacy based on either PRA or DRC. Fourth, the diagnostic performance of ARR was independent of geographic region (based on selected countries in which the studies were performed), age, sex, potassium level, and systolic blood pressure.
Excessive levels of endogenous circulating aldosterone have been reported to significantly contribute to secondary hypertension, underscoring the importance of enhancing the efficacy of screening. However, epidemiological studies have reported that only 3% of individuals with resistant hypertension receive PA screening. In particular, male and Asian (Chinese, Japanese) patients have the lowest rates of PA screening. 38 In this study, we exclusively enrolled patients with hypertension to minimize bias introduced by different cohort backgrounds and the prevalence of PA. The overall prevalence of PA in our study aligns with prior reports. Two previously published meta-analyses explored similar themes. Hung et al. 39 pooled 10 studies, of which 2 involved normotensive subjects. Two studies used ARR based on PRA, whereas the rest used ARR based on DRC as the screening tests. The analysis was performed by pooling all studies regardless of whether they used ARR based on DRC or PRA, and the overall sensitivity and specificity were similar to our results. We exclusively enrolled patients with hypertension to minimize bias introduced by different cohort backgrounds and the prevalence of PA. Another meta-analysis conducted by Gao et al. 40 also proposed a similar probability panel; however, several studies were domestic and potentially had a significant risk of bias. Interestingly, a more pronounced difference in specificity rather than sensitivity was evident throughout these studies.
ARR is a reproducible and reliable parameter to evaluate non-suppressible aldosterone activity. ARR is the sole recommended index for PA screening and it be calculated using DRC, which requires less cumbersome processing and is potentially more accurate. Nevertheless, despite its simplicity and utility in PA screening, it’s important not to overlook the fluctuating nature of ARR under different sampling conditions. 41 According to the Framingham Heart Study, ARR is easily affected by clinical factors, 42 including age, sex, race, body mass index, sodium intake, posture, circadian rhythm, and quantification method for serum aldosterone (radioimmunoassay or chemiluminescent assay). 43 A prior investigation found a fair correlation between PRA and DRC, 44 however, the cutoff values for the confirmatory tests were heterogeneous. As highlighted in a previous international multicenter survey, 45 substantial heterogeneities remained regarding how PA was diagnosed and further standardization of the protocol was urgently needed. In our analysis, we noticed most of the studies used ARR based on PRA, and pooled sensitivity and specificity as well as the AUCs were comparable between ARR based on PRA and DRC. Furthermore, subgroup analysis suggested that the diagnostic performance was not significantly affected by the choice of either index.
Various clinical factors have been proposed to affect the ARR threshold for PA diagnosis, necessitating adjustments of screening test cutoff values to maintain optimal efficacy. A previous study suggested using a higher ARR for older adults to reflect the diminished suppression of plasma renin. 46 A trend of a higher threshold was noted in the older patients; however, our results showed that age did not alter the performance of screening tests after adjustment. In addition, the subgroup analyses and meta-regression in our study showed that the underlying status of the cohort did not markedly alter the efficacy of the screening tests. For example, potassium directly affects the renin–angiotensin system and impacts both renin and aldosterone levels. 47 Although guidelines recommend correcting for hypokalemia before assessing ARR, 48 our meta-analysis suggested that the performance of the tests was not affected by baseline serum potassium level. Before excluding other possible confounders, interpretation of the screening results should still be done with caution. Future studies should focus on standardizing screening protocols to achieve optimized efficacy.
Although this is the most extensive investigation of PA screening tests to date, several limitations should be noted. First, the subgroup analyses in this study were performed on a restricted set of parameters. We were unable to incorporate all patient characteristics that could potentially impact screening test performance. Stratified analysis should be updated as the literature grows to better phenotype all individuals. Additionally, the comparison of diagnostic performance between ARR alone and the combination of ARR with PAC was not performed due to limited statistical power. Second, confirmatory testing is affected by individual sensitivity and specificity, which could potentially result in misclassification. However, using confirmation tests as a surrogate reference standard is currently the sole method to determine the false negative rate of ARR testing. 49 The inherent uncertainties surrounding confirmatory tests could also complicate efficacy evaluations of the screening test. Third, claiming that the performance of ARR is entirely independent of geographic region may not be entirely accurate, as the countries where these cohort studies were conducted may not necessarily represent the status across the entire geographic region. Fourth, all the included studies were observational in nature, which would inevitably introduce bias. Since randomization is not feasible regarding screening tests, a diagnostic meta-analysis is mandatory to validate its performance.
Conclusion
Screening for PA using ARR based on either PRA or DRC is a feasible approach with ideal sensitivity and specificity in patients with hypertension. The screening performance remained consistent across patients with diverse demographic and clinical backgrounds. Future studies are essential to further refine ARR examination methodologies, improve the diagnostic performance of ARR as a screening test, and revise current guidelines. For now, ARR should be utilized to facilitate early diagnosis and targeted treatment of PA in patients with hypertension, regardless of other clinical factors.
Supplemental Material
sj-docx-1-tae-10.1177_20420188241303429 – Supplemental material for Diagnostic efficacy of aldosterone-to-renin ratio to screen primary aldosteronism in hypertension: a systemic review and meta-analysis
Supplemental material, sj-docx-1-tae-10.1177_20420188241303429 for Diagnostic efficacy of aldosterone-to-renin ratio to screen primary aldosteronism in hypertension: a systemic review and meta-analysis by Ting-Wei Kao, Jui-Yi Chen, Jung-Hua Liu, Wen-Hsin Tseng, Chih-Chia Hsieh, Vin-Cent Wu, Yen-Hung Lin and Zheng-Wei Chen in Therapeutic Advances in Endocrinology and Metabolism
Supplemental Material
sj-docx-2-tae-10.1177_20420188241303429 – Supplemental material for Diagnostic efficacy of aldosterone-to-renin ratio to screen primary aldosteronism in hypertension: a systemic review and meta-analysis
Supplemental material, sj-docx-2-tae-10.1177_20420188241303429 for Diagnostic efficacy of aldosterone-to-renin ratio to screen primary aldosteronism in hypertension: a systemic review and meta-analysis by Ting-Wei Kao, Jui-Yi Chen, Jung-Hua Liu, Wen-Hsin Tseng, Chih-Chia Hsieh, Vin-Cent Wu, Yen-Hung Lin and Zheng-Wei Chen in Therapeutic Advances in Endocrinology and Metabolism
Footnotes
Acknowledgements
The article was benefited from statistical assistance provided by Alfred Hsing-Fen Lin, MS, and Ben Yu-Lin Chou, MPH, Raising Statistics Consultant Inc., for the assistance in statistical analysis of this study.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.