
Abstract
Background:
The prevalence of type 2 diabetes mellitus (T2DM) continues to increase; the clinical practice guidelines continue to modify the recommendations for its treatment.
Objective:
The aim was to determine the prescription patterns of noninsulin antidiabetics in a group of patients from Colombia.
Design:
Cross-sectional study.
Methods:
The use of noninsulin antidiabetic drugs based on a population database of patients under treatment in 2022. Comorbidities were identified, including total numbers, proportions, and defined daily doses of each antidiabetic agent per 1000 inhabitants/day (DHD).
Results:
A total of 155,381 patients with T2DM were identified, with a mean age of 67.1 ± 12.0 years. The most widely used antidiabetics according to DHD were metformin (9.46 DHD), empagliflozin (5.3), sitagliptin (2.8), linagliptin (2.4), and dapagliflozin (2.3), mainly in combination therapy (55.5%), most often two (31.2% of patients) or three antidiabetics (22.4% of patients). The most frequent cardiovascular comorbidities were hypertension (67.6%), chronic kidney disease (6.3%), and coronary ischemic heart disease (2.5%), treated with angiotensin 2 receptor antagonists, followed by diuretics, calcium antagonists, and β-blockers.
Conclusion:
This group of patients with T2DM has been treated mainly with metformin alone or in combination with other antidiabetic drugs, but despite the changes in treatment in recent years, a significant number of patients with concomitant cardiovascular conditions are not receiving appropriate antidiabetic agents. Sodium-glucose type 2 cotransporter or glucagon-like peptide-1 receptor agonists may offer additional benefits with reduced cardiovascular risk.
Plain language summary
Pharmacological treatment recommendations for patients with type 2 diabetes mellitus are changing rapidly in recent years, with the introduction of new medications that improve cardiovascular outcomes. This study identified the prescription patterns of noninsulin antidiabetics in patients with a diagnosis of T2DM affiliated with the Colombian health system. The patterns reflect the changes that have occurred after the introduction of new technologies such as SGLT2is and GLP1-ras, which open prospects for cardiovascular and renal protection in this group of people. These findings may be useful to treating physicians, health administrators, and those who draw up health policies since they collect information on individuals who have prescriptions made by general practitioners and specialists.
Keywords
Introduction
Diabetes mellitus (DM) affects approximately 10% of the world’s population, and its prevalence is increasing rapidly. 1 According to the High Cost Account, in Colombia which was a country with 51 million inhabitants in 2021, approximately 1,576,508 people had a diagnosis of DM, equivalent to a prevalence of 3.11 cases per 100 inhabitants, and its incidence is rising. 2 Patients with DM suffer micro- and macrovascular complications that lower their quality of life and significantly increase their mortality compared to those who do not suffer from this condition.3,4 A total of 3.7% of patients with DM died in 2021 in Colombia. 2
The American Diabetes Association (ADA) recommends a patient-centered therapeutic approach that involves lifestyle changes such as physical activity, weight loss, diet control, and medications that control carbohydrate metabolism, taking into account the efficacy, safety, costs, and clinical characteristics. The ADA makes special mention of comorbidities such as atherosclerotic cardiovascular disease, kidney disease, and heart failure. Metformin is the first-line drug in patients with type 2 DM (T2DM) without cardiovascular or renal complications.5–7
Medications belonging to the groups of sulfonylureas, thiazolidinediones, dipeptidyl peptidase type 4 inhibitors (DPP-4i), sodium-glucose cotransporter type 2 inhibitors (SGLT2is), glucagon-like peptide-1 receptor agonists (GLP1-ras), and insulins are among the therapeutic options for the combination therapy of T2DM.5,8 Although numerous trials have compared dual therapy with metformin, there is little evidence to support one combination over another. Taking into account cardiovascular risk, the presence of comorbidities such as heart failure, atherosclerotic disease, and chronic kidney disease, SGLT2is and GLP1-ras are recommended even in monotherapy as part of the glucose-lowering regimen, regardless of glycosylated hemoglobin levels. 5 Some molecules of both therapeutic groups have shown, in controlled clinical trials, a statistically significant reduction of cardiovascular events, such as acute myocardial infarction, cerebrovascular events, and cardiovascular death, as well as beneficial effects to slow the progression of chronic kidney disease.3,5,9–13 Despite the recommendations by the ADA regarding patients with T2DM at high risk with established cardiovascular disease, Colombia has found a high use of metformin and sulfonylureas and a low use of GLP1-ras and SGLT2is.5,14,15
The Colombian health system offers universal coverage to the entire population through two affiliation regimes, one contributory or paid by both the employer and the worker and the other subsidized by the state for those without the ability to cover their expenses, which counts with a benefit plan that includes all antidiabetics available in the country from the different pharmacological groups. Given that it is unknown how the use of antidiabetic drugs has evolved with the advent of new groups, we aimed to determine the prescription patterns of noninsulin antidiabetic drugs in a group of patients affiliated with the Colombian health system in 2022.
Methods
Population and sample
A cross-sectional study was conducted on the prescription patterns of the different drugs used for the treatment of T2DM according to a population-based drug dispensing database that collects information from approximately 9.2 million people affiliated with the Colombian health system through four health insurance companies, corresponding to approximately 28.0% of the active affiliated population of the contributory or payment scheme and 9.8% of the state-subsidized scheme, which together make up 17.5% of the Colombian population.
The data of individuals dispensed an antidiabetic drug during the quarter between September 1, 2022 and November 30, 2022, aged ⩾18 years, of either sex, treated in medical consultation, and whose treatment was unbroken for these 3 months were included. All patients who had only one or two dispensations of antidiabetic agents in the 3-month observation period were excluded. This requirement was monitored by dispensing the medication and was intended to ensure that patients complied with the treatment in a more or less stable manner, which reflects tolerability to the medication and adherence, while the people who missed medical appointments at the end of the observation period were excluded since we considered that these individuals would introduce biases in a study aimed at describing patterns of use of medications in a chronic and continuous way.
Based on the information on drug consumption of the affiliated population, systematically obtained by the dispensing company (Audifarma SA, Pereira, Colombia), we designed a database in which we gathered the following groups of variables:
Sociodemographic: sex, age, affiliation regime to the health system (contributory or subsidized), and place of residence. The place of residence was categorized into the regions used by the National Administrative Department of Statistics of Colombia: Bogotá-Cundinamarca, Caribbean, Central, Eastern, Pacific, and Amazon–Orinoquía.
Comorbidities: Comorbidities were identified from the main and secondary diagnoses reported by the codes of the International Classification of Diseases of the selected patients from September 1 to November 30, 2022. Cardiovascular disorders were particularly sought.
Type of prescriber: general practitioner or medical specialist (internal medicine, endocrinology, cardiology, among others).
Medications for the treatment of T2DM: biguanides (metformin), sulfonylureas (glibenclamide, gliclazide, glimepiride), thiazolidinediones (pioglitazone), GLP1-ra (exenatide, liraglutide, semaglutide, etc.), DPP-4is (vildagliptin saxagliptin, linagliptin, etc.), meglitinides (nateglinide, repaglinide), α-glycosidase inhibitors (acarbose), and SGLT2is (dapagliflozin, empagliflozin, canagliflozin). The information on the dose used was analyzed, considering as a unit the defined daily dose (DDD) and the estimated DDD per 1000 inhabitants/day (DHD).
Comedications: They were grouped into the following categories: (a) antihypertensives and diuretics, (b) lipid-lowering drugs, (c) nonopioid analgesics and anti-inflammatories, (d) antiulcer drugs, (e) antiplatelet drugs, (f) insulins, (g) thyroid hormone, and (h) antidepressants, (i) antiepileptic drugs, (j) opioid analgesics, (k) antihistamines, and (l) bronchodilators, among others.
Comparison with the study of antidiabetic prescription patterns from 2015: a comparison was made of the earlier treatment patterns used in Colombia. 15
The protocol was approved by the Bioethics Committee of the Technological University of Pereira in the category of “research without risk,” according to Resolution No. 8430 of 1993 of the Ministry of Health of Colombia, which establishes the scientific, technical, and administrative standards for health research (Endorsement code: 10-130223; date February 13, 2023). The principles established by the Declaration of Helsinki were respected.
The data were analyzed with the statistical software SPSS Statistics version 26.0 for Windows (IBM, Armonk, NY, USA) and Python 3 16 using the Pandas 1.4.1 library 17 and the Numpy 1.24.3 library. 18 Descriptive analyses were carried out with frequencies and proportions for the qualitative variables and measures of central tendency and dispersion for the quantitative variables. The UpSet library version 0.6.1 in Python was used to generate the figure of the combined consumption of drugs. 19
Results
Initially, 1,106,470 dispensing records were identified, which for the month of November 2022 corresponded to 374,765 patients. Of these, 158,835 were included who had deliveries of effective noninsulin antidiabetic drugs during the 3 months under study, and of them, 405 minors and those with no registered age were eliminated, as were 1593 who received an antidiabetic drug in its presentation for the management of obesity, leaving 155,381 patients who met all the inclusion criteria.
The mean age of the 155,381 eligible patients was 67.1 ± 12.0 years. The majority of the patients were women, especially from the Caribbean, Bogotá-Cundinamarca, and Central regions, who were most often cared for by general practitioners (see Table 1). The most frequently identified medical conditions in this group of patients were arterial hypertension (n = 105,001, 67.6%), chronic kidney disease (n = 9807, 6.3%), coronary ischemic heart disease (n = 5968, 3.8%), heart failure (n = 3853, 2.5%), and a history of cerebrovascular events (n = 327, 0.2%).
Sociodemographic and prescribing physician characteristics of a group of 155,381 patients diagnosed with type 2 diabetes mellitus affiliated with the Colombian health system, 2022.

SD, standard deviation.
All medications and presentations available in Colombia for the management of T2DM were considered. The prescription patterns of noninsulin antidiabetic drugs are shown in Table 2. The DHDs of the most commonly used noninsulin antidiabetics were, in descending order, metformin (DHD: 9.46), empagliflozin (5.53), sitagliptin (2.86), linagliptin (2.44), dapagliflozin (2.30), vildagliptin (1.67), glimepiride (0.17), gliclazide (0.12), glibenclamide (0.10), semaglutide (0.04), saxagliptin (0.02), dulaglutide (0.01), liraglutide (0.004), lixisenatide (0.001), and exenatide (0.0004).
Prescription patterns of noninsulin antidiabetics in a group of 155,381 patients with a diagnosis of type 2 diabetes mellitus affiliated with the Colombian health system, 2022.

Lixisenatide doses are presented in micrograms.
The doses of dulaglutide, exenatide, and semaglutide are weekly.
DDD, defined daily dose; DPP-4i, dipeptidyl peptidase type 4 inhibitors; GLP1-ras, glucagon-like peptide-1 receptor agonists; SGLT2i, sodium-glucose cotransporter type 2 inhibitors.
Combination therapy versus monotherapy
Of the included patients identified, 69,055 (44.4%) were treated with a single antidiabetic drug, while 86,326 (55.5%) were being treated with combinations of noninsulin antidiabetic drugs: two drugs in 48,467 (31.2%), three drugs in 34,828 (22.4%), four drugs in 2994 (1.9%), and five drugs in 37 (0.01). It should also be noted that 24.7% (n = 38,340) received some form of insulin.
Metformin alone or in combination was prescribed to 125,738 patients (80.9% of all patients), of whom 49.9% used it in combination with another antidiabetic drug. Most often it was prescribed along with a DPP-4i, followed by an SGLT2i (see Table 3).
Groups of noninsulin antidiabetics and main types of comedications of 155,381 patients with a diagnosis of diabetes mellitus under treatment, in Colombia, 2022.

ARNI, angiotensin receptor–neprilysin inhibitor; DPP-4i, dipeptidyl peptidase type 4 inhibitors; GLP1-ra, glucagon-like peptide-1 receptor agonists; SGLT2i, sodium-glucose cotransporter type 2 inhibitors.
The most frequently used treatment regimens were metformin alone (n = 45,965, 29.5% of all patients), followed by metformin plus a DPP-4i (n = 18,663, 12.0%). At least 61 different forms of antidiabetic combinations were identified (including insulins; the regimens used by at least 200 patients can be seen in Figure 1).
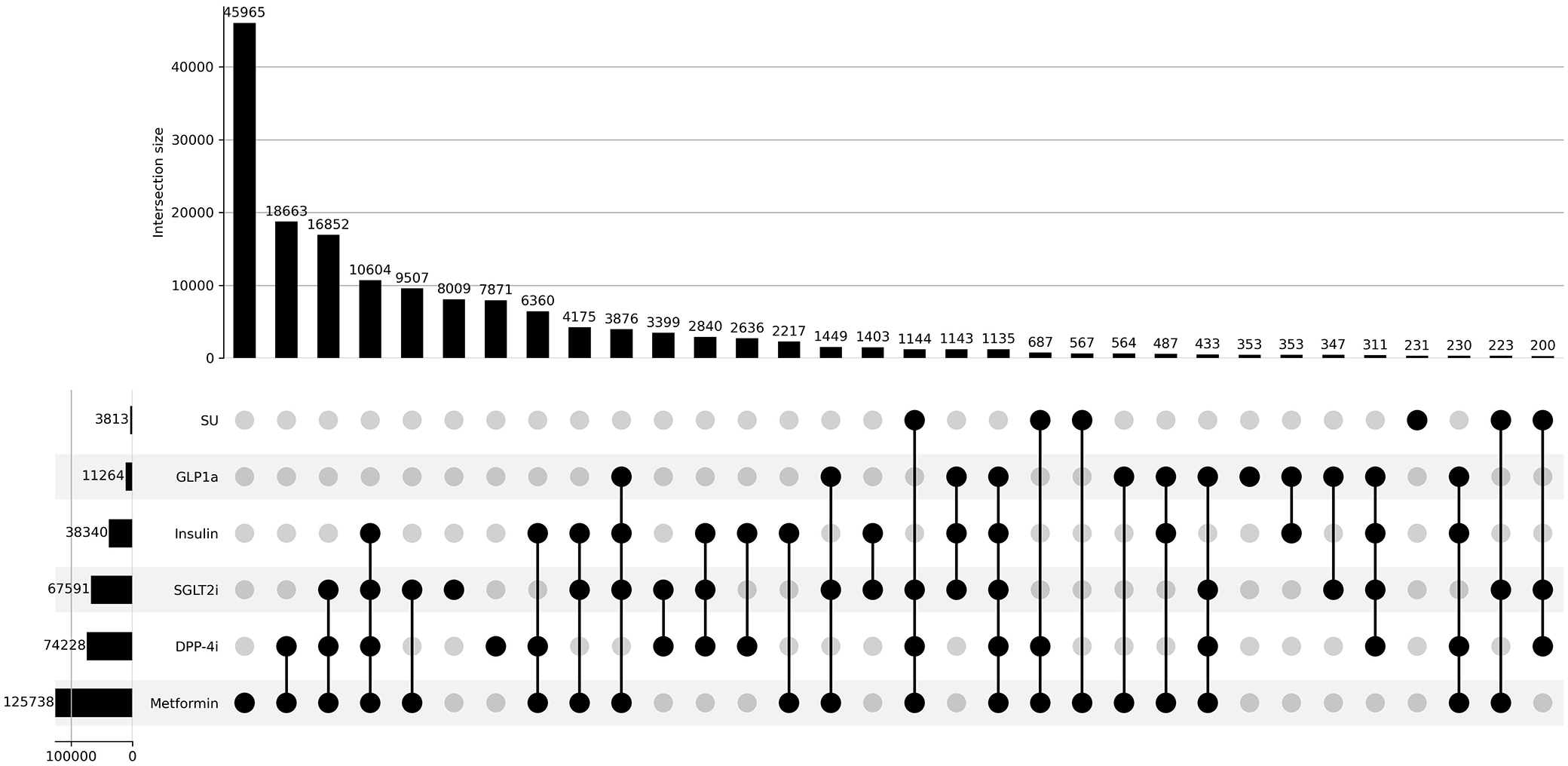
Combinations and antidiabetic treatment schemes most frequently used by a group of 155,381 patients with type 2 diabetes mellitus from Colombia, 2022.
Comedications
Of the population included in the study, 148,936 (95.9%) were receiving concomitant treatment with one or more medications for the most frequent comorbidities that accompany the patient with T2DM. A total of 10,448 patients were taking a single comedication (6.7% of the cases); 14,628 (9.4%) were taking two, 19,689 (12.7%) were taking three, 23,153 (14.9%) were taking four, and 81,018 (52.1%) were taking five or more. The average number of comedications per patient was 4.7 ± 2.6 drugs. The most commonly prescribed medications for this group of patients were antihypertensives, followed by lipid-lowering, nonopioid and anti-inflammatory analgesics, antiulcers, antiplatelet agents, insulins, and thyroid hormone (Table 4).
Medications most frequently used for comorbidities in a group of 155,381 patients diagnosed with diabetes mellitus in Colombia, 2022 (includes different insulins).

Within the group of antihypertensive drugs, the most widely used were angiotensin 2 receptor antagonists, followed by diuretics, calcium channel blockers, and β-blockers, but 71.8% received some inhibitor of the renin–angiotensin–aldosterone system. The most commonly used lipid-lowering drugs were statins (72.7%), and 1.0% were prescribed some drug for the treatment of obesity.
Comparison with study of antidiabetic patterns in Colombia 2015 versus 2022
The proportion of use of any metformin did not change between 2015 and 2022, but the use in combination with noninsulin antidiabetics increased, while its combination with insulins decreased. Marked changes in the DPP-4i, SGLT2i, and GLP1-ra rates were observed, with variable proportions of increased dispensing. The use of sulfonylureas and insulins was reduced at this time (Figure 2).
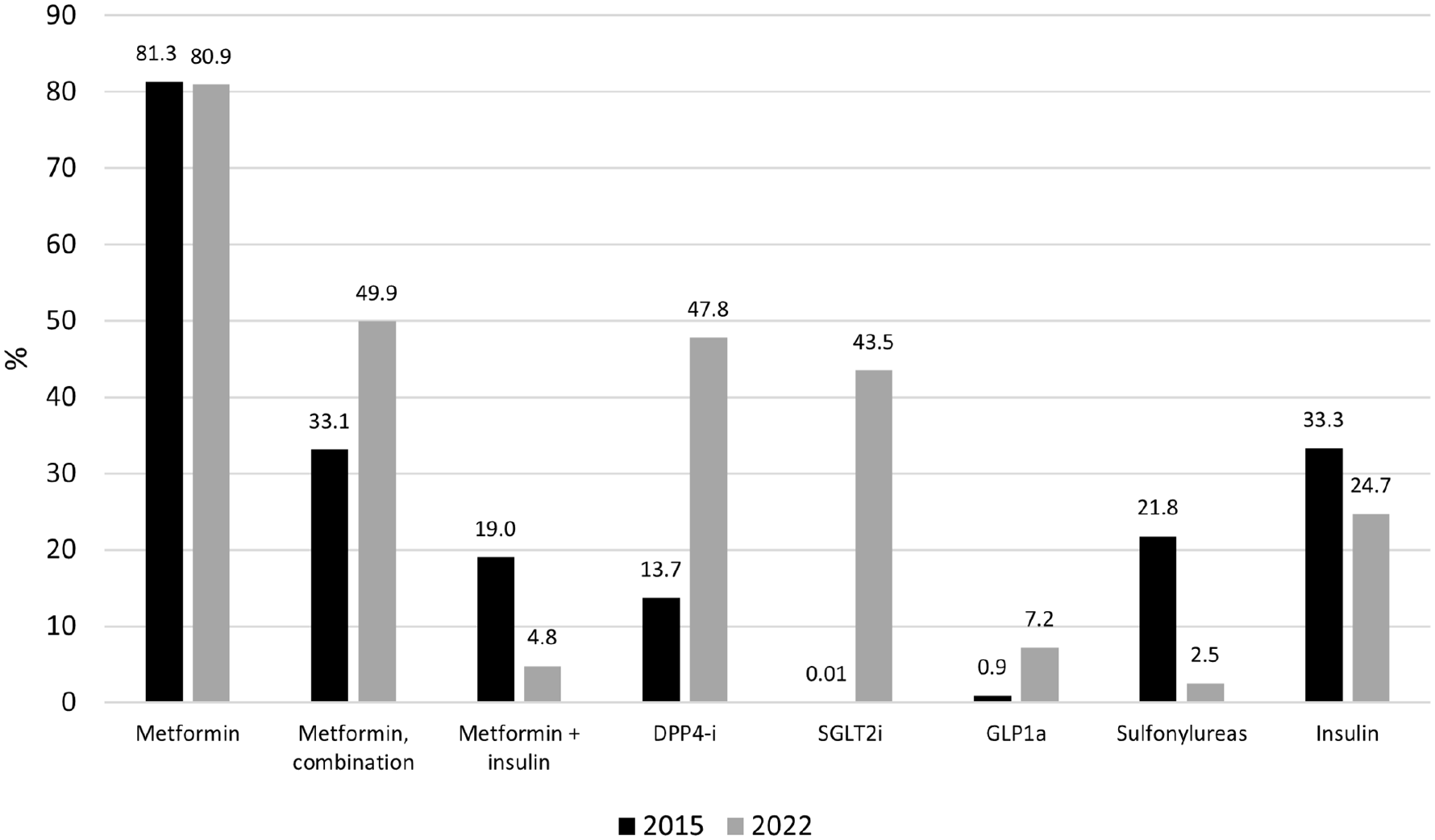
Comparison of the frequency of use of the most used antidiabetics for the treatment of group of 155,381 patients with type 2 diabetes mellitus from Colombia, between 2015 versus 2022.
Discussion
This study identified the prescription patterns of noninsulin antidiabetics in patients with a diagnosis of T2DM affiliated with the Colombian health system. The patterns reflect the changes that have occurred after the introduction of new technologies such as SGLT2is and GLP1-ras, which open prospects for cardiovascular and renal protection in this group of people. These findings may be useful to treating physicians, health administrators, and those who draw up health policies since they collect information on individuals distributed throughout the country affiliated with the contributory and subsidized regimes, who have prescriptions made by general practitioners and specialists.
The mean age identified in this analysis agrees with findings in other countries in terms of mean age (67.1 vs 65.7 years),20,21 though it is lower than reported in patients with T2DM from northern Italy (75.1 years) 22 and greater than that found in Mexico (56.0 years). 23 Our cohort’s proportion of women (59.2%) was similar to the 59.5% reported in the United States 24 but differed from that in Japan (42.5%), 21 Italy (45.1%), 22 and France (46.8%). 20 In addition, the presence of cardiovascular-type comorbidities such as arterial hypertension is similar to reports from Japan (67.6% vs 72.0%), 21 and the rate of chronic kidney disease is similar to that reported in Italy (6.3% vs 7.3%) 22 and Colombia (7.5%), 25 but the rate of heart failure is much lower than that reported in Japan (9.2%) 21 and Italy (11.8%). 24 These similarities and differences can be related to the groups of patients selected in each country, access to health services, and the sociodemographic differences of each study.
Information on the consumption of antidiabetics according to DHD is relevant for making comparisons between countries and at different times. Unfortunately, despite being a recommendation of the World Health Organization, they are not routinely reported by different researchers, and it was not possible to contrast their prescriptions in Colombia with those of other parts of the world. What is clear is that metformin, empagliflozin, and some DPP-4 predominate, as in other countries.21,22,24 The relationship between the mean dose and DDD for most antidiabetics was close to 100%, though in the case of metformin, it fell from 75% to 60% of the recommended dose in recent years in Colombia, 15 which is striking since metformin is still the most widely used drug but at lower doses, which may be related to its gastrointestinal tolerability or to its increasing use in combination with other antidiabetics, which leads the clinician to reduce the concentration to ensure that the patient can tolerate it and take it with adequate adherence. 26
Even the most recent guidelines for the management of T2DM propose starting with changes in lifestyle and, concomitantly, the use of certain antidiabetic drugs in monotherapy according to the presence or absence of atherosclerotic cardiovascular disease, high cardiovascular risk, heart failure, or chronic kidney disease. 5 In this analysis, fewer than half of the patients were prescribed one drug, while the most common number of noninsulin drugs was two, followed by three. The most common combinations were metformin associated with some DPP-4i or SGLT2i, similar to the trends in Japan in the last decade. 27 The high number of drug combinations identified in this group of patients is striking. It may be a reflection of the difficulties that clinicians have in achieving metabolic control in certain cases due to the lack of adherence to the recommendations of the clinical practice guidelines and the diversity of drugs available today for the treatment of T2DM. 28
Though an increasing trend in the use of GLP1-ras and SGLT2is was evident, reflecting the transition toward therapies that offer advantages that go beyond the metabolic control of glucose, such as reducing the risk of cardiovascular events and the progression of renal function deterioration in patients suffering from T2DM, the predominance of DPP-4is is striking, since these offer no advantages in T2DM beyond glucose reduction.5,27,29,30 This may reveal some level of clinical inertia on the part of physicians to prescribe new drugs even if they have shown therapeutic advantages.28,31 In countries such as the United States and Japan, the use of insulin has remained stable over the last few years.24,27 Here, a reduction of insulins from 33.3% in 2015 to 24.7% in 2022 was evident, which may be associated with patient preferences, fear of injecting insulin, and the introduction of new therapeutic groups for oral use. The reduction of the use of sulfonylureas or other antidiabetics such as glitazones, acarbose, and meglitinides has occurred in other countries21,22 and here, which must be associated with the lack of recommendation by the clinical practice guidelines that leave them as last-line options 5 or to the growing evidence of worse cardiovascular outcomes among its users than among those who take GLP1-ras and SGLT2is 32 and the fact that sulfonylureas are associated with weight gain, a situation that must be avoided at present. The current recommendations for adults over 65 years of age, such as the Beers criteria of the American Geriatrics Society, also suggest avoiding these drugs in this population.26,33 However, it should be taken into account that in countries such as France and Mexico, sulfonylureas continue to be used frequently.20,23 It should be taken into account that Resolution 2292 of 2021 of the Ministry of Health of Colombia included all noninsulin antidiabetics (including the new GLP1-ras, SGLT2is) for the treatment of DM, which allows their use in all patients, whose physician will consider it necessary, according to clinical practice guidelines. 34
This work has some limitations related to its observational nature, as the only source of information was data from medical formulas and drug dispensing records. There were no clinical or paraclinical results that would let us identify the degree of control of T2DM in each case and that may have guided the decision of doctors to select the antidiabetic drugs for each of their patients. In addition, this study collected information from people affiliated with a health system, who have their own particular characteristics. This may prevent the extrapolation of the analyses to other contexts. By selecting patients adhering to treatment for 3 months, some who had just started antidiabetic drugs in the last 2 months and who may have had new formulations could have been excluded. Furthermore, given that the clinical records were not verified, it is possible that a proportion of patients receiving metformin alone were using it for diagnoses other than T2DM, such as prediabetes, gestational diabetes, polycystic ovary disease, or even weight loss. A major strength of the study is its real-world evidence of the updated use of antidiabetics in a large number of patients affiliated with a health system that provides all health technologies. Another related strength is related to the fact that the universe of patients with antidiabetic prescriptions was taken and not a sample of them.
Conclusion
Treatment of T2DM in this group of patients from Colombia has undergone important changes in recent years, with the introduction and use of new antidiabetic drugs that offer cardiovascular and renal benefits such as GLP1-ras and SGLT2is, but metformin continues to be the fundamental pillar of the management of most patients, alone or in combination with DPP-4is, SGLT2is, and insulins. In addition, there was a significant reduction in the use of sulfonylureas and insulins, although the proportion of patients treated with combined antidiabetic therapy increased. Given that a significant proportion of the patients analyzed also had arterial hypertension and other cardiovascular risk conditions, it is important to consider the assessment of said risks and the choice of medications aiming at metabolic control but that also offer benefits such as the reduction of cardiovascular events, the main generators of mortality among patients suffering from T2DM.