
Abstract
In this perspective review, we describe a brief background on the status quo of diabetes mellitus-related therapies and glycemic control among patients in rural communities in sub-Saharan Africa. The article discusses insulin therapy as well as the difficulties in obtaining insulin and oral hypoglycemic medications for diabetic patients living in sub-Saharan Africa. We wrap up our discussion with suggestions on solutions and opportunities for future research to tackle this health challenge in these impoverished communities. We conducted a literature search from PubMed and Google Scholar up until August 2023. Key words were used to generate search terms used to retrieve the required information. All types of literature with pertinent information on the current topic were included in the study. Diabetes mellitus is on the rise in sub-Saharan Africa. Several studies have reported poor glycemic control, low screening rates for diabetes mellitus, cigarette smoking, high alcohol consumption, prescription of antidiabetic therapy, and associated costs as contributors to the uptake of antidiabetic treatment. Although there is paucity of data on the extent of insulin therapy uptake and its possible modifiable contributors among the diabetic patients in the region, the anticipated increase in the number of people with diabetes on the continent makes it critical for global leaders to address the research gaps in insulin therapy among rural communities of sub-Saharan Africa, thus reducing the burden of diabetes in these populations.
Keywords
Introduction
The prevalence and burden of insulin resistance varies greatly among different countries and regions of sub-Saharan Africa (Figure 1), making the current situation on the continent complicated. Despite the significance of diabetes on world health, the future economic effects of the condition are still unknown. 1 In sub-Saharan Africa, improvements in the therapeutic management of type 2 diabetes and related glycemic control are still far from ideal. 2

Map showing Sub-Saharan Africa (in green) according to the United Nations By Jcherlet: Jcherlet / derivative work: Jcherlet (talk) – HDImap_spectrum2006_Africa.png, Public Domain, https://commons.wikimedia.org/w/index.php?curid=12340966.
Diabetes mellitus is a growing public health concern in sub-Saharan Africa, with the prevalence of the disease increasing rapidly over the past few decades. Diabetes facts and figures show that there is a growing global burden for individuals, families, and countries. The International Diabetes Federation (IDF) Diabetes Atlas (2021) reports that 10.5% of the adult population (20–79 years) has diabetes, with almost half unaware that they are living with the condition. By 2045, IDF projects that 1 in 8 adults, approximately 783 million, will be living with diabetes, an increase of 46%. 3 It was also reported that there were approximately 19.4 million people with diabetes in sub-Saharan Africa in 2019, and this number is projected to increase to 47.1 million by 2045. 4
Over 90% of cases of diabetes in sub-Saharan Africa are type 2, making it the most prevalent kind of the disease. 5 Changing food habits, physical inactivity, increasing urbanization, and genetic susceptibility are among the risk factors for diabetes globally and sub-Saharan Africa is no exception. 6 World over, including sub-Saharan Africa, diabetes is often undiagnosed and poorly managed due to a lack of awareness, inadequate healthcare infrastructure, and limited access to affordable diabetes care and medications .5,7,8 The global diabetic population suffers associated complications such as cardiovascular disease, kidney disease, and blindness, which are also a major occurrence among the diabetic patients in sub-Saharan Africa whose healthcare systems are in a dilapidated state.9,10 However, efforts are being made to address the rising burden of diabetes in sub-Saharan Africa, including improved screening and diagnosis, increased availability of affordable diabetes care and medications, and public health campaigns to raise awareness and promote healthy lifestyles.11,12
Methods
We conducted an extensive search of published literature from PubMed and Google Scholar. The search was done using the key words of ‘insulin therapy’, ‘oral hypoglycemic’, glycemic control, ‘anti- diabetic drugs’, ‘sub Saharan Africa’, ‘diabetes mellitus’. Several articles were retrieved; however, only articles with pertinent information were included in the review. Selected primary studies with relevant findings were summarized in Table 1.
Overview of the review of some retrieved studies.
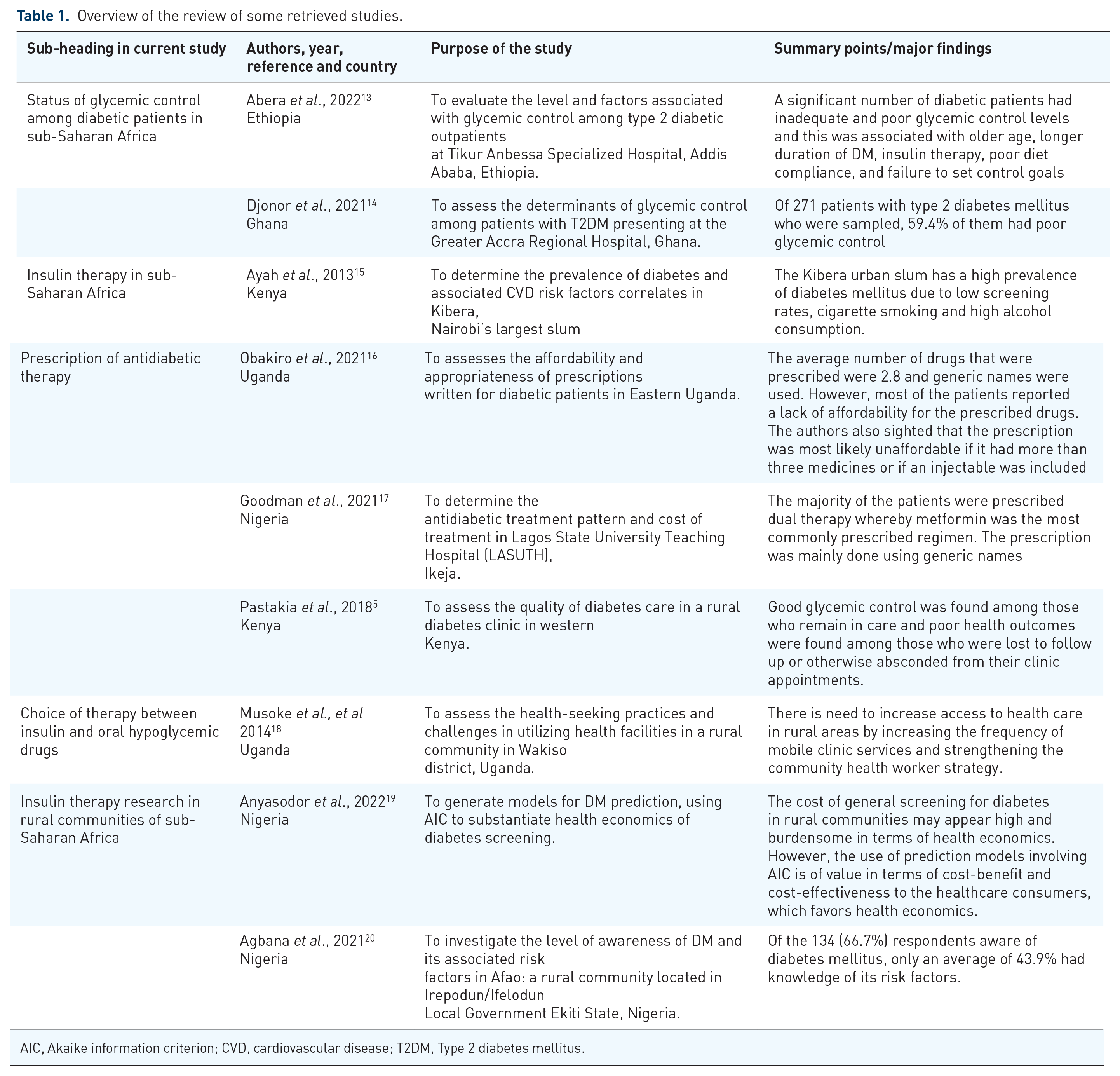
AIC, Akaike information criterion; CVD, cardiovascular disease; T2DM, Type 2 diabetes mellitus.
Review
Status of glycemic control among diabetic patients in sub-Saharan Africa
The status of glycemic control among diabetic patients in sub-Saharan Africa is generally poor. There are several reasons for this, including limited access to healthcare, a lack of diabetes education and awareness, and the high cost of diabetes care and medications. According to research studies, many diabetics in sub-Saharan Africa have inadequate control of their glucose levels, which puts them at higher risk for consequences like heart disease, kidney damage, and blindness.21,22 A study conducted in Ethiopia found that a significant number of diabetic patients had inadequate and poor glycemic control levels and this was associated with older age, longer duration of DM, insulin therapy, poor diet compliance, and failure to set control goals. 13 Another study conducted in Ghana found that only 59.4% of people with diabetes had poor glycemic control. 14 There are several challenges to achieving good glycemic control in sub-Saharan Africa. These include a lack of access to insulin and other diabetes medications, poor adherence to treatment due to cultural and economic factors, and inadequate healthcare infrastructure.21,23 Efforts are being made to improve glycemic control among diabetic patients in sub-Saharan Africa, including the development of locally appropriate guidelines and protocols for diabetes care, training of healthcare professionals, and the establishment of diabetes clinics and education programs. However, there is still a long way to go to ensure that all people with diabetes in sub-Saharan Africa have access to the care and support they need to achieve good glycemic control and prevent complications.
Insulin therapy in sub-Saharan Africa
The proportion of diabetic patients who are on insulin therapy can vary depending on several factors, including the type of diabetes, the stage of the disease, and the availability and accessibility of insulin and other diabetes medications. In general, insulin therapy is more commonly used in patients with type 1 diabetes, as this form of diabetes is characterized by a lack of insulin production by the pancreas.24–27 In contrast, patients with type 2 diabetes may initially be treated with lifestyle modifications and oral hypoglycemic agents, with insulin therapy reserved for those who do not achieve adequate glucose control with these interventions.28–31 In rural communities of sub-Saharan Africa, the prevalence of diabetes and the proportion of patients on insulin therapy can vary widely depending on the specific location and healthcare resources available. For example, a study conducted in a Kenyan slum area found a high prevalence of diabetes mellitus which was attributed to low screening rates, cigarette smoking and high alcohol consumption; however, the uptake of insulin therapy is not known amongst these study populations.5,15,32,33 In some areas, access to insulin and other diabetes medications may be limited, resulting in a lower proportion of patients on insulin therapy.34,35 In other areas, insulin therapy may be more widely used, particularly in patients with type 1 diabetes or advanced type 2 diabetes. 6 It is important to note that diabetes is a growing public health concern in sub-Saharan Africa. With increasing rates of the disease and its complications, rural-to-urban migration in the region has been noted to significantly increase the geographical spread of people with diabetes. 33 Efforts to improve access to diabetes care, including insulin therapy, are needed to address this growing burden of disease.
Prescription of antidiabetic therapy
Patients with diabetes mellitus, a chronic metabolic condition marked by elevated circulating blood sugar levels, are typically recommended insulin therapy.36,37 Insulin is a hormone that helps regulate blood glucose levels by promoting the uptake of glucose into cells and tissues, and the synthesis and storage of glycogen in the liver and muscles.38,39 Patients with diabetes mellitus may require insulin therapy if their body is unable to produce enough insulin or if their cells are resistant to insulin, resulting in elevated blood glucose levels.39,40 Diabetes mellitus can be of two major types: Diabetes type 1: This autoimmune illness causes the beta cells in the pancreas that create insulin to be assaulted and eliminated by the body’s immune system.41–43 Type 1 diabetes typically develops in childhood or adolescence and requires lifelong insulin therapy.25,26 Type 2 diabetes: This is a metabolic disorder characterized by insulin resistance and impaired insulin secretion.30,31,44 Obesity and a sedentary lifestyle are frequently linked to type 2 diabetes and is typically managed initially with lifestyle modifications and oral medications.30,45 However, some patients with type 2 diabetes may eventually require insulin therapy as the disease progresses. In addition to patients with diabetes, insulin therapy may also be prescribed to patients with other medical conditions that affect glucose metabolism, such as gestational diabetes, cystic fibrosis-related diabetes, and steroid-induced diabetes.46–48
Oral hypoglycemic drugs are medications that are used to treat diabetes mellitus by lowering blood glucose levels.49–52 Unlike insulin therapy, which is delivered via injections or an insulin pump, oral hypoglycemic drugs are taken orally in pill form.53–55 The choice of oral hypoglycemic medication depends on several factors, including the type of diabetes, the severity of the disease, and the presence of other medical conditions.50,51,56 In some cases, oral hypoglycemic drugs may be used in combination with insulin therapy to achieve optimal blood glucose control.57,58
In sub-Saharan Africa, the patterns and trends of prescription have been carried out among different diabetic patients in selected countries. The findings are surprisingly similar despite the difference in the organization of the healthcare systems in these countries. A study conducted in Mbale, Uganda, assessed the irrational prescription of antidiabetic therapy and found that the average number of drugs that were prescribed were 2.8 and generic names were used. However, most of the patients reported a lack of affordability for the prescribed drugs. The authors also sighted that the prescription was most likely unaffordable if it had more than three medicines or if an injectable was included. 16 Another similar study conducted in Lagos, Nigeria assessed the antidiabetic treatment pattern and its cost effectiveness found that majority of the patients were prescribed dual therapy whereby metformin was the most commonly prescribed regimen. The prescription was mainly done using generic names. 17 The similarity in these two study sheds light on how the diabetic drugs are being utilized in the recent times.
Due to the limited availability and high cost of oral hypoglycemic medications in rural communities across sub-Saharan Africa, insulin therapy is frequently favored as a treatment for diabetes.22,33,59,60 While oral hypoglycemics can be effective in managing diabetes, they may not be as readily available or accessible as insulin therapy in many rural areas.58,61,62 Furthermore, insulin therapy may be a more practical option for patients who do not have access to refrigeration or reliable electricity, which may be necessary to store and administer some oral hypoglycemic medications.63–65 However, it is worth noting that the availability and use of insulin therapy in rural communities of sub-Saharan Africa is also limited by several factors, including the high cost of insulin, the need for regular monitoring of blood glucose levels, and the lack of trained healthcare providers who can administer and manage insulin therapy.10,66 A study conducted in a Kenyan rural community found that good glycemic control was consistent with those diabetic patients who remained in care implying eased access to diabetic medication and poor health outcomes were found among those who were lost to follow-up or otherwise absconded from their clinic appointments. 5 Overall, the choice of therapy for diabetes in rural communities of sub-Saharan Africa may depend on a range of factors, including the availability of medications, the infrastructure for healthcare delivery, and the preferences and needs of individual patients.
Choice of antidiabetic therapy
The choice of therapy for diabetes, whether insulin or oral hypoglycemic drugs, is determined by a healthcare provider in consultation with the patient.50,67,68 Healthcare providers, such as doctors, nurses, or clinical officers, are trained to diagnose and manage diabetes, and they will typically evaluate a patient’s medical history, symptoms, and laboratory results to determine the most appropriate course of treatment.69,70 Factors that may influence the choice of therapy include the type and severity of diabetes, the patient’s overall health status, their access to healthcare and medications, and their preferences and lifestyle.56,71,72 In rural communities of sub-Saharan Africa, where resources and infrastructure may be limited, healthcare providers may need to consider additional factors, such as the availability and cost of medications, and the practicalities of administering and monitoring treatment.18,73–75 A study conducted in rural Uganda emphasized that there is a need to increase access to health care in rural areas by increasing the frequency of mobile clinic services and strengthening the community health worker strategy. 18 Ultimately, the choice of therapy for diabetes should be a shared decision between the healthcare provider and the patient, taking into account the best available evidence and the individual needs and circumstances of the patient.
Hypoglycemia, which is defined as a blood glucose level below 70 mg/dL (3.9 mmol/L), is a common complication of insulin therapy. 76 The kind and dosage of insulin, the timing and frequency of insulin injections, the patient’s general health status, and adherence to treatment are all factors that affect the risk of hypoglycemia. Studies have shown that depending on the population being investigated and the techniques employed to measure hypoglycemia, the frequency of hypoglycemia varies significantly.26,68,77,78 For instance, a review of studies involving individuals who had type 1 diabetes revealed that minor to moderate low blood sugar (requiring self-treatment) occurred in 18–138 episodes per patient-year while severe low blood sugar (requiring assistance from another person) occurred in 0.05–2.4 episodes per patient-year.79,80 Similarly, studies of patients with type 2 diabetes found that the incidence of hypoglycemia varied depending on the type of insulin used, with a higher risk observed among those using long-acting basal insulin compared to those using short-acting insulin.81–85 It is important to note that hypoglycemia can be a serious and potentially life-threatening complication of insulin therapy, and patients on insulin should be educated about the signs and symptoms of hypoglycemia and how to treat it promptly if it occurs.76,86,87 Regular monitoring of blood glucose levels and close communication with a healthcare provider can also help to minimize the risk of hypoglycemia and ensure optimal diabetes management.
Hyperglycemia, which is defined as a blood glucose level above the target range and can occur in people on insulin therapy if the dose of insulin is not adequate or if there are other factors affecting insulin sensitivity, such as illness or stress.70,88 The frequency of hyperglycemia among people on insulin therapy can vary depending on several factors, including the type and dose of insulin, the timing and frequency of insulin injections, and the patient’s overall health status and adherence to treatment.89–91 According to research, the risk of hyperglycemia persists even after insulin therapy is able to successfully lower blood glucose levels in persons with diabetes. For example, a study of people with type 1 diabetes reported that 38.2% of people with a HbA1c level of 7.0% or higher and 11.2% of people with a HbA1c level of less than 7.0% experienced hyperglycemia, which is characterized as a level of blood sugar above 180 mg/dL or 10 mmol/L.92–96 Similarly, a study of patients with type 2 diabetes found that 44% of patients receiving basal insulin therapy and 52% of patients receiving basal-bolus insulin therapy experienced hyperglycemia, which is defined as blood glucose levels above 130 mg/dL or 7.2 mmol/L. 97 It is important for patients on insulin therapy to regularly monitor their blood glucose levels and work with their healthcare provider to adjust their insulin dose as needed to keep the blood sugar level under control and reduce the possibility of having elevated sugar levels.
Management of diabetic individuals using insulin therapy
In the treatment of people with diabetes on insulin treatment, measurement of glucagon levels is not frequently performed.98,99 However, glucagon plays an important role in glucose homeostasis, and understanding the interaction between insulin and glucagon can be useful in managing diabetes, particularly in patients on insulin therapy. 100 Insulin and glucagon have opposite effects on blood glucose levels, with insulin promoting glucose uptake and storage, while glucagon promotes the release of glucose from the liver. 101 In patients with diabetes, the balance between insulin and glucagon is disrupted, leading to hyperglycemia. In patients on insulin therapy, glucagon levels can impact glucose control, as high levels of glucagon can counteract the effects of insulin and lead to elevated blood glucose levels.70,102,103 While glucagon levels are not routinely assessed in the management of diabetes, healthcare providers may consider measuring glucagon levels in certain situations, such as in the context of research studies or when there is suspicion of glucagonoma, a rare tumor that produces excessive amounts of glucagon and can lead to severe hyperglycemia.104,105 In general, the management of diabetes on insulin therapy focuses on monitoring blood glucose levels and adjusting insulin doses as needed to achieve optimal glucose control. 106 Regular follow-up with healthcare providers is important to assess treatment effectiveness and adjust treatment plans as needed.
The assessment of glucagon levels is not a common practice in the routine management of diabetes in rural communities of sub-Saharan Africa.107,108 Glucagon is a hormone produced by the pancreas that plays an important role in regulating blood glucose levels by promoting the release of stored glucose from the liver. 100 While glucagon levels can be measured through blood tests, this is typically done in a research or clinical setting, and not as part of routine diabetes management.98,106 The assessment and monitoring of blood glucose levels, as well as other measurements like HbA1c, which shows whether or not long-term glucose control has been achieved, are often the main priorities in the handling of diabetes.70,76 Insulin therapy and/or oral hypoglycemic agents are typically used to lower blood glucose levels, while dietary and lifestyle modifications are also important in the management of diabetes.50,64 It is significant to remember that medical amenities are not readily available, including laboratory testing and medical supplies. These can be limited in rural communities of sub-Saharan Africa, which may impact the ability to perform certain tests or provide certain treatments.71,109,110,111 As such, healthcare providers in these settings may need to prioritize the most essential components of diabetes management based on available resources and the specific needs of individual patients.
Diabetes research in rural communities
Diabetes research in rural communities of sub-Saharan Africa has been ongoing for several years. Some of the key areas of research include: access to insulin which is one of the major challenges faced by rural communities in sub-Saharan Africa.6,14,107,112 Research has been conducted to determine the availability of insulin in rural areas and to identify barriers to its access. This has led to the development of strategies to improve access to insulin, such as training healthcare workers to provide insulin therapy and establishing distribution networks to deliver insulin to rural areas.112–114 Studies have also examined the number of cases with diabetes in rural areas and the efficiency of various treatment options.19,112,115–117 A study in the Ndokwa communities of Delta State in Nigeria was looking for models to screen and predict diabetes outcomes as a way of mitigating the cost implications associated with the disease. 118 This type of research involves conducting surveys and clinical trials to assess the impact of various interventions, such as lifestyle modifications, medication adherence programs, and community-based care models. 19 Research has also looked at the cost-effectiveness of insulin therapy in rural communities.20,118,119 This has involved evaluating the cost of insulin therapy and its impact on patient outcomes, as well as assessing the feasibility of scaling up insulin therapy in resource-limited settings. Another area of research has been focused on increasing education and awareness about diabetes and insulin therapy in rural communities .65,120–123 A study conducted in a rural community located in Irepodun/Ifelodun, Ekiti State in southwestern Nigeria found that of the 134 (66.7%) respondents aware of diabetes mellitus, only an average of 43.9% had knowledge of its risk factors. 120 This finding is an indication of the dire need for an improved level of awareness about diabetes and its associated factors especially in the rural communities of sub-Saharan Africa. Strategies should consider developing culturally appropriate educational materials and working with community health workers to deliver diabetes education and support. Overall, insulin research in rural communities of sub-Saharan Africa is aimed at improving access to insulin therapy, reducing the burden of diabetes, and improving patient outcomes.
Research gaps
Despite the progress made in insulin research in rural communities of sub-Saharan Africa, there are still several research gaps that need to be addressed. Some of the key research gaps include: Limited data on insulin access: while there have been efforts to improve access to insulin in rural areas, there is still limited data on the availability and accessibility of insulin. 61 More research is needed to assess the current state of insulin access in rural communities and to identify strategies for improving access. Limited understanding of patient perspectives: research has primarily focused on healthcare provider perspectives, with limited understanding of patient perspectives on insulin therapy.68,124–127 More research is needed to understand patient experiences with insulin therapy, including barriers to adherence and strategies for improving treatment outcomes. Limited data on long-term outcomes: while there have been studies assessing the short-term impact of insulin therapy on patient outcomes, there is a lack of data on long-term outcomes, such as mortality rates and quality of life.128,129 More research is needed to assess the long-term impact of insulin therapy on patient outcomes in rural communities. Limited research on alternative insulin delivery methods: while insulin injections are the most common method of insulin delivery, there is a need for research on alternative insulin delivery methods that may be more feasible or acceptable in rural communities, such as insulin patches or inhalers.54,130 Limited research on comorbidities: diabetes often coexists with other conditions, such as hypertension and cardiovascular disease. 131 Additional research is required to comprehend the way pathologies affect insulin therapy as well as to develop integrated treatment modalities that simultaneously tackle many illnesses.
Limitations
We were unable to retrieve sufficient information to discuss the specific regional challenges in regards to antidiabetic drugs use as well as the prescription of these drugs in the different countries of sub-Saharan Africa. These were considered as areas with scanty literature and therefore recommended for further investigation using other research strategies.
Conclusion
Although there is paucity of data on the extent of insulin therapy uptake and its possible modifiable contributors among the diabetic patients in the region, the anticipated increase in the number of people with diabetes on the continent makes it critical for global leaders to address the research gaps in insulin therapy among rural communities of sub-Saharan Africa, thus reducing the burden of diabetes in these populations. This review has also identified the need for primary studies on the continent that seek to identify the prescription patterns of antidiabetic therapies.