
Abstract
Objective:
To assess the in-hospital mortality from acute stroke and its predictors in sub-Saharan Africa.
Method:
The literature search was conducted in the databases of PubMed/Medline, Embase, CINAHL, and Google Scholar. The retrieved studies were screened by titles and abstracts, and then full texts were assessed for eligibility. The methodological quality of the included studies was assessed using the Joanna Briggs Institute’s critical appraisal checklist. The publication bias was assessed using the funnel plot asymmetry and the Egger tests. Data were analyzed using Stata software version 15.0 in a random-effect model.
Result:
A total of 27 studies with a total sample size of 6331 were included in this systematic review and meta-analysis. The pooled estimated prevalence of in-hospital mortality due to stroke was 22% (95% confidence interval = 0.17–0.27). Stroke mortality in Western Africa (37%, 95% confidence interval = 0.24–0.50) was higher than in Eastern Africa (15%, 95% confidence interval = 0.12–0.19) and Southern Africa (18%, 95% confidence interval = 0.06–0.19). In three studies, mortality was higher in hemorrhagic stroke (25%) than ischemic stroke (14%). Risk factors associated with higher mortality were admission Glasgow Coma Scale, stroke severity, age, sex, presence of hypertension, and declined renal function.
Conclusion:
The in-patient mortality of stroke in sub-Saharan Africa was high. Therefore, there is an urgent need for further stroke epidemiology studies in stroke subtypes and the performance of patient-level meta-analysis to understand the risk factors associated with mortality and herald appropriate intervention to curb the high mortality rate in the region.
Introduction
Stroke is an acute medical condition that is characterized by sudden weakness or numbness of the face, arm, or leg, most often on one side of the body. 1 It results from an inadequate supply of oxygen and nutrients to the brain due to a disruption of cerebral perfusion. It is the brain equivalent of a heart attack. 2
Stroke is one of the leading causes of morbidity and mortality worldwide.3,4 According to the recent reports of the Global Burden of Disease study, cerebrovascular diseases ranked the second leading cause of death after ischemic heart disease. 5 Although the incidence in developed countries has shown a 42% reduction, the incidence in low-income countries has shown a 100% increase. 6 Globally, an estimated 16.8 million people were diagnosed with stroke per annum. 7
In sub-Saharan Africa, the incidence of stroke has risen substantially over the last 20 years. Like other non-communicable diseases, currently, it is the prominent cause of death, disability, and dementia in this region.8,9 The healthcare system in sub-Saharan Africa mainly focuses on infectious diseases. Thus, there is a lack of resources to prevent or treat non-communicable diseases, including stroke. In this region, stroke treatment is inadequate in clinical practice.8,10 Several studies were conducted to evaluate the in-hospital mortality rate from acute stroke in sub-Saharan Africa.11–37 However, the mortality rate has not been summarized to reflect the overall in-hospital mortality rate in the region. Hence, this systematic review and meta-analysis aimed to obtain more robust evidence on stroke treatment outcomes from the existing literature in sub-Saharan Africa countries.
Methods
Protocol and reporting
The protocol was registered in Prospero with a registration number CRD42020169770. The systematic review and meta-analysis were reported in line with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guideline.
Search strategies
The Cochrane guidelines and the PRISMA statement were used to conduct a systematic computerized search of the PubMed, Google Scholar, CINAHL, Embase, and Medline databases. The literature search was performed using keywords related to stroke in-hospital outcome in sub-Saharan Africa (Stroke (MeSH) OR “cardiac ischemia” OR “intracranial haemorrhage” OR “hemiplegia” OR “quadriplegia” AND in-hospital outcome (MeSH)) AND sub-Saharan Africa (“Angola,” “Benin,” “Botswana,” “Burkina Faso,” “Burundi,” “Cameroon,” “Cape Verde,” “Central African Republic,” “Chad,” “Comoros,” “Congo,” “Côte d’Ivoire,” “Djibouti,” “Equatorial Guinea,” “Eritrea,” “Ethiopia,” “Gabon,” “Gambia,” “Ghana,” “Guinea,” “Guinea-Bissau,” “Kenya,” “Lesotho,” “Liberia,” “Madagascar,” “Malawi,” “Mali,” “Mauritania,” “Mozambique,” “Namibia,” “Niger,” “Nigeria,” “Rwanda,” “Sao Tome and Principe,” “Senegal,” “Sierra Leone,” “Somalia,” “South Africa,” “Sudan,” “Swaziland,” “Tanzania,” “Togo,” “Uganda,” “Zambia,” and “Zimbabwe”). In addition, we searched the reference lists the included studies using snowball technique. Both observational (prospective and retrospective) and interventional studies were included in the review and meta-analysis. The publication date of studies was not used to determine the study’s eligibility. Any studies published before 20 November 2020 were included in the study.
Eligibility
Inclusion and exclusion criteria
Original articles published in the English language that examined stroke treatment outcomes in sub-Saharan Africa were included in the systematic review and meta-analysis. Furthermore, qualitative studies and studies without full text were excluded.
Screening and quality assessment
The studies retrieved during the searches were screened initially by titles and abstracts. Then, the full text was assessed for eligibility. The quality assessment was performed using the Joanna Briggs Institute (JBI)’s critical appraisal checklist for cohort and analytical cross-sectional studies.38,39 The methodological quality assessment was done independently by two reviewers (A.S.M. and A.D.). The mean scores of two authors were considered in coming to a final decision regarding study quality. Any discrepancies were resolved through a discussion with other co-authors. Finally, studies were ranked by their methodological qualities based on the total number of appraisers’ scores marked as “yes” to questions of the JBI’s critical appraisal checklist. Accordingly, we included all studies with the overall positive responses of 50%–75% (moderate-quality studies) or higher than 75% (high-quality studies) in the systematic review and meta-analysis.
Data extraction
The authors extracted important data related to the study characteristics (the region and the study area, the first author, the year of publication, the study design, the population characteristics, and the sample size) and the outcomes of interest (the effect size data, including the in-hospital stroke outcome, and the predictors of poor in-hospital outcome).
Risk of bias assessment
The presence of publication bias was assessed using the Begg and Mazumdar rank correlation test and the Egger regression test and presented using the funnel plots.
Data analysis
Stata software version 15.0 was used to analyze the pooled estimates of primary and secondary outcomes and as well as the subgroup analysis. Considering the variation in true effect size across the studies, DerSimonian and Laird’s random-effects model was applied for the analysis, with a 95% confidence level (CI). Due to the heterogeneity among the included studies in reporting the factors associated with in-hospital outcomes, we could not analyze the pooled estimate of predictors. Sub-group analysis was conducted by the regions of the continent (Eastern, Western, Northern, and Southern Africa).
Results
Search findings
A total of 1728 records were identified from the search of databases and indexing services. Accordingly, 165 studies were retrieved in PubMed, 388 studies were retrieved in Medline, 390 studies were retrieved in Embase, 85 studies were retrieved in CINAHL, and 700 were retrieved in Google Scholar databases. Four hundred and thirty-one duplicates were removed, and 1297 articles were screened by titles and abstracts. From this, 1241 articles were excluded, and the retained 56 full-text articles were assessed for eligibility. Out of this, 29 articles were excluded with reasons, and 27 studies were included for the final analysis (Figure 1). Besides, the methodological quality of the included studies was assessed by employing the JBI’s critical appraisal checklist (Table 1).
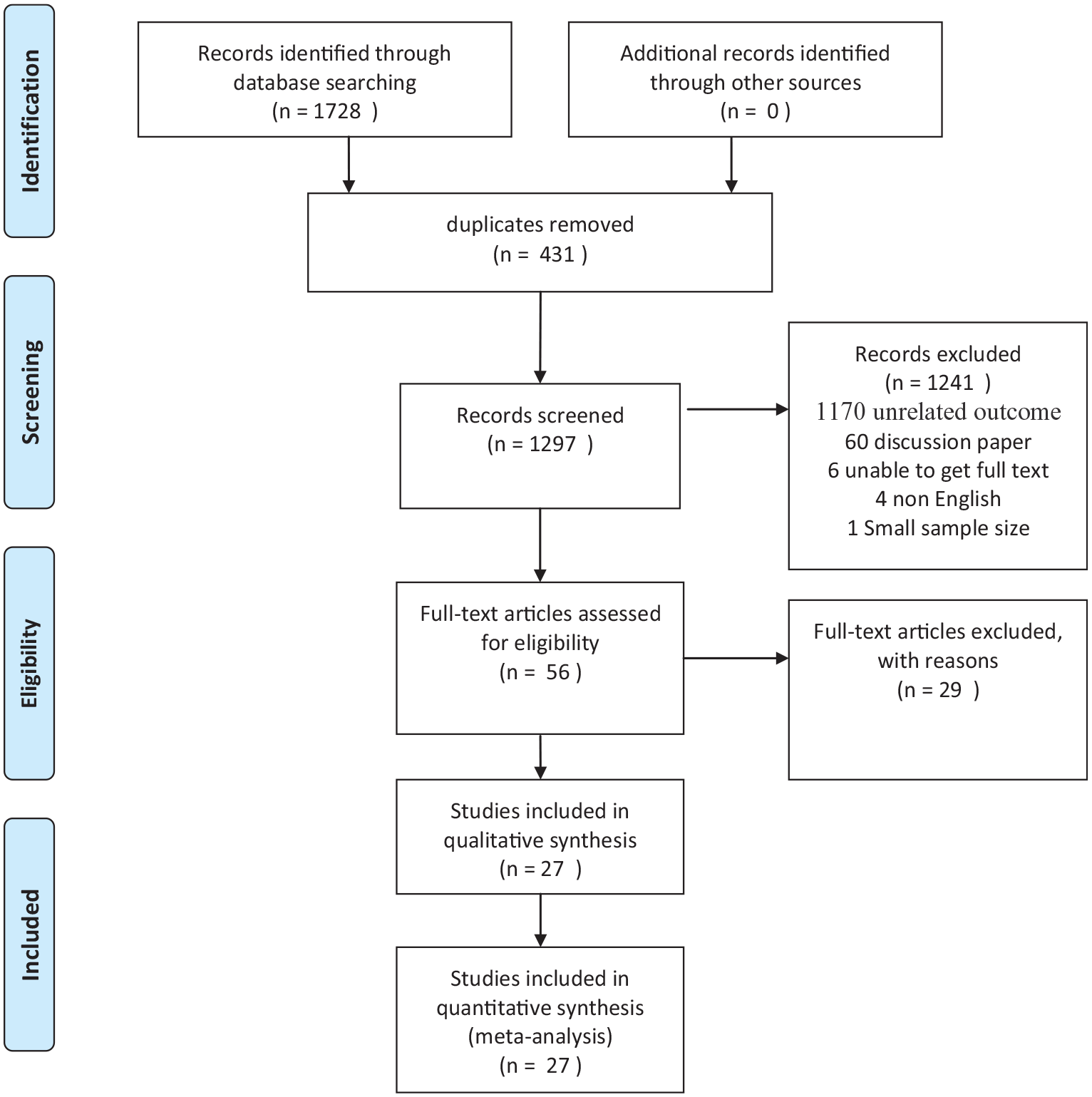
PRISMA flow diagram of article searching.
Quality assessment of the included studies.

NA: not applicable.
JBI’s critical appraisal checklist for analytical cross-sectional studies (Q1: were the criteria for inclusion in the sample clearly defined? Q2: were the study subjects and the setting described in detail? Q3: was the exposure measured in a valid and reliable way? Q4: were objective, standard criteria used for measurement of the condition? Q5: were confounding factors identified? Q6: were strategies to deal with confounding factors stated? Q7: were the outcomes measured in a valid and reliable way? Q8: was appropriate statistical analysis used?); Q1–11, JBI’s critical appraisal checklist for cohort studies (Q1: were the two groups similar and recruited from the same population? Q2: were the exposures measured similarly to assign people to both exposed and unexposed groups? Q3: was the exposure measured in a valid and reliable way? Q4: were confounding factors identified? Q5: were strategies to deal with confounding factors stated? Q6: were the groups/participants free of the outcome at the start of the study (or at the moment of exposure)? Q7: were the outcomes measured in a valid and reliable way? Q8: was the follow-up time reported and sufficient to be long enough for outcomes to occur? Q9: was follow-up complete, and if not, were the reasons to loss to follow-up described and explored? Q10: were strategies to address incomplete follow-up utilized? Q11: was appropriate statistical analysis used?).
Study characteristics
The 27 studies included for the systematic review and meta-analysis had 6331 participants. Out of these, 2499 patients had an ischemic stroke, while 1884 patients had a hemorrhagic stroke. Of the total included studies, four reported a higher rate of hemorrhagic stroke.11,21,24,34 The sample size of the included studies was ranged from 36 to 1054.13,36 Of the total studies, most of them (15 studies) were conducted in Eastern Africa15,16,19,20,22–24,26–29,31,32,34,37 and eight of them were in Western Africa 12 –14,21,30,33,35,36 and the remaining four studies were conducted in Southern Africa11,17,18,25 (Table 2).
Characteristics of in-hospital mortality among stroke patients in sub-Saharan Africa.

CS: cross-sectional; RFU: retrospective follow-up; FU: prospective follow-up; NR: not reported.
Prevalence of in-hospital mortality among stroke patients
The pooled estimated prevalence of in-hospital mortality from acute stroke in sub-Saharan Africa was 22% (pooled proportion (PP) = 0.22, 95% CI = 0.17–0.27; I 2 = 96.4%, p ⩽ 0.001). The mortality rate was ranged from 5% (95% CI = 0.02–0.12) to 78% (95% CI = 0.62–0.88) (Figure 2).

Forest plot of the pooled prevalence of in-hospital mortality among stroke patients in sub-Saharan Africa.
Sensitivity and subgroup analyses
In this meta-analysis, we performed sensitivity analyses by excluding outliers.33,36 Hence, the analysis showed that they did not significantly change the extent of pooled outcome measures and heterogeneity (PP = 0.21, 95% CI = 0.17–0.26, I 2 = 96.16%). As a result, we included all the studies for the meta-analysis. A subgroup analysis by the regions of sub-Saharan Africa showed that the pooled estimate of in-hospital mortality in Western Africa (PP = 0.37, 95% CI = 0.24–0.50) was higher as compared to the mortality rate in Eastern (PP = 0.15, 95% CI = 0.12–0.19) and Southern Africa (PP = 0.18, 95% CI = 0.06–0.19) (Figure 3).

Forest plot describing in-hospital mortality by regions of sub-Saharan Africa.
The present meta-analysis showed that the pooled estimate of in-hospital mortality for hemorrhagic stroke was 25% (95% CI = 0.07–0.42), while the pooled estimate of in-hospital mortality for ischemic stroke was 14% (95% CI = 0.10–0.18) (Figure 4). However, out of the 27 studies, only two and three studies reported the mortality rates of ischemic and hemorrhagic strokes, respectively.
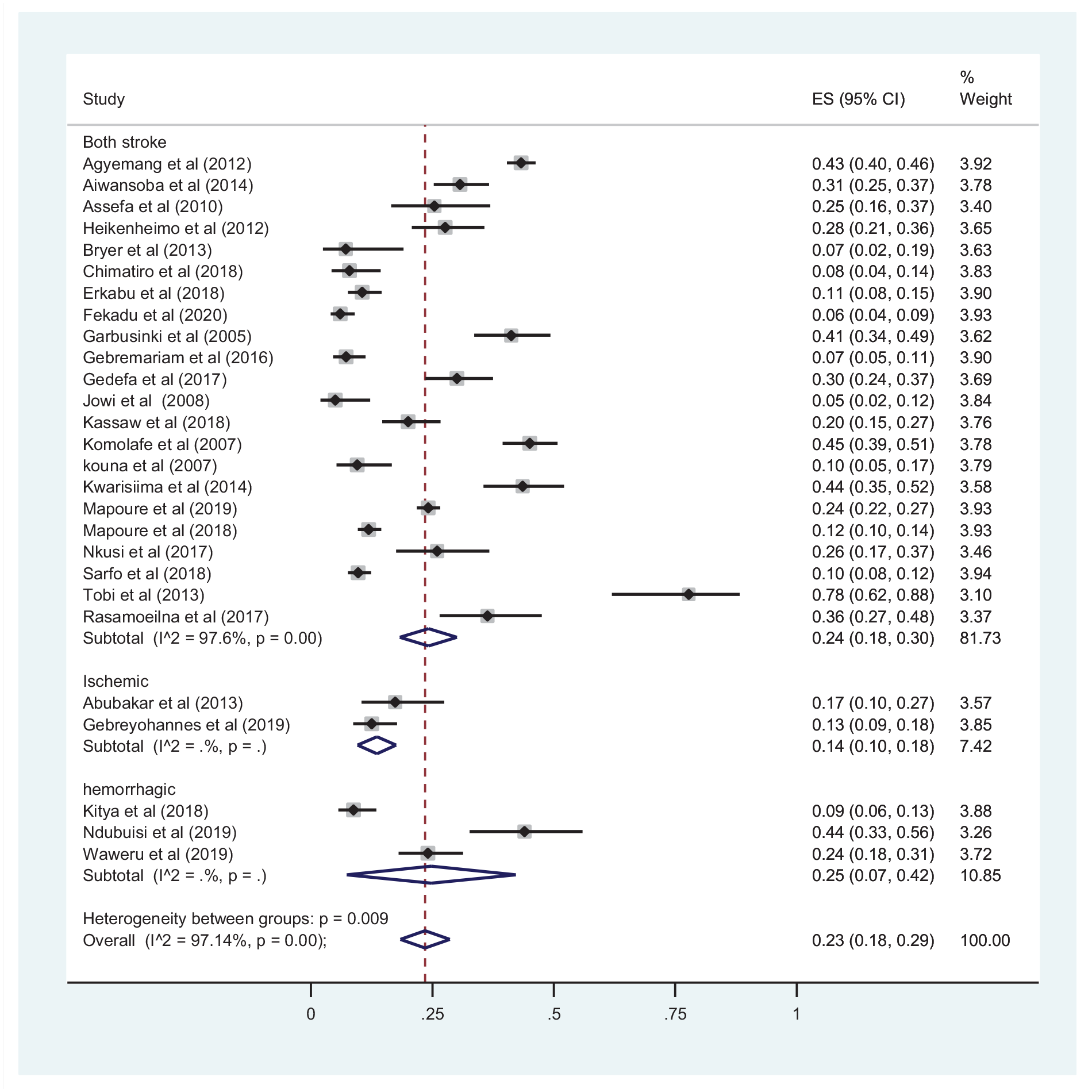
Forest plot describing in-hospital mortality by type of stroke.
Predictors of in-hospital mortality among stroke patients in sub-Saharan Africa
As a result of the heterogeneity in reporting the factors, the pooled estimate factors associated with in-hospital outcomes were not computed. Therefore, all of the included studies that addressed the determinants of in-hospital mortality among stroke patients were systemically reviewed. In a study conducted in Western Africa, admission Glasgow Coma Scale (p = 0.002) and Canadian Neurological Scale status (p = 0.002) had significantly influenced in-hospital mortality. 14 Similarly, another study conducted in Western Africa depicted that the Glasgow Coma Scale <8 on admission was significantly associated with increased in-hospital mortality among stroke patients (adjusted odds ratio (AOR) = 6.06, 95% CI = 3.17–12.79). 35
The severity of stroke at admission,21,25 ischemic types of stroke,21,35 and undetermined types of stroke 16 were reported as determinants of in-hospital mortality among hospitalized stroke patients. A study by Garbusinski et al. 21 revealed fever and lung infection were significant predictors of death. Similarly, a study conducted by Gebreyohannes et al. 23 in northwest Ethiopia has shown that the presence of any infection was significantly associated with in-hospital mortality. Similarly, the study conducted by Russell et al. 35 reported that the presence of aspiration pneumonia heralding the in-hospital mortality of stroke patients (AOR = 3.03, 95% CI = 1.44–6.36, p = 0.001).
Several studies revealed that older age was significantly associated with in-hospital mortality.15,25,32,37 The presence of vascular disease was identified to decrease the in-hospital mortality among ischemic stroke patients. 23 However, another study has shown that the presence of hypertension at admission was significantly associated with all-cause mortality among stroke patients. 35 Previous stroke and clinical diagnosis were reported as a common risk factor of in-hospital mortality in a study conducted in Sierra Leone. 35 Moreover, female gender, 21 the severity of ictus at admission, 37 absence of aspirin treatment, 21 and a decrease in renal function 23 were also reported to influence the in-hospital mortality from acute stroke significantly.
Publication bias
In the present meta-analysis and systemic review, the funnel plot and the Egger test (p-value = 0.054) have not indicated publication bias among the included studies (Figure 5).

Funnel plot of standard error by logit event rate for publication bias.
Discussion
This systematic review and meta-analysis evaluated the in-hospital mortality from acute stroke in sub-Saharan Africa. The review included 27 studies that full filled the predefined eligibility criteria. The overall in-hospital mortality rate was 22% (95% CI = 0.17–0.27). It was ranged from 5.0% 26 to 78% 36 when the results of the individual studies were considered. The mortality rate reported in this review was slightly higher when compared with the mortality rate reported in the meta-analysis conducted by Alene et al. 40 (18%).
In contrast, there was a significant reduction in the stroke death rate in the developed countries, which could be due to the modifiable nature of most of the risk factors of stroke. 41 Nevertheless, about 50% of stroke-related deaths are due to inadequate management of preventable modifiable risk factors stroke globally. 42
The high in-hospital mortality rate from acute stroke in sub-Saharan Africa might be linked to the poor management of preventable risk factors of stroke due to limited healthcare facilities and lack of awareness about the clinical characteristics of the disease. 20 Furthermore, most developing countries failed to understand the advantage of early admission of patients hospitalized with acute stroke. Hence, most of them have late admission, which creates management difficulties as these first hours are essential to avoid secondary insults to the brain. 43 In a previous study, most patients were not candidates for thrombolytic therapy due to late admission to the hospital, which is the most effective treatment modality to achieve better outcomes among patients with ischemic stroke. 20 In addition, governments and health planners in sub-Saharan Africa tend to underestimate the importance of stroke treatment.
Similarly, a Chinese study showed in-hospital mortality reduction of stroke from 3.16% in 2007 to 2.30% in 2010. This may be due to the advancement of stroke care in the country. 44 In contrast, the prevalence of mortality due to stroke in sub-Saharan Africa was lower than a Brazilian study, which reported a mortality rate of 32%. 45 The results of sub-group analysis revealed that the mortality rate was 37%, 18%, and 15% in Western, Southern, and Eastern Africa, respectively. This disparity could be due to differences in the clinical characteristics among study participants and the quality of care provided in sub-Saharan Africa regions.
A previous review reported that hemorrhagic stroke was a significant cause of death, although ischemic stroke was more frequent. 46 Accordingly, in this systemic review and meta-analysis, the pooled estimated in-hospital mortality rate for hemorrhagic stroke (25%) was higher than ischemic stroke (14%). Similarly, a study in Europe reported an in-hospital mortality rate of 9.8% for ischemic stroke and 26.6% for hemorrhagic stroke in 2017. 47 Besides, an in-hospital mortality rate of 4% was reported due to ischemic stroke in Asian countries. 48 This is far lower than our review’s in-hospital fatality rate due to ischemic stroke (14%). Paradoxically, ischemic stroke type was a significant (60%) cause of death in Asian countries. 49
Even if the pooled estimate factors determining the in-hospital mortality were not computed in this review, several factors were reported to influence the in-hospital mortality rate in the included studies. Thus, patient age (>55 years) was reported as a common risk factor of in-hospital mortality from acute stroke in sub-Saharan Africa.15,25,32,37,50
In addition, clinical diagnosis in the absence of imaging was also reported as a predictor of in-hospital mortality from acute stroke in the included studies. 35 This is in line with the reports of systematic review and meta-analysis conducted in Nigeria. 51 Moreover, statins use was reported as protective of in-hospital mortality among patients hospitalized with acute stroke. 23 This is supported by a current review that depicted statins are associated with better survival and improved functional outcome when administered during the acute phase of stroke. 52 It seems that both lipid-lowering and pleiotropic effects contribute to these effects.
Limitation of the study
The present meta-analysis has posed some limitations that should be considered in interpretation. First, studies from a few countries in sub-Saharan Africa included in this meta-analysis may be difficult to generalize the findings to all stroke patients in the region. Second, this systematic review and meta-analysis included only articles reporting in the English language, which may restrict our findings. Besides, only a few studies reported in-hospital mortality among stroke patients. Third, inconsistent reporting of some variables has limited the conclusiveness of the factors associated with in-patient mortality due to stroke.
Conclusion and recommendations
In summary, in-hospital mortality among stroke patients in sub-Saharan Africa was high. The mortality rate was higher in Western Africa as compared to the Eastern and Southern African sub-Saharan Africa. In sub-Saharan Africa, priorities should be given to primary prevention of stroke, particularly the detection and management of hypertension, smoking cessation, diabetes control, and lifestyle modifications to reduce mortality due to stroke. Besides, promoting public awareness about the preventable nature of stroke and the warning signs and symptoms should also be implemented to deter disease progression early.
Footnotes
Acknowledgements
The authors are thankful to all individuals who helped us through this systemic review and meta-analysis.
Availability of data and materials
The data sets used and/or analyzed during this study are available from the corresponding without any limitation.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.