
Abstract
Objective:
Podoconiosis, one of the neglected tropical diseases (NTDs), affects barefoot people in impoverished regions and contributes to poverty by having negative impacts on economic output, education, and disability. People who have the disease waste nearly half of all of their productive workdays. There is limited evidence available on prevalence of podoconiosis in sub-Saharan Africa (SSA). Therefore, the aim of this research was to determine the pooled prevalence of podoconiosis in the SSA over the last 10 years.
Methods:
Studies were retrieved from PubMed, Embase, Web of Science, Scopus, Google Scholar, and Google by using a combination of search terms with Boolean operators. All authors independently assessed each study’s quality using the modified Newcastle–Ottawa Scale for cross-sectional studies. STATA Version 14 was used to conduct the statistical analysis. The random-effect approach of meta-analysis was used. To test for heterogeneity, I-Squared (I2) statistics were employed and sensitivity analysis with a leave-one-out was done.
Result:
In this systematic review and meta-analysis, a total of 16 publications with 2,195,722 individuals were included. The pooled prevalence of podoconiosis was 2.66 (95% confidence interval (CI): 2.24, 3.10) with heterogeneity index (I2) of 99.9%. Walking barefoot adjusted odd ratio (AOR) 5.35 (95% CI: 1.65, 9.05), p = 0.001, not washing feet with soap and water regularly AOR 2.8 (95% CI: 1.16, 4.44, p = 0.001), and an increased age AOR 2.23 (95% CI: 1.25, 5.58) were factors significantly associated with the prevalence of podoconiosis.
Conclusion:
This study revealed that pooled prevalence of podoconiosis was considerable in SSA. Age, being barefoot, and failing to wash one’s feet with soap and water have been identified to be factors that were significantly associated with the prevalence of podoconiosis. Therefore, creating awareness on shoe wearing and providing shoes in communication with supporting organizations in podoconiosis prevalent areas, and early diagnosis based on family history are needed for the prevention of podoconiosis
Introduction
Podoconiosis, one of the neglected tropical diseases (NTDs), affects barefoot people in impoverished regions and contributes to poverty by having negative impacts on economic output, education, and disability. 1 It is a noninfectious type of elephantiasis that affects persons who are barefoot and have been exposed to red clay soil for a long time. It is prevalent in northern India, Central America, and tropical Africa. 2 Globally, there are 17 countries with evidence of podoconiosis presence and 12 of them are African countries. These 12 African nations were found to have podoconiosis, with perfect agreement on the disease’s occurrence in 6 of them (Cameroon, Ethiopia, Kenya, Tanzania, Rwanda, and Uganda), and substantial evidence in 4 others (Burundi, Cape Verde, So Tomé and Prncipe, and Sudan). 3
Podoconiosis is characterized by bilateral swelling below the knee, which can be avoided and managed by putting on shoes, regularly bathing the foot as well as applying antiseptics and emollients. 2
Lymphatic filariasis and the non-filarial elephantiasis known as podoconiosis are the two main kinds of elephantiasis. Podoconiosis is a nonparasitic illness, whereas lymphatic filariasis is caused by parasitic worms. 4
It is a condition that is caused by a combination of environmental and inherited factors. There have been no reports of any biological agents. There is a link between podoconiosis and regions of the genome frequently engaged in T-cell driven inflammatory reactions as well as a heightened helper T-cell response in the lymph nodes of persons with podoconiosis. 5
Although the pathophysiology of the disease has not yet been thoroughly researched, it is thought that it is brought on by tiny dirt particles that penetrate the skin and cause the lymphatic system to become irritated. 6
The substances come into touch with the exposed skin under the feet, ascend up to the lymphatic veins, obstruct them, and cause an infection termed as podoconiosis.7,8
The World Health Organization presently lists the condition as one of the NTDs in endemic areas.9–17
Podoconiosis affects four million people worldwide, with the majority of them living in highland regions of tropical Africa, Central and South America, and various regions of Asia. 18
Podoconiosis severely hampers sufferers’ human rights. They are unable to exercise their right to the things they require to live at a level of living sufficient for their health and well-being. Social and economic prospects are eventually disrupted by failing to address health risks. Podoconiosis puts a strain on patients’ social, psychological, and financial well-being and causes them to miss work and work less hours because of frequent acute bouts and anxiety about being stigmatized. Podoconiosis consequently poses a serious danger to possibilities for career and education. 19 Podoconiosis has numerous negative consequences, such as an immense economic and social challenge; it additionally contributes to significant stigma at school, employment, or the market, as well as marginalization from social ties like marriage. 20
Around half of the total productive workdays of those who have podoconiosis are lost. Podoconiosis is predicted to cost a population of 1.5 million people US$16 million per year in direct and productivity expenditures, putting a US$208 million annual financial cost on Ethiopia. 21
Other than the economic and societal effects, complications are the most common side effects of podoconiosis. People with podoconiosis scored significantly lower on all quality of life measures in one SSA country, Ethiopia, including hygienic circumstances, nutritional status, and accessibility to shoes. 22 Thus, these situations lead to acute adenolymphangitis, one of the main consequences of podoconiosis, which results in 149.5 days of lost activity each year. 23
Podoconiosis patients face a significant level of prejudice and discrimination in important spheres of life, including marriage and work. Forced divorce affects the majority of people, and breakups in marriage were highly common. 2
In recent years, there have been a number of positive advancements in the fight against podoconiosis. In four endemic countries (Ethiopia, Uganda, Rwanda, and Cameroon), national or local strategies have been launched for the control and eradication of podoconiosis. Three nations have finished their nationwide mapping of podoconiosis, 24 and at least three others have made notable advancements in their surveillance systems. Ethiopia has also improved the availability of morbidity management services. 25
Despite various impressive achievements in reducing the public health issue of podoconiosis in SSA, there are still a number of significant obstacles that must be taken into particular account at the SSA regional and international level. The challenges persist: an absence of a global strategy for the control or elimination of podoconiosis exists; 26 the disease is the least financed NTDs; 27 regarding new and improved tools for podoconiosis prevention, control, and eradication, there is a lack of innovation; 25 and there is a shortage in reliable data for decision-making to make the best use of the resources at hand. 28
Hence, thorough data and ongoing updates on the disease’s burden are required to strengthen the current strategy and create a fresh plan to end podoconiosis. The objective of this study was to determine the pooled prevalence of podoconiosis throughout the sub-Saharan Africa (SSA) over the last 10 years.
Methods
Search strategy
Preferred Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines were followed. Search for published articles was done by using different data bases. We searched systematically data bases PubMed, Scopus, Web of sciences, Embase, MEDLINE, Google Scholar and Google by using terms “podoconiosis,” “non-filarial elephantiasis,” “mossy-foot,” “epidemiology,” “prevalence,” “magnitude” and the name of sub-Saharan countries by combinning the boolean operator “OR” combined by or. Articles published in English Language in the last 10 years were searched. With registration number (CRD42023392583), the study protocol was submitted to and published in the PROSPERO international prospective register of systematic reviews (Supplemental Material 1). The PRISMA criteria were followed for the literature search approach, study selection, data extraction, and result reporting in this systematic review and meta-analysis. 29 Endnote Version X7 Software for managing references was used to download, arrange, review, and cite linked publications.
Criteria for article selection
Inclusion criteria
Articles published in English Language, which assessed prevalence/magnitude of podoconiosis, articles published in the last 10 years in member countries of SSA (from 1 February 2012 to 1 February 2023) and cross-sectional studies were included.
Exclusion criteria
Studies that were published in languages apart from English were not included. Studies conducted on podoconiosis but did not assess the prevalence/magnitudes were also excluded. Case reports, review, methodologically poor studies, and interventional studies were excluded from this review.
Quality assessment of included studies
The modified Newcastle–Ottawa Scale (NOS) for cross-sectional research was used to rate the quality of each study. 30 The scale, which has eight categories, assessed the included articles based on their selection, comparability, assessment of their exposure, and their outcomes. The point score and interpretation were as follows: Quality is rated from 0 to 5 as low quality, 6–7 as moderate, and 8 and above being considered high quality. We only incorporated items with a minimum NOS rating of 6 (Supplemental Material 2). AA and EW evaluated the quality of each study using NOS. Researchers evaluated the titles and abstracts of the identified studies for their suitability to the review and were checked and the full texts of relevant articles were retrieved by TLA.
Data extraction and synthesis
Data extraction was done after the study search was completed. Each study was carefully read by AA and EW and the figure of the prevalence/magnitude of podoconiosis, and factors associated were identified, and extracted to a preprepared data extraction Excel sheet. After extracting data by excel, they were exported to STATA Version 14.
Data analysis
Data analysis was conducted by STATA version 14. Funnel plot was used for checking the publication bias of the studies via personal observation of authors and forest plot was used for checking the analysis results briefly by using confidence intervals. Random-effect model was used for the estimation of pooled prevalence of podoconiosis. Heterogeneity analysis test was done. Subgroup analysis between countries was conducted and sensitivity analysis of studies was tested.
Results
In the beginning, 637 studies were first gathered via manual searching and database searches. Fifteen duplicates were detected from this and eliminated. A total of 542 unrelated studies were eliminated after screening based on their title and abstract. The remaining 80 articles were evaluated for suitability and 62 of them were excluded for not reporting the wanted outcome, podoconiosis studies with no prevalence, or not primary studies. At the end, 16 articles met the study’s inclusion requirements (Figure 1).

PRISMA flowchart diagram of the study selection.
Features of the study
This systematic review and meta-analysis comprised a total of 16 publications involving 2,195,722 people from four SSA countries. All 16 studies included were cross-sectional in design. The number of participants included in the samples varies throughout studies, from 366 31 to 1,360,612 32 participants. The highest numbers (nine) of studies were included from Ethiopia and one study was obtained from Rwanda. The lowest prevalence of podoconiosis (0.07% )was reported in Rwanda, 32 and the highest (6.3%) was reported from Ethiopia 28 (Table 1).
Information about the articles that were included in the systematic review and meta-analysis of the prevalence of podoconiosis in SSA in 2023 (n = 2,195,722).

Prevalence of podoconiosis in SSA
The pooled effect size was calculated using a DerSimonian and Laird random-effects model. Based on the estimate, the pooled prevalence of podoconiosis among adults was 2.66 (95% confidence interval (CI): 2.21, 3.10) with heterogeneity index (I2) of 99.9% (p < 0.001) (Figure 2).
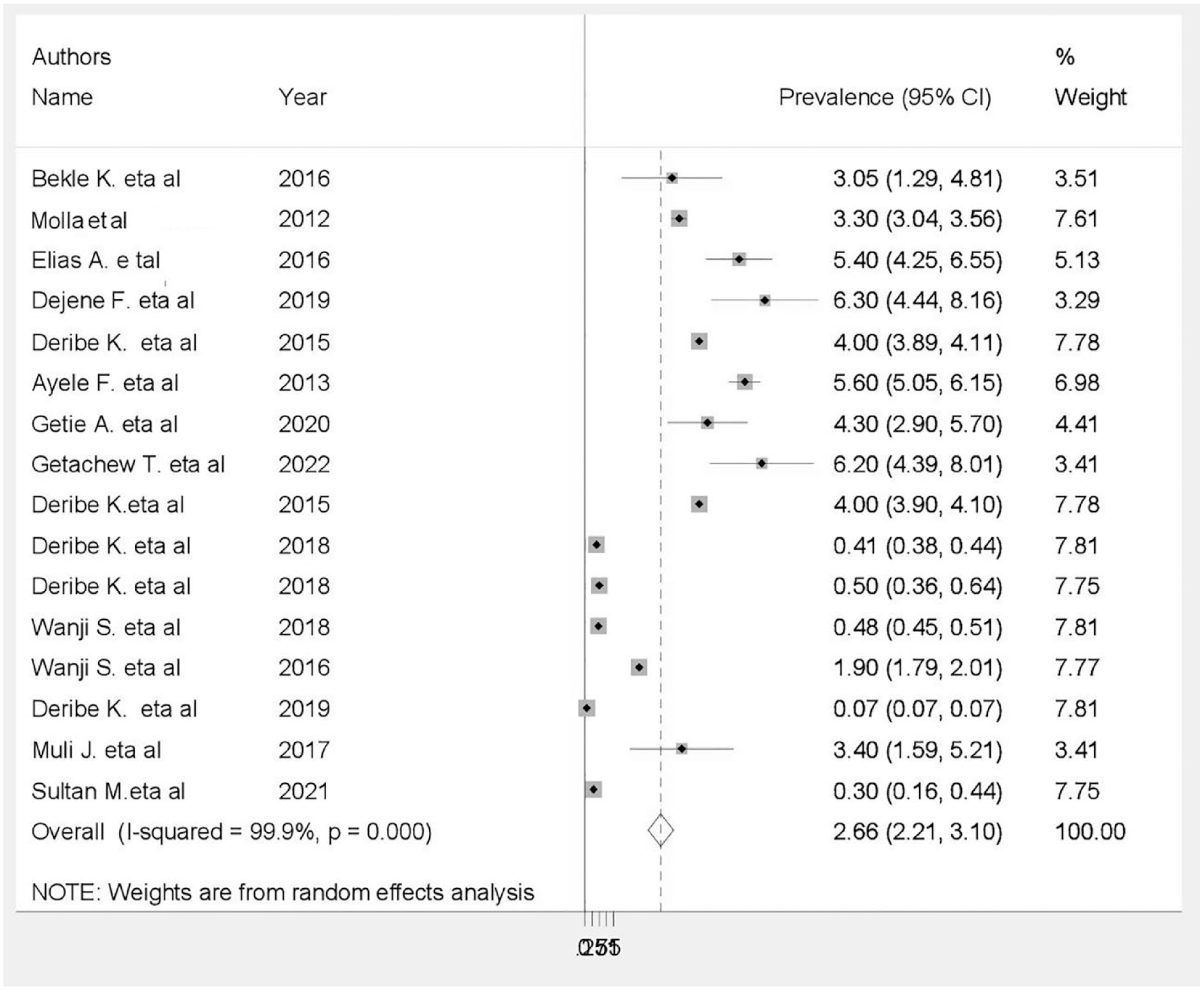
Forest plots showing the pooled prevalence of podoconiosis in SSA.
Subgroup analysis
Subgroup analyses showed a substantial variation between countries, highest prevalence of podoconiosis was 4.32 (95% CI: 3.96, 4.68) and the lowest was (0.07, 95% CI, 0.07, 0.07) seen in Ethiopia and Rwanda, respectively (Figure 3).

Subgroup analysis of prevalence of podoconiosis by countries in SSA.
Heterogeneity and publication bias
We conducted a subgroup analysis based on the data from this study to correct and reduce the reported huge heterogeneity among countries in SSA and conducted random-effect model. To pinpoint the cause of heterogeneity, meta-regression employing sample size and publication year as covariates was also carried out. According to regression, sample size and year of publication have little impact on the degree of heterogeneity between studies (Table 2). Egger’s test and a funnel plot were used to visually and graphically assess the presence of publication bias for included studies.31–46 Visual inspection of the funnel plot revealed an uneven distribution (Figure 4), which the Egger test revealed to be statistically significant (p < 0.001). The final effect size was therefore calculated using trim and fill analysis with the random-effects model (Figure 5). But utilizing the model, a comparable effect magnitude was discovered. Additionally, we performed sensitivity analysis by gradually deleting studies to assess the impact of each study (Table 3).
Analysis of the factors influencing the between-study heterogeneity using meta-regression.

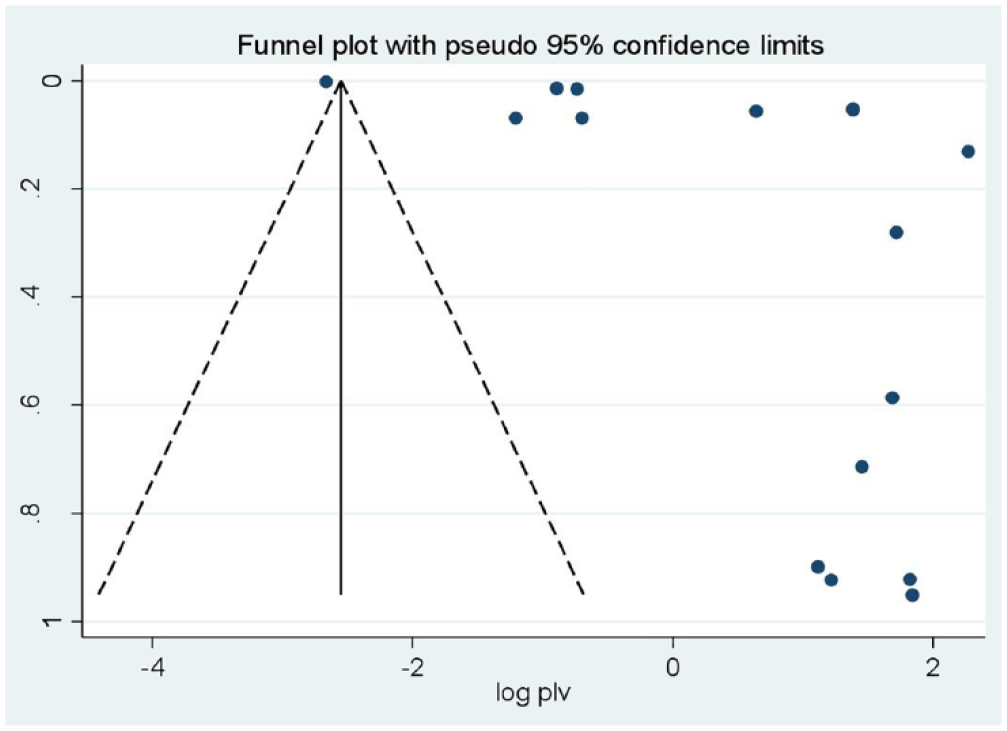
Funnel plot to test the publication bias in 16 studies with 95% confidence limits.
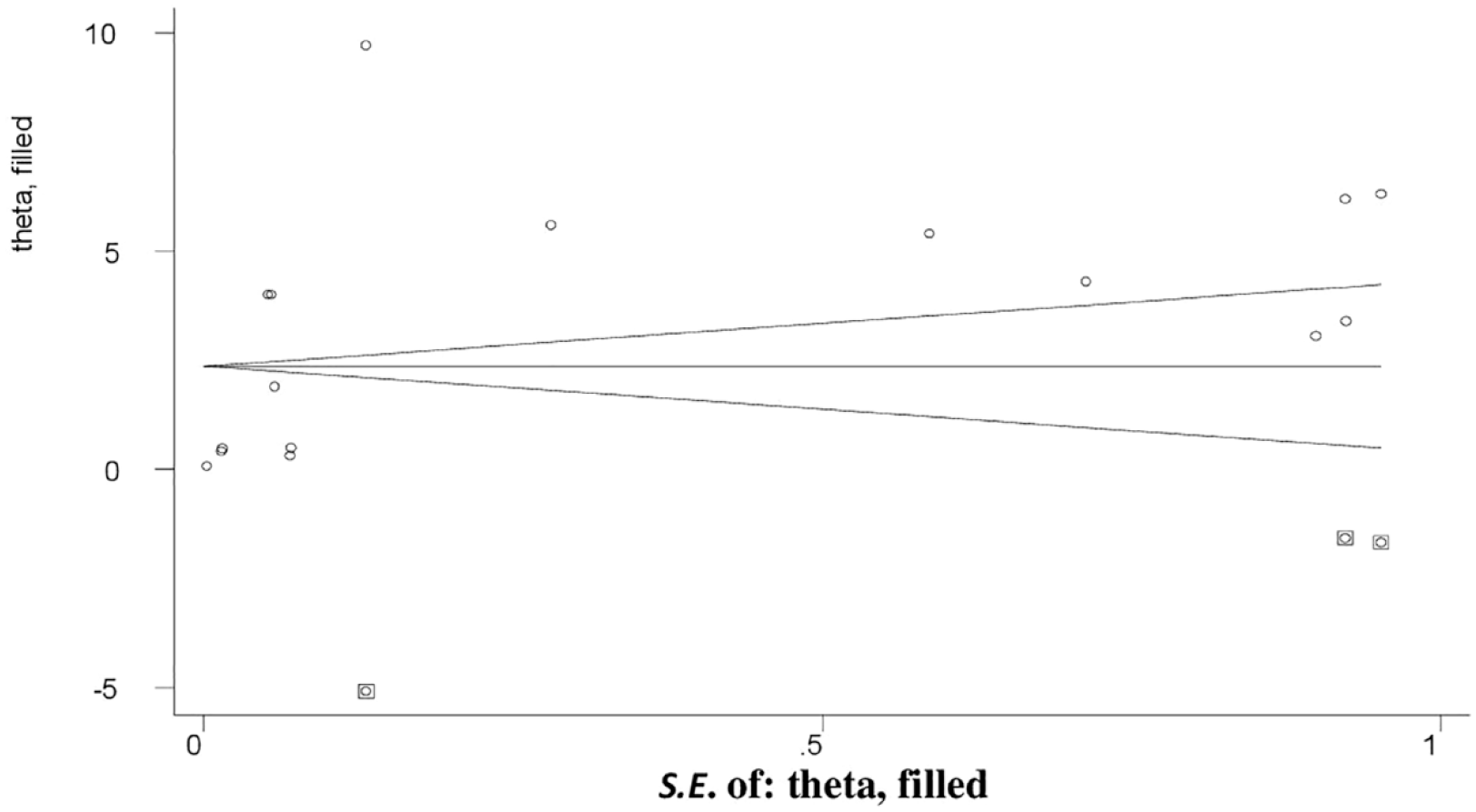
Filled funnel plot after adjusting for publication bias with 95% confidence limits.
Sensitivity analysis of the combined prevalence for removing each study one at a time.

Factors associated with magnitude of podoconiosis in SSA
To determine the variables associated with the prevalence of podoconiosis in adults, eight variables were retrieved. From these variables, three (barefoot, washing foot with soap and water, and age) were found to be significantly associated with occurrence of podoconiosis. Participants who walk barefoot were 5.73 (95% CI: 2.49, 8.96), p = 0.001 times more likely to get podoconiosis (Figure 6).

Pooled effect (adjusted odd ratio) of the association between walking on barefoot and occurrence in Ethiopia, 2023.
This study revealed that participants who do not wash their feet with soap and water regularly were 2.8 (95% CI: 1.16, 4.44, p = 0.001) times more likely to acquire podoconiosis than participants who wash their feet with soap and water (Figure 7).
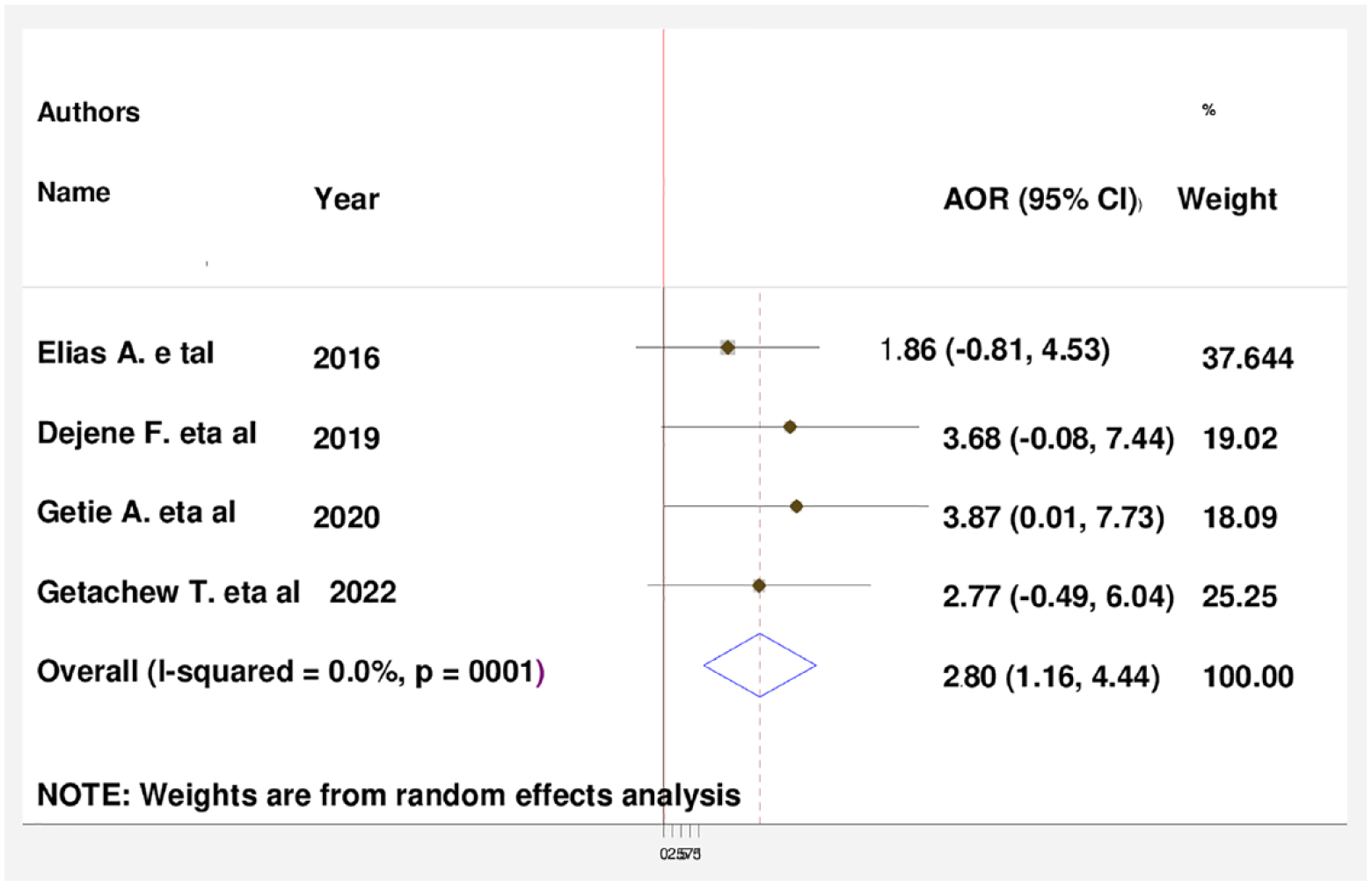
Pooled effect (adjusted odd ratio) of the association between not washing feet with soap and water and occurrence of podoconiosis among adults in Ethiopia, 2023.
The current study indicated that increased age has 2.23 (95% CI: 0.16, 4.3) times higher chance of getting podoconiosis than younger ages (Figure 8).

Pooled effect (adjusted odd ratio) of the association between increased age and occurrence of podoconiosis in Ethiopia, 2023.
Because of significant heterogeneity in this study, we conducted a subgroup analysis among SSA countries. There is significant difference between prevalence of podoconiosis among included countries in this study. The subgroup analysis identified that Ethiopia had a high pooled prevalence of podoconiosis, which is 4.32 (95% CI: 3.96, 4.68), and the lowest prevalence was seen in Rwanda, 0.007. We also used random-effect model to control heterogeneity. Publication bias of the study was checked via Egger’s test and visual inspection of funnel plots. Funnel plot showed that the included studies had asymmetrical distribution, so that we conducted trim and fill method.
Discussion
This study was conducted to determine the prevalence of podoconiosis in SSA. The pooled prevalence of podoconiosis in SSA was 2.66 (95% CI: 2.21, 3.10). This finding is comparable with single studies conducted in Ethiopia 33 and in Kenya. 45 The current study finding is lower compared to researches conducted in Ethiopia,34,35,38,39,47–49 9.7%, 5.4%, 4.3%, 6.2%, 7.4%, 5.6%, and 5.1%, respectively. The difference may be related to an overall steady rise in practices of putting on footwear, improved availability of sanitary tools such as soap, and growing knowledge of broader social and hygienic aspects.
Concerning subgroup analysis, the highest prevalence of podoconiosis was observed in Ethiopia and the lowest was in Rwanda, this may be due to number of studies included from Ethiopia is high, this may underestimate the prevalence of podoconiosis in Rwanda.
According to the findings of this meta-analysis, the occurrence of podoconiosis was significantly associated with participants’ age, going barefoot, and not washing one’s feet with soap and water.
This review revealed that study participants who walk barefoot were 5.73 (95% CI: 2.49, 8.96), p = 0.001 times more likely to get podoconiosis than participants who wear shoes. This finding is similar to studies conducted in Ethiopia,30,31,34–36 Kenya, 44 and Cameroon. 45 This is because walking bare foot exposes people to mineral particles and this long-term exposure to mineral particles predisposes people to develop podoconiosis. 50
The current finding showed that participants who do not wash their feet with soap and water regularly were 2.8 (95% CI: 1.16, 4.44, p = 0.001) times more likely to acquire podoconiosis than participants who wash their feet with soap and water. This finding is comparable with studies conducted in Ethiopia.34–39,47 This may be the reality that washing the feet regularly may help to remove any dust or other factors that could otherwise produce a super infection.
This study showed that increased age has 2.23 (95% CI: 0.16, 4.3) times higher chance of getting podoconiosis than younger ages. This result is in line with research done in Ethiopia34–46 and in Cameroon. 45 It is to be believed that as people get older, the likelihood of developing podoconiosis rises, probably as a result of repeated exposure to irritated soil. Moreover, changes in shoe-wearing habits and cumulative exposure to the alleged causes over a person’s lifetime are potential contributing factors.
This analysis found that although podoconiosis is frequent in SSA and has been documented by prior studies, many of these countries lack recent findings that indicate the prevalence of the condition.
Limitations
There are some limitations that need to be taken into account in the future study even if this systematic review and meta-analysis offers the most recent information regarding the epidemiology of podoconiosis in SSA. First, we could not find studies from many of SSA countries except Ethiopia, Cameroon, Rwanda, and Kenya, and generalizing the results to the entire SSA countries may be challenging. Secondly, we found high variability among the included studies and the existence of publication bias; hence, the results must be interpreted with caution
Conclusion
This study revealed the pooled prevalence of podoconiosis in SSA was considerable. Most of the podoconiosis studies were concenterated in two of SSA countries, such as Ethiopia and Cameroon. Age, walking barefoot, and not washing feet with soap and water were discovered to be strongly linked to the prevalence of podoconiosis. Therefore, creating awareness on shoe wearing and providing shoes in communication with supporting organizations in podoconiosis prevalent areas, teaching the communities about washing feet with soap and water, limiting the soil contact with feet and early diagnosis based on family history are needed for the prevention of podoconiosis.
Supplemental Material
sj-pdf-1-smo-10.1177_20503121231193602 – Supplemental material for Epidemiology of podoconiosis in sub-Saharan Africa: A systematic review and meta-analysis
Supplemental material, sj-pdf-1-smo-10.1177_20503121231193602 for Epidemiology of podoconiosis in sub-Saharan Africa: A systematic review and meta-analysis by Temesgen Lera Abiso, Amene Abebe Kerbo and Eskinder Wolka Woticha in SAGE Open Medicine
Supplemental Material
sj-pdf-2-smo-10.1177_20503121231193602 – Supplemental material for Epidemiology of podoconiosis in sub-Saharan Africa: A systematic review and meta-analysis
Supplemental material, sj-pdf-2-smo-10.1177_20503121231193602 for Epidemiology of podoconiosis in sub-Saharan Africa: A systematic review and meta-analysis by Temesgen Lera Abiso, Amene Abebe Kerbo and Eskinder Wolka Woticha in SAGE Open Medicine
Supplemental Material
sj-pdf-3-smo-10.1177_20503121231193602 – Supplemental material for Epidemiology of podoconiosis in sub-Saharan Africa: A systematic review and meta-analysis
Supplemental material, sj-pdf-3-smo-10.1177_20503121231193602 for Epidemiology of podoconiosis in sub-Saharan Africa: A systematic review and meta-analysis by Temesgen Lera Abiso, Amene Abebe Kerbo and Eskinder Wolka Woticha in SAGE Open Medicine
Footnotes
Acknowledgements
We would like to forward our gratitude to Wolaita Sodo University, College of Health Sciences and Medicine. We also thank all authors of primary study and participants of the primary study.
Author contributions
TLA, AA, and EW equally contributed to this research work.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.