
Abstract
Background:
People with type 2 diabetes (T2D) are at high risk of fragility fractures; however, there are no randomized controlled trials evaluating the efficacy of anti-osteoporosis drugs as a primary pre-specified endpoint in T2D.
Objectives:
To compare the efficacy of anti-osteoporotic drugs in postmenopausal women with T2D.
Design:
Prospective, randomized, open, blinded endpoint clinical pilot trial.
Methods:
Postmenopausal women (⩾50 years) with T2D (duration ⩾5 years), HbA1c 7–10%, eGFR ⩾45 mL/min/1.73 m2 and prior vertebral (clinical/morphometric), hip, radius, humeral fragility fracture or bone mineral density (BMD) T-score (adjusted for diabetes) at lumbar spine/femoral neck ⩽−2.5 and high FRAX score will be eligible for inclusion. Subjects with secondary causes of osteoporosis, prior exposure to bone-active therapies or history of use of glucocorticoids/pioglitazone/thiazides/canagliflozin will be excluded. Finally, eligible subjects will undergo estimation of serum calcium, phosphate, alkaline phosphatase, parathyroid hormone, 25-hydroxyvitamin D and bone turnover markers (BTMs) (total procollagen type I N-propeptide, β-CTX) along with trabecular bone score (TBS) and high-resolution peripheral quantitative computed tomography (HR-pQCT) of non-dominant hand and leg. After a 2-week run in phase, they will be randomized in a 1:1:1:1 ratio to receive yearly zoledronate, or biannually denosumab or daily teriparatide (in addition to standard of care, i.e., calcium 1000 mg/day and cholecalciferol 1000 IU/day) or only standard of care (control). The primary endpoints will be change in areal BMD and frequency of incident fractures at 18 months. The secondary endpoints will be change in HR-pQCT parameters, TBS and BTMs at 18 months. Adverse events will be recorded for all randomized participants.
Ethics:
The study has been approved by the Institute Ethics Committee. Written informed consent will be obtained from each participant.
Discussion:
The trial is expected to provide information regarding optimal anti-osteoporotic therapy in people with T2D and bone fragility.
Registration:
Prospectively registered in Clinical Trial Registry of India (CTRI/2022/02/039978).
Introduction
Several epidemiological studies have consistently shown that people with diabetes are at a high risk of fragility fractures than non-diabetic controls. 1 The risk is increased in type 1 (T1D) as well as type 2 diabetes (T2D), being consistently higher in people with T1D than in T2D. In a recent meta-analysis that included more than 17 million people with diabetes, the relative risk of hip and non-vertebral fractures in people with T2D was 1.33 and 1.19, respectively. 2
Notably, although fracture risk is increased, areal bone mineral density (BMD) is higher in people with T2D as compared to age- and sex-matched healthy controls. This apparent paradox is attributed to deteriorated bone microarchitecture in people with T2D, irrespective of the BMD. Evidence suggests that T2D is primarily associated with adverse cortical characteristics 3 ; nevertheless, recent data also hint towards poor trabecular bone quality in T2D. 4
Despite advances in the knowledge about the pathogenesis and diagnosis of bone fragility in diabetes, very little is known regarding its optimum treatment. Available data on the use of anti-osteoporotic agents in T2D are limited to only a few observational studies or post hoc analyses or subgroup analyses of randomized controlled trials (RCTs) without pre-specified bone disease-related endpoints. Besides, there are no head-to-head RCTs comparing one anti-osteoporotic drug over the other in people with T2D. 5
Furthermore, most of the available studies have included people with osteoporosis (based on BMD alone) instead of people with fragility fractures. In all the available studies, osteoporosis has been defined classically as BMD T-score ⩽ −2·5; nevertheless, since people with T2D tend to have higher BMD, osteoporosis in T2D sets in at a T-score of −2.0. Hence, for evaluating the efficacy of anti-osteoporotic therapies in T2D, subjects with T-score ⩽ −2·0 should ideally be recruited.
In the absence of robust evidence, hitherto, bisphosphonates remain the first choice for treating bone fragility in people with T2D. However, since T2D is a state of low bone turnover, there are theoretical concerns over using anti-resorptive agents. 6 That anabolic agents might be a better choice than anti-resorptives in the setting of T2D is unknown.
Considering the noticeable dearth in the available literature, the present randomized controlled trial has been planned to compare the efficacy of anti-osteoporotic agents in postmenopausal women with T2D.
Methods
Study design
The proposed study is a prospective, randomized, open, blinded endpoint clinical pilot trial of 72 weeks duration conducted at the Postgraduate Institute of Medical Education and Research (PGIMER), Chandigarh, India. The trial is designed to compare the efficacy of the three available anti-osteoporotic agents, teriparatide, zoledronate, or denosumab, in postmenopausal women with T2D at high risk of fragility fractures. The trial is prospectively registered on the Clinical Trial Registry of India (CTRI/2022/02/039978).
Patients
Asian-Indian ambulatory postmenopausal women ⩾50 years of age with at least 5 years of menopause and diagnosed with T2D for at least 5 years will be screened for possible inclusion in the study. All subjects will be inquired about any prior history of fragility fractures. Those with an estimated glomerular filtration rate (eGFR) ⩾ 45 mL/min/1.73 m2 (based on CKD-EPI formula), body mass index ⩾23 kg/m2 and glycated haemoglobin (HbA1c) ⩾7% and ⩽10% will be asked for written consent for additional screening procedures to be undertaken. Accordingly, they will undergo estimation of areal BMD at the lumbar spine, femoral neck and distal one-third radius (non-dominant) using dual-energy X-ray absorptiometry (DXA; HOLOGIC Discovery A, QDR 4500, Hologic, Inc., Bedford, MA, USA) and a lateral radiograph of the lumbosacral spine to look for the presence of any morphometric vertebral fractures.
Subsequently, the FRAX® score will be calculated using the online calculator (https://frax.shef.ac.uk/FRAX/tool.aspx?country=51) after lowering the T-score at the femoral neck by −0.5, the correction that is commonly used to estimate the true fracture probabilities in people with T2D. Finally, screened subjects with a prior vertebral (clinical or morphometric), hip, radius, or humerus fragility fracture will be included in the study. In the absence of the aforementioned fragility fractures, those with a screening BMD T-score at lumbar spine or femoral neck ⩽ −2.5 (corrected for T2D) and a high FRAX® score will be considered eligible for subsequent randomization. For the present study, a FRAX® score ⩾ 2.5% and ⩾ 9% for hip fracture and major osteoporotic fracture, respectively, will be considered based on the observations from a recent study from southern India where the cut-offs mentioned above predicted fragility vertebral fractures with sensitivities of 77–88% and specificities of 55–72%. 7
Patients will be excluded if they have any of the following characteristics: T1D, latent autoimmune diabetes of adults (LADA) or secondary diabetes mellitus; prior history of use of bone-active therapies (bisphosphonates, teriparatide, denosumab, selective estrogen receptor modulators, hormone replacement therapy and calcitonin); history of glucocorticoid use [⩾ 5 mg (prednisolone or equivalent) for ⩾ 3 months]; history of use of pioglitazone, thiazides or canagliflozin over last 6 months; history suggestive of secondary causes of osteoporosis and history of tooth extraction over the prior 6 months.
The full inclusion and exclusion criteria have been detailed in Table 1.
Showing the proposed inclusion and exclusion criteria.
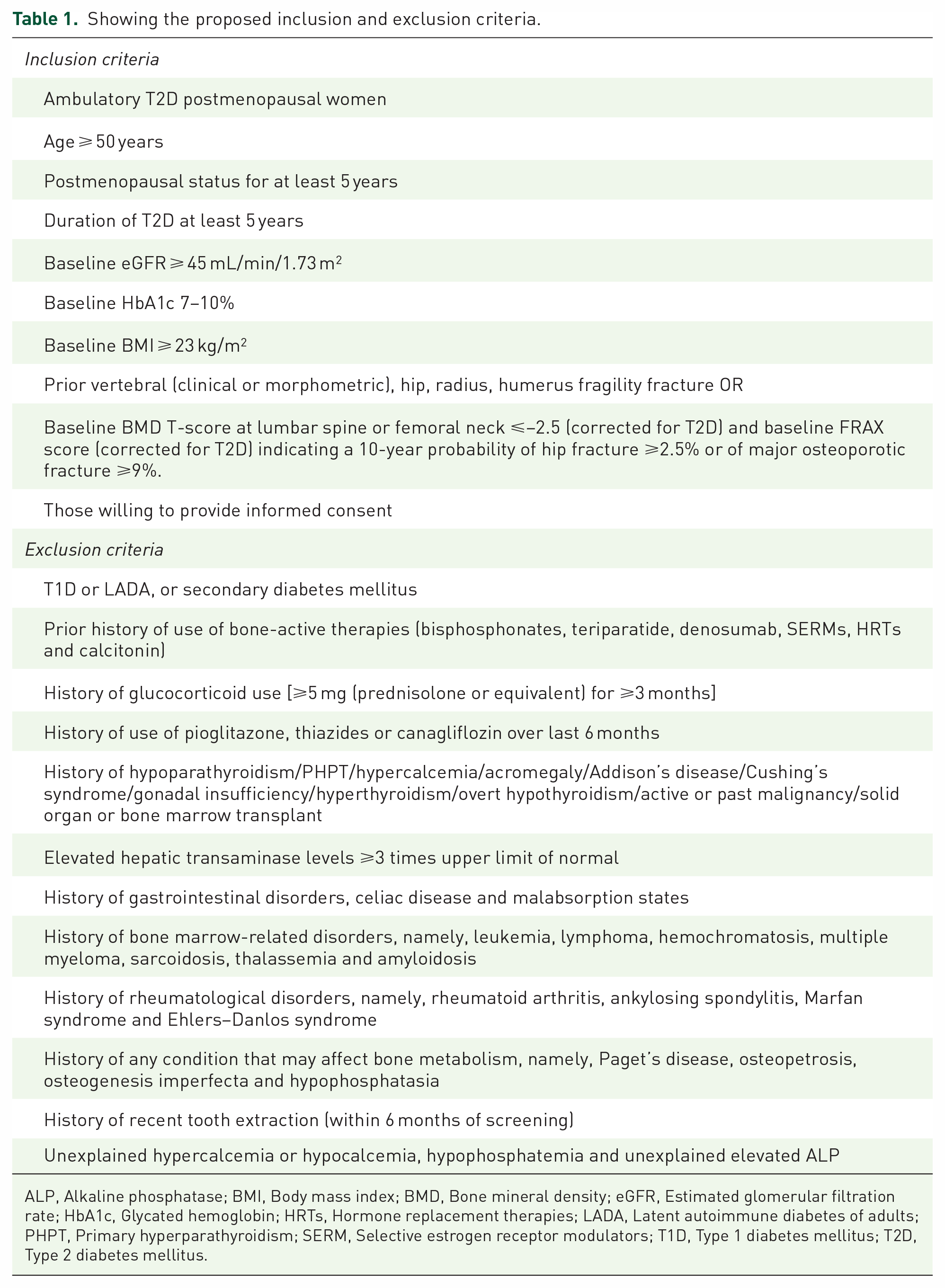
ALP, Alkaline phosphatase; BMI, Body mass index; BMD, Bone mineral density; eGFR, Estimated glomerular filtration rate; HbA1c, Glycated hemoglobin; HRTs, Hormone replacement therapies; LADA, Latent autoimmune diabetes of adults; PHPT, Primary hyperparathyroidism; SERM, Selective estrogen receptor modulators; T1D, Type 1 diabetes mellitus; T2D, Type 2 diabetes mellitus.
Baseline blood investigations
After the screening, all supposedly eligible subjects will undergo additional blood investigations after an overnight fast that will include fasting plasma glucose (FPG), postprandial plasma glucose (PPPG), serum total calcium, inorganic phosphate, total alkaline phosphatase (ALP), liver function test, plasma intact parathyroid hormone (iPTH) and plasma 25-hydroxyvitamin D [25(OH)D]. Serum calcium will be corrected for the corresponding serum albumin levels. Estimation of thyroid function, 8 am cortisol, IgA tissue transglutaminase (IgA tTg) and serum protein electrophoresis will be carried out to rule out relatively common secondary causes of osteoporosis, notably, thyrotoxicosis, exogenous Cushing syndrome, celiac disease and monoclonal gammopathy, respectively. Surplus plasma samples will be preserved at −80°C.
Following these investigations, subjects with unexplained hypercalcemia or hypocalcemia, hypophosphatemia, unexplained elevated ALP and any abnormal blood investigations suggestive of secondary osteoporosis will be excluded. Notably, however, considering the high prevalence of hypovitaminosis D in Asian-Indians,8,9 those with vitamin D deficiency will not be excluded.
Finally, subjects eligible for randomization will be asked to provide informed written consent. They will undergo estimation of bone turnover markers (BTMs), notably, total procollagen type I N-propeptide (PINP) and β-C-terminal telopeptide of type I collagen (β-CTX), using the preserved plasma samples.
The details of the investigations have been summarized in the Supplemental Appendix.
Baseline radiological investigations
Apart from areal BMD, additional radiological investigations will be performed as measures of bone microarchitecture. Accordingly, all eligible subjects will undergo measurement of lumbar spine trabecular bone score (TBS), an indirect measure of the microarchitecture of bone, from each spine DXA examination using the TBSiNsight Software version 3.0.3.0 (Medimaps, Merignac, France). The following cut-offs proposed in the literature for TBS values in postmenopausal women will be considered: Normal: TBS of ⩾1.350; Partially degraded microarchitecture: TBS between 1.200 and 1.350 and Degraded microarchitecture: TBS ⩽1.200. 10
In addition, all eligible subjects will also undergo high-resolution peripheral quantitative computed tomography (HR-pQCT) scan of the non-dominant arm (distal radius) and leg (distal tibia) using the second-generation XtremeCT II scanner (Scanco Medical, Bruttisellen, Switzerland). The process of acquisition of the scan has been described in the Supplemental Appendix.
The following outcomes were recorded at distal sites: total vBMD (Tt.vBMD, mgHA/cm3); trabecular vBMD (Tb.vBMD, mgHA/cm3), trabecular bone volume fraction (Tb.BV/TV, %), thickness (Tb.Th, mm), number (Tb.N, 1/mm) and separation (mm) and cortical vBMD (Ct.vBMD, mgHA/cm3), area (Ct. Ar, mm2), thickness (Ct.Th, mm), porosity (Ct.Po, %) and porosity diameter (Ct.Po.Dm, mm).
Bone strength will be estimated from the HR-pQCT images using Scanco Medical’s finite element analysis (FEA) software. The following outcomes will be recorded at both the distal sites: stiffness (N/mm), failure load (F.Load) (N), apparent Young modulus measured for the whole bone structure (E.app) (MPa), trabecular bone estimated strain (Tb.ES) and cortical bone estimated strain (Ct.ES)
All radiological data will be stored in a central database and interpreted at the end of the trial by a single experienced radiologist.
Baseline assessment of sarcopenia and falls
Type 2 diabetes mellitus is often associated with sarcopenia, which increases the risks of osteoporosis and bone fragility.11,12 Hence, all eligible subjects would undergo an assessment of muscle strength and muscle mass as measures of sarcopenia. Muscle strength will be assessed using dominant handgrip strength measured by the Jamar Plus Digital Hand Dynamometer (Jamar®, Patterson Medical). The subjects will be advised to press on the handle as tightly as possible for 3–5 s each time. Handgrip strength will be measured three times in the dominant arm. A rest period of at least 1 min between two serial measurements on the same arm will be given. The maximum reading obtained will be considered as the final result. 13
Muscle mass will be measured as a part of the body composition assessment acquired by the DXA scanner. For assessing sarcopenia, muscle mass will be expressed as appendicular skeletal muscle mass index, calculated as the sum of lean mass at arms and legs in kilograms divided by the square of height in meters. 13
Diabetes increases the risk of falls, increasing risk of fractures. Hence, assessing the risk of falls is an integral part of evaluating bone fragility in people with T2D. Accordingly, the self-reported FRAS (Falls risk assessment score) questionnaire will be used to calculate the risk of falls at baseline. The details of the FRAS questionnaire have been included in the Supplemental Appendix. A cumulative score of ⩾3.5 predicts a high risk of falls with a sensitivity of 96.2% and a specificity of 86%. 14
Run in phase
Once informed written consent is obtained, and baseline assessments are complete, all eligible participants will undergo a 2-week run in phase. All participants without vitamin D deficiency [25(OH)D ⩾30 ng/mL] will be started on oral calcium (1000 mg elemental calcium/day) and cholecalciferol supplementation (1000 IU/day). Participants with hypovitaminosis D [25(OH)D <30 ng/ml] will be started on oral calcium (1000 mg elemental calcium/day) supplementation. In addition, they will initially receive bolus cholecalciferol supplementation (oral nanodroplet formulation) at a dose of 60,000 IU once daily for seven consecutive days (total dose of 420,000 IU). This modified bolus dosing protocol has been adopted to ensure rapid correction of circulating vitamin D levels as bolus cholecalciferol doses ⩾300,000 IU provide optimal changes in circulating 25(OH)D and parathyroid hormone concentrations. 15 After 1 week of bolus vitamin D, they will be shifted to cholecalciferol doses of 1000 IU/day while calcium supplementation will be continued.
Randomization and drug administration
After 2 weeks of the run in phase, all eligible participants will be randomized in a 1:1:1:1 ratio to either of the four treatment arms:
Arm A: intravenous zoledronic acid 5 mg annually
Arm B: subcutaneous denosumab 60 mg biannually
Arm C: subcutaneous teriparatide 20 mcg daily
Arm D (control arm): only standard of care (daily calcium and cholecalciferol).
Participants will receive the randomized drug without blinding for 72 weeks (two doses of zoledronic acid, four doses of denosumab, 72 weeks of teriparatide). In addition, participants in Arms A, B, and C will also receive standard of care throughout the study duration.
Randomization will be carried out by block randomization using a computer-generated program. The block size will be documented in the clinical trial report. Sequentially numbered, sealed opaque envelopes will be used to conceal allocation, which will be revealed to the participants only by Trupti Nagendra Prasad (TNP). Subsequent drug administration as per schedule will also be carried out only by TNP.
TNP will administer zoledronic acid and denosumab at the outpatient clinic. The technique of administration of teriparatide will be demonstrated by TNP at the time of treatment allocation and participants will be asked to self-administer the drug daily at home. Compliance will be ensured by teriparatide cartridge counting. Calcium (as tablets) and cholecalciferol (as soft gel capsules) will also be dispensed by TNP at treatment allocation and thereafter at each subsequent visit. Compliance will be monitored by counting the blister packs.
All other investigators will be blinded to the process of treatment allocation.
The study design has been summarized in Figure 1.

Study design showing participant eligibility, recruitment and treatment allocation.
Endpoints
The primary endpoint will be the change in areal BMD at the lumbar spine and femoral neck at the end of 72 weeks. The co-primary endpoint will be the frequency of clinical major osteoporotic fractures (fragility) and/or morphometric vertebral fractures (fragility) during the study. The secondary endpoints will include the change in BMD at the distal one-third radius, TBS, HR-pQCT parameters, and BTMs at the end of 72 weeks. In addition, interim exploratory endpoints will include the change in HR-pQCT parameters and BTMs at 24 weeks following treatment allocation.
Besides efficacy, safety endpoints will also be assessed. The following adverse events will be pre-specified as being of special interest based on pre-existing data on anti-osteoporotic drugs, notably, acute phase response (fever, chills, myalgia, arthralgia, headache, influenza-like symptoms), hypersensitivity, renal injury, atypical femoral fractures, osteonecrosis of the jaw, atrial fibrillation, acute uveitis, hypocalcemia (symptomatic or biochemical), hypophosphatemia (symptomatic or biochemical), hypercalcemia (symptomatic or biochemical), dermatological reactions and orthostatic hypotension.
Assessments and schedule
Following the run in phase and the treatment allocation (week 0), participants will be followed up at 6, 12, 24, 36, 48, 60 and 72 weeks. To ensure participant retention and complete follow-up, we will keep in periodic telephonic contact with the participants. Follow-up will be carried out by investigators (other than TNP) who will be blinded to the randomization and treatment allocation process. Endpoint assessors will refrain from inquiring about the nature of the anti-osteoporotic drug received. At each visit, a medical history will be sought inquiring about any incident clinical fractures, new-onset backache or any pre-specified adverse effects. Any other adverse events will also be recorded.
Blood investigations, namely, FPG, PPPG, serum calcium, inorganic phosphate, ALP, renal function test, 25(OH)D, PINP and β-CTX will be repeated at 6, 24, 48, 60 and 72 weeks after a full overnight fast. HbA1c will be repeated only at 24, 48 and 72 weeks. Of note, blood investigations will be performed before the subsequent dose of zoledronate and denosumab. With regard to radiological investigations, DXA, TBS and radiograph of the lumbar spine will be repeated only at the end of 72 weeks. HR-pQCT will be repeated twice at 24 and 72 weeks. As with the baseline investigations, all radiological data will be stored in a central database to be interpreted at the end of the trial.
As part of the study protocol, the investigators can prescribe rescue medication for hyperglycemia for participants with HbA1c >7.5% at follow-up. Any glucose-lowering drugs may be used for glycemic rescue except pioglitazone and canagliflozin, which will be noted on follow-up.
Statistical analysis
Being a pilot study and in the absence of sufficient data on the effect of anti-osteoporotic drugs on BMD, specifically in people with T2D, we will not undertake any formal sample size calculation. Nevertheless, the law of large numbers holds that the central limit theorem is valid as random samples become large enough, usually defined as an n ⩾ 30. 16 Hence, we will select a sample size of 30 in each group. To account for a dropout rate of around 15%, we will finally consider a sample size of 35 in each group with a total of 140 to detect a significant difference in primary outcome, that is, change in areal BMD between any two groups at 80% power of study and 95% confidence interval (alpha level of 5%).
The primary endpoint will be evaluated as per-protocol analysis, with participants who have completed 72 weeks of follow-up and have had two DXA scans performed being the only ones included. Similarly, the secondary endpoints will also be evaluated as per-protocol analysis. Adverse events and laboratory data will be analysed for all randomized patients who will receive at least one dose of the drugs. Adverse events will be classified using the current version of the Medical Dictionary for Drug Regulatory Activities. The analyses will be purely descriptive.
Study oversight
The study will be overseen by the coordinating investigator (RP), who will coordinate with all other investigators involved in the study. No external/contract research organizations will be involved in the study. Funding organizations will have no access to the study data. Confidentiality of the data will be ensured. The final trial dataset for statistical analysis will be accessible to the coordinating investigator (RP) and statistician (AK).
The study recruitment began on 5 February 2022. Recruitment has been carried out in a staggered fashion till 4 October 2022. Each participant will be followed for 72 weeks, with the last study follow-up scheduled on 3 April 2024.
Ethics and dissemination
The trial will be conducted according to the ethical principles of the Declaration of Helsinki and in accordance with the Guideline for Good Clinical Practice from the International Conference on Harmonization.
We plan to submit the trial results to conferences and peer-reviewed journals. All study investigators will be eligible for authorship. No professional writers will be involved. Study results will not be individually informed to the trial participants.
Discussion
The proposed study is the first ever RCT primarily designed to evaluate the efficacy of the commonly available anti-osteoporotic drugs, namely, zoledronate, denosumab and teriparatide, in postmenopausal women with T2D. The results of the study will help guide the management of diabetic bone disease, which, hitherto, is mainly based on evidence drawn from the non-diabetic population.
People with diabetes mellitus are at a high risk of low-trauma vertebral and non-vertebral fractures, with fracture risk being higher in T1D than T2D. Surprisingly, people with T2D have either normal or higher BMD than age- and sex-matched non-diabetic controls. The apparent paradox between increased BMD and high fracture risk is explained by deteriorated bone microarchitecture.1,5 The Framingham HR-pQCT study reported that people with T2D had lower cortical vBMD, higher cortical porosity and smaller cross-sectional area only at the tibia. Trabecular indices were similar or more favourable in T2D than in non-T2D. 17 Nevertheless, very recent data suggest that trabecular bone is no less affected in T2D. 4
The pathogenesis of bone disease in diabetes is multifactorial and many possible mechanisms have been postulated. One involves the excessive formation of advanced glycation end products (AGEs). ACE accumulation in bone leads to collagen cross-linking that reduces osteoblast adhesion to the bone matrix, and diminishes alkaline phosphatase activity in mature osteoblasts. Besides, activation of receptor for AGE (RAGE) on pre-osteoclasts leads to the generation of cytokines and reactive oxygen species promoting osteoclastogenesis and inhibiting osteoblastogenesis. 6 Estimation of BTMs has revealed that bone remodeling is reduced in people with T2D. Reduction in bone remodeling compromises the healing of micro-fractures in mechanically loaded bones; accumulation of micro-fractures may predispose people with diabetes to fragility fractures.
Considering the peculiarities of bone disease in T2D, it is intriguing if its pharmacotherapy differs from routine postmenopausal osteoporosis. Notably, the use of bisphosphonates, the most commonly used anti-osteoporotic agent in postmenopausal osteoporosis, in a state of low bone turnover as in T2D, might be of potential concern. Hitherto, no RCTs have directly evaluated the anti-fracture efficacy of osteoporosis treatment in people with T2D as a primary pre-specified endpoint.5,18
In a post hoc analysis of the landmark Fracture Intervention Trial that had included 297 postmenopausal women with T2D, Keegan et al. reported that diabetes did not alter the effect of alendronate on BMD gain versus placebo. 19 Likewise, risedronate showed similar responses on lumbar spine BMD and BTMs between osteoporotic subjects with (n = 53) or without diabetes (n = 832). 20 In another open-label prospective study, oral ibandronate at a dose of 150 mg/month for 1 year resulted in a similar increase in BMD at the lumbar spine, femoral neck and total hip in osteoporotic postmenopausal women with (n = 49) or without diabetes (n = 55). 21 As far as parenteral bisphosphonates are concerned, there are no published data on the effect of BMD or fracture risk in people with T2D with the use of pamidronate or zoledronate.
In a sub-analysis of the placebo-controlled FREEDOM trial (Fracture REduction Evaluation of Denosumab in Osteoporosis every 6 months) and its 7-year extension, the rate of vertebral fracture was significantly lower with denosumab (n = 266) compared with placebo (n = 242) in people with diabetes mellitus (1.6% versus 8.0%). On the contrary, the rate of non-vertebral fractures was higher in the denosumab group than in the placebo group (11.7% versus 5.9%). 22
With regard to osteoanabolic agents, the effect of teriparatide administered at a standard dose of 20 μg/day (for up to 24 months) was assessed in patients with and without T2D in the post hoc analyses of the DANCE observational study (Direct Analysis of Non-vertebral Fractures in the Community Experience). For spine and total hip BMD, teriparatide treatment had a similar effect in people with (n = 291) and without diabetes mellitus (n = 3751). The incidence of non-vertebral fractures at 6 months was similar in both groups. 23 In a post hoc analysis of the ACTIVE (Abaloparatide Comparator Trial in Vertebral Endpoints) trial, 198 women with postmenopausal osteoporosis and T2D were identified. At 18 months, abalaparatide significantly improved BMD at the total hip, femoral neck and lumbar spine and TBS at the lumbar spine versus placebo. Non-vertebral fractures were significantly lower with abaloparatide compared to placebo (p = 0.04). 24
Thus, the aforementioned data reinforce that, until now, there are no RCTs that have evaluated the efficacy and safety of anti-osteoporosis drugs as a primary endpoint in people with T2D. No RCTs have compared the available anti-osteoporotic drugs in a head-to-head fashion in people with T2D. Besides, most of the available studies (post hoc/subgroup analyses of RCTs) have included people with osteoporosis (based only on BMD) rather than people with fragility fractures. Moreover, in all the available studies, only individuals with osteoporosis (as defined classically by T-score ⩽−2·5) were included; nevertheless, since people with T2D tend to have a higher BMD, osteoporosis in T2D sets in at a T-score of −2.0. Hence, for evaluating the efficacy of anti-osteoporotic therapies in T2D, subjects with a T-score ⩽−2.0 should be ideally recruited. Furthermore, some of the available data are only restricted to changes in BMD rather than prevention of incident fractures (considered a more hardcore endpoint while evaluating the efficacy of osteoporosis treatment). 5
Considering the striking lacunae in the literature, we plan to conduct the proposed study to bridge the aforementioned knowledge gaps. We will recruit only postmenopausal women with T2D with a diabetes duration of at least 5 years as the risk for fractures increases with a diabetes duration of >5 years. 18 We will include subjects with fragility fractures and/or low T-score and high FRAX® score. We will take a T-score cut-off of −2.0 rather than −2.5, consistent with the fact that osteoporosis in T2D begins at a T-score of −2.0. In addition, the stringent exclusion criteria will ensure that secondary causes of bone fragility (other than diabetes) are diligently ruled out and do not affect the study results. Besides, we will estimate muscle strength, muscle mass and risk of falls at baseline, all of which can affect bone fragility in people with T2D and, subsequently, the efficacy of anti-osteoporotic medications.
To assess bone health, we will perform TBS and HR-pQCT as measures of bone microarchitecture. Since T2D affects bone microarchitecture more than bone mass, assessment of skeletal microarchitecture is expected to yield more meaningful results regarding the efficacy of anti-osteoporotic drugs. Besides, bone strength, measured as stiffness and failure load using FEA, will further provide robust insight into the efficacy of the anti-osteoporotic drugs. Nevertheless, since efficacy is usually equated in terms of an increase in BMD and/or reduction in fracture risk, the primary endpoint will consist of a change in the lumbar spine and femoral risk BMD, while the co-primary endpoint will cater to incident fragility fractures. Changes in bone microarchitecture and bone strength will be evaluated as secondary endpoints.
In conclusion, the proposed RCT plans to evaluate the efficacy of anti-resorptive (zoledronate or denosumab) or osteoanabolic (teriparatide) therapies in postmenopausal women with T2D. The trial, with its unique inclusion criteria, is expected to provide knowledge regarding the best anti-osteoporotic drug in a low turnover state like T2D. The proposed trial’s results will fill a noticeable void in the existing literature.
Supplemental Material
sj-doc-1-tae-10.1177_20420188231207516 – Supplemental material for Efficacy of zoledronate, denosumab or teriparatide in postmenopausal women with type 2 diabetes mellitus at high risk of fragility fractures: protocol of an open, blinded endpoint randomized controlled pilot trial
Supplemental material, sj-doc-1-tae-10.1177_20420188231207516 for Efficacy of zoledronate, denosumab or teriparatide in postmenopausal women with type 2 diabetes mellitus at high risk of fragility fractures: protocol of an open, blinded endpoint randomized controlled pilot trial by Trupti Nagendra Prasad, Sanjay Kumar Bhadada, Veenu Singla, Neelam Aggarwal, Sant Ram, Uttam Chand Saini, Ashok Kumar and Rimesh Pal in Therapeutic Advances in Endocrinology and Metabolism
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.