
Abstract
Background:
Inflammations are the crucial pathogenesis of chronic complications of type 2 diabetes mellitus (T2DM).
Objectives:
The timeline of cardiovascular and renal complications of T2DM and whether soluble tumor necrosis factor receptor type 1 (sTNFR1) levels predict cardiorenal outcomes were still elusive.
Design:
Prospectively observational study.
Methods:
Chinese patients with T2DM were enrolled. Cardiorenal composite events defined by either cardiovascular composite events (all-cause mortality, acute coronary syndrome, or non-fatal stroke) or renal composite events (a decline of >30% of renal function or worsening status of albuminuria) were followed. Associations of sTNFR1 levels and cardiovascular, renal, and cardiorenal composite events were analyzed in regression models presented by hazard ratio (HR) and 95% confidence interval (95% CI).
Results:
Among 370 subjects, 42 cardiovascular and 86 renal composite events occurred. Higher sTNFR1 levels were related to higher frequency and risks of cardiovascular composite events (HR 1.07, 95% CI 1.01–1.13, p = 0.009) and renal composite events (HR 1.05, 95% CI 1.02–1.09, p < 0.001). Occurrences of cardiovascular composite events were not predicted by precedential renal composite events. sTNFR1 levels were proved to be associated with risks of cardiorenal composite events in Cox regression sequential models (adjusted HR 1.04, 95% CI 1.00–1.08, p = 0.03). The results were consistent in all subgroup analyses.
Conclusion:
Levels of sTNFR1 were associated with cardiorenal complications of T2DM and the predictabilities of TNFR1 levels were better than precedential cardiovascular or renal events.
Keywords
Introduction
Type 2 diabetes mellitus (T2DM) is a highly prevalent non-communicable disease worldwide and the numbers of patients as well as the burdens of the complications are growing.1–3 Both macrovascular and microvascular complications had great impact on the prognosis of the subjects with T2DM. The risks of cardiovascular diseases increase 2–4 folds in people with T2DM comparing with non-diabetic ones and one-third to half of subjects with T2DM died of cardiovascular disease.4,5 Furthermore, 30–50% of subjects with T2DM were complicated with diabetic kidney disease (DKD) and the DKD is still the dominant etiology of end stage renal disease and associated with worse prognosis of diabetic subjects.6,7 Moreover, the experiences of cardiovascular disease and declines of renal functions were the risk factors of each other and the bi-directional associations can be concluded by previous reports.8,9 Except the loss of quality and quantity of life, the costs of therapies for vascular complications of T2DM contributed to more than half of expenses for diabetic care. 10 Therefore, the method which stratified the risk precisely then introduced appropriate intervention for preventing complications of T2D as early as possible is exigent.
Soluble tumor necrosis factor receptor type 1 (sTNFR1) level is one of the biomarkers which represents the status of systemic inflammation. The inflammatory reaction is one the important pathogenesis of vascular complications of T2D.11,12 sTNFR1 levels predict the occurrences of end stage renal disease and cardiovascular disease in independent cohorts composed of subjects with T2DM.13,14 However, whether sTNFR1 levels predicted cardiovascular and renal complications simultaneously among subjects with T2DM were still elusive. Besides, even the renal functions at baseline were related to the risks of cardiovascular events and the history of cardiovascular disease was associated with renal outcomes, whether occurrences of renal events can predict cardiovascular outcomes and precedential cardiovascular events can be a predictor of renal complications in diabetic cohort should be clarified.
The purpose of the study was to explore whether levels of sTNFR1 were associated with cardiorenal outcomes and to investigate whether precedential cardiovascular or renal events can predict consequences of renal or cardiovascular complications in subjects with T2DM.
Material and methods
Recruitment of patients
We conducted a prospectively observational study since June 2014 and the purpose of the study was to explore the associations of clinical or biological markers and the outcomes of patients with T2DM. The design of this study was compliant to the guide of Strengthening the Reporting of Observational Studies in Epidemiology (STORBE). Subjects who were confirmed to be T2DM as well as agreed with their participation were recruited after completing informed consents. Those with severe impairment of renal function [estimated glomerular filtration rate (eGFR) <30 mL/min/1.73 m2], hepatitis with unknown cause, and hemoglobin A1c (HbA1c) more than 9% were excluded from the study. The comprehensive evaluations for clinical characteristics, demographic or anthropometric markers, co-morbidities, and current medications of participating subjects were conducted in the first visit of the study. The comorbidities were identified by reviewing the electronic medical records of participants which were conducted in Taipei Veteran General Hospital. The sodium glucose cotransporter type 2 inhibitor (SGLT2i) was firstly confirmed as a modifier of DKD which reduced the risk of worsening nephropathy in subjects with T2DM in 2016. 15 Therefore, the introductions of SGLT2 inhibitor for the participants among the periods of observations were also record. The samplings of biochemical markers relevant to diabetic outcomes were proceeded with immediately after the first visit. The tests of creatinine of serum as well as spot urine and albumin of spot urine were conducted in the first visit and repeated per 6 months. The sTNFR1 levels of baseline were measured by commercial human ELISA kit (Cat. No.:DRT 100, Quantikine ELISA, MN, USA) according to the instructions from the manufacturer. The limit of detectable level of sTNFR1 was approximately 0.8 pg/dL while the variations of the assay were about 3–8%.
Follow-up of cardiovascular, renal, and cardiorenal events
Composite events of cardiovascular disease, including all-cause mortality, acute coronary syndrome, or non-fatal stroke, were identified according to the diagnoses of the discharge summaries of recruited subjects. The cause of death was determined by the first diagnosis of the discharge summary when the subject died during the period of hospitalization. The acute coronary syndrome was defined as a myocardial infarction or unstable angina which was necessary to be intervened by the cardiologist with the procedure of percutaneous coronary arterioplasty sequentially. A Non-fatal stroke was defined by the ischemic insult of the parenchyma of brain or brain stem rather than hemorrhagic one and the event was confirmed by the neurologist according to symptoms, neurological examination, and radiological studies. The renal composite events were composites of either a more than 30% of decline of eGFR or worsening status of albuminuria. The results of eGFR were calculated by the method of Modification of Diet in Renal Disease. 16 The decline of eGFR should be confirmed by the consistent result which was tested 6 months later to the first appearance of a > 30% drop of eGFR. The status of albuminuria was determined by the result of urinary albumin-creatinine ratio (UACR) of baseline. The progressive switches of status of albuminuria, including from normo- to micro-albuminuria (increasing UACR levels from <30 mg/g creatinine to 30–300 mg/g creatinine), micro- to macroalbuminuria (elevated UACR levels from 30 to 300 mg/g creatinine to >300 mg/g creatinine), or normo- to macroalbuminuria, were considered as the worsening status of albuminuria.17,18 Due to the fluctuations of UACR levels time by time, the progressive shifts should be validated by the repeated tests of UACR 6 months post to prior exam. The cardiorenal composite events were recognized as the first occurrence of any aforementioned composites of either cardiovascular or renal events.
Statistics
The analyses of variance were the methods to find the differences of values of continuous variables and Pearson’s chi-squared tests were used for comparisons of the categorical variables across the groups with and without cardiorenal composite events. The cumulative events-free probabilities of cardiovascular, renal, or cardiorenal composite events across the levels of sTNFR1 were calculated by Kaplan–Meier analyses and a p value of Log-Rank test <0.05 was interpreted as significant. The relevant factors of cardiovascular and renal composite events were identified by the Cox proportional hazard analyses. The associations of sTNFR1 levels and the risks of either cardiovascular or renal composite events were confirmed by adjusting all other factors associated with cardiovascular or renal outcomes in Cox regression analyses. After confirming sTNFR1 levels were relevant to cardiovascular and renal composite events, three Cox regression sequential models were used for confirming the associations between sTNFR1 levels and cardiorenal composite events. The first model contained the factors of age and gender then the factor of duration of diabetes were further added in model 2. Model 3 contained above factors and all other biologically or statistically relevant factors which were associated with cardiovascular or renal outcomes in this study. Above analyses were conducted with IBM SPSS software 18.0 (IBM, Armonk, New York, USA). For further estimating the effect of using SGLT2i on cardiovascular, renal, and cardiorenal outcomes, the time-varying Cox regression model was conducted. The use of SGLT2i was recognized as a time-dependent variable whereas other relevant factors were input as fixed covariates. 19 The software of SAS (version 9.4, SAS Institute; Cary, NC, USA) was used for analyses of time-varying Cox regression model.
Results
Baseline characteristics
Three hundred seventy-one subjects were recruited in this study and the median period of follow-up was 45 months. One subject was excluded due to the level of HbA1c more than 9% at baseline. Eight participants were dead and twenty-six subjects were lost to follow-up during the period of observation (Figure 1). The mean age of our cohort was 61.2 years old and the duration of diabetes was about 11 years. Hypertension and hyperlipidemia were the leading co-morbidities in this cohort. Twenty percent of subjects had a history of coronary artery disease and six subjects were diagnosed as having had heart failure before the entry of this analysis. The prevalence rate of microvascular complications of T2DM other than DKD was 10%. The existence of albuminuria accounted for 34% of recruited patients and the portion of chronic kidney disease (CKD) stage 3 or above was 20%. Ten percent of subjects had albuminuria as well as eGFR less than 60 mL/min/1.73 m2. Five subjects had histories of severe hypoglycemia. The managements of hyperglycemia and hypertension were relatively acceptable. For essential medicines associated with cardiovascular or renal outcomes, 50–60% of the subjects received RAS inhibitors or statins and 20% individuals of the total cohort were treated by anti-platelet therapy. Eighty-two users of SGLT2i were identified in this cohort. Three subjects were treated by SGLT2i before the beginning of the observation and SGLT2i were initiated in 79 subjects after the entry of the study. The median period of using SGLT2i was 23 months. Three subjects were treated by analogues of glucagon-like peptide-1 (GLP1a; Table 1).
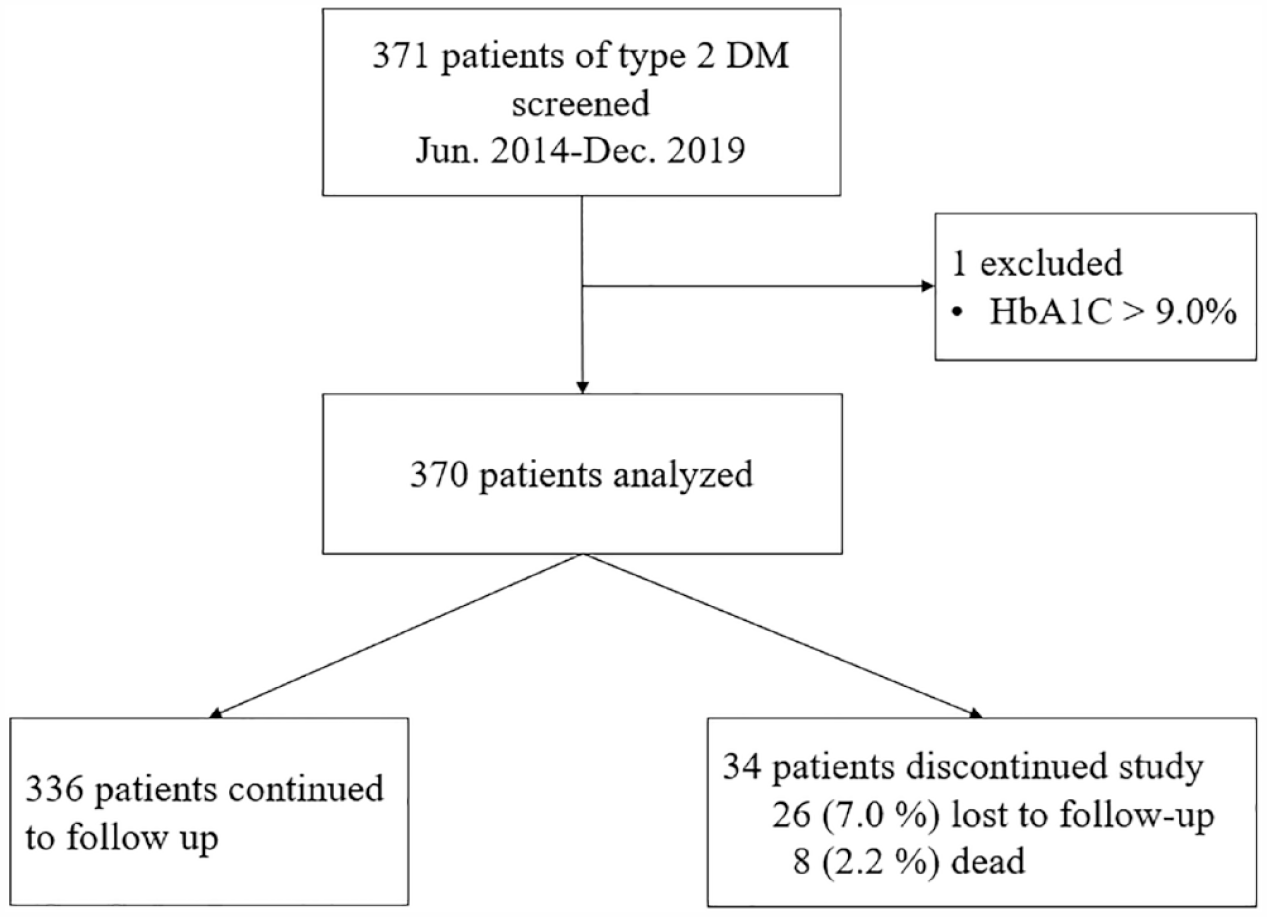
Patient disposition.
Baseline characteristics of subjects with type 2 diabetes grouped by the occurrence of cardiorenal events or not.

Data are expressed as numbers and percentage in non-continuous variables and mean ± SD in continuous variables.
p < 0.05 was defined as significant difference among two groups.
CKD, chronic kidney disease; eGFR, estimated glomerular filtration rate; GLP-1, glucagon like peptide-1; HbA1c, hemoglobin A1C; SGLT2, sodium glucose cotransporter type 2; sTNFR1, soluble tumor necrosis factor receptor type 1.
Associations of sTNFR1 and cardiovascular or renal events
Among our cohort, 42 cardiovascular composite events and 86 renal composite events occurred till January 2022. Eight subjects died during the period of follow. One of them died due to cardiovascular cause, one died of the infection of respiratory tract, as well as others died of malignancy. The acute coronary syndrome was the major component of the cardiovascular composite events (28 of 42 cardiovascular composite events; Table 1). The third tertile of sTNFR1 levels were associated with the highest risks of the cardiovascular composite events [p < 0.001 by log-rank test; Figure 2(a)]. After adjusting other crucial factors, the association of sTNFR1 levels and cardiovascular composite events were proved by Cox regression analyses [adjusted hazard ratio (HR) 1.07, 95% confidence interval (CI) 1.01–1.13, p = 0.009; Table 2]. Among the renal composite events, 72% of them were worsening status of albuminuria. The highest tertile of sTNFR1 levels were also related to the greater numbers of the renal composite events [p < 0.001 by log-rank test, Figure 2(b)]. The Cox regression analyses indicated sTNFR1 levels were an independent factor to predict the occurrences of renal composite events (adjusted HR 1.05, 95% CI 1.02–1.09, p < 0.001; Table 2). The Use of SGLT2i was not associated with cardiovascular or renal outcomes in our cohort (HR 0.85, 95% CI 0.39–1.84, p = 0.68 for cardiovascular events; HR 1.15, 95% CI 0.70–1.88, p = 0.57 for renal events). The results were consistent in time-varying Cox regression model (HR 0.29, 95% CI 0.04–2.18, p = 0.23 for cardiovascular events; HR 0.82, 95% CI 0.32–2.05, p = 0.67 for renal events). The mean periods of the occurrences of cardiovascular composite events were not different from these of renal composite events (29.7 months for cardiovascular composite events versus 32.2 months for renal composite events, p = 0.51 by analyses of variance). The results of Cox regression analyses showed borderline associations between occurrences of cardiovascular composite events and risks of renal composite events (HR 1.80, 95% CI 1.04–3.10, p = 0.03) but the associations between occurrences of renal composite events and risks of cardiovascular composite events were not significant (HR 1.73, 95% CI 0.92–3.24, p = 0.08).

Kaplan–Meier curve showing the probability of cumulative events-free survival of cardiovascular (a), renal (b), and cardiorenal composite events (c) in patients with type 2 diabetes mellitus divided into groups based on concentration tertiles of sTNFR1.
Result of univariate and multivariate Cox proportional hazard model for association of the levels of sTNFR1 with cardiovascular, renal, and cardiorenal composite events.

Model 1: adjusted with age and gender. Model 2: adjusted with age, gender, and duration of diabetes. Model 3: adjusted with all factors relevant to cardiovascular or renal composite events.
Adjusted with factors associated with cardiovascular composite events.
Adjusted with factors associated with renal composite events.
CI, confidence interval; Cr, creatinine; DPP4, dipeptidyl peptidase-4; eGFR, estimated glomerular filtration rate; HR, hazard ratio; RAS, renin-angiotensin system; sTNFR1, soluble tumor necrosis factor receptor type 1; UACR, urinary albumin-creatinine ratio.
Associations of sTNFR1 and cardiorenal events
One hundred eleven cardiorenal composite events occurred within the period of follow-up. Subjects with the cardiorenal events were elder and had higher portions of existed coronary artery disease, albuminuric, and non-albuminuric CKD than those free from cardiorenal composite events (Table 1). The higher concentrations of sTNFR1 were related to lower cumulative events-free probabilities of cardiorenal composite events in Kaplan–Meier analyses [p < 0.001 by Log-Rank test, Figure 2(c)]. The levels of sTNFR1 were associated with the risks of cardiorenal composite events and the associations were persistent after adjusting with other factors related to cardiovascular or renal composite events in Cox regression sequential models (Model 1: HR 1.06, 95% CI 1.03–1.09, p < 0.001; Model 2: HR 1.05, 95% CI 1.03–1.08, p < 0.001; Model 3: HR 1.04, 95% CI 1.00–1.08, p = 0.03; Table 2). The Cox regression model showed the cardiorenal outcomes of our subjects were not influenced by using SGLT2i or not (HR 1.12, 95% CI 0.72–1.37, p = 0.61) and the result were not changed in time-varying Cox regression model (HR 0.78, 95% CI 0.34–1.89, p = 0.57). In subgroup analyses, the associations of sTNFR1 levels and occurrences of cardiorenal composite events were consistent among subjects older or younger than 60 years old, male or female, with or without documented coronary artery disease, being eGFR more than 60 mL/min/1.73 m2 or not, being albuminuric or non-albuminuric, users and ono-users of RAS blockades, and uses of SGLT2i or not (Table 3).
Results of association of the sTNFR1 levels and cardiorenal composite events stratified by age, sex, duration of diabetes, history of coronary artery disease, eGFR, and the use of RAS inhibitors.

CI, confidence interval; eGFR, estimated glomerular filtration rate; HR, hazard ratio; RAS, renin-angiotensin system; SGLT2; sodium glucose co-transporter type 2; UACR, urinary albumin-creatinine ratio.
Discussion
Our cohort composed of Chinese subjects with T2DM showed sTNFR1 levels were related to cardiovascular and renal outcomes then furtherly demonstrate sTNFR1 was a potential biomarker to predict cardiorenal outcomes. The predictability of sTNFR1 levels for cardiovascular and renal outcomes were better than precedential cardiovascular or renal events in subjects with T2DM.
Our results highlighted the implications of sTNFR1 levels by following reasons. The first, the associations of sTNFR1 levels and cardiorenal composite events were persistent after adjusting traditionally non-modifiable risk factors, such as age, duration of diabetes, renal function at baseline, and history of vascular complications. Second, the associations remain even the managements of modifiable risk factors, such as blood pressure and glycemia, were relatively optimal according to the results of clinical investigations and the suggestions from the clinical guideline.20–22 The interventional study and analysis of net-work model of the active agent also supported sTNFR1 rather than HbA1c might be the target of reversing the pathogenesis of complications of T2DM.23,24 The aforementioned messages notified the crucial role of sTNFR1 levels in generating and predicting risks of cardiovascular or renal complications in subjects with T2DM other than traditional biomarkers. Third, the associations were consistent across the subjects with or without history of cardiovascular or signs of renal complications in our study. The previous reports showed inconsistent conclusions about the predictability of sTNFR1 levels for cardiovascular and renal outcomes in subjects with stable coronary artery disease or advanced CKD versus subjects without apparent signs of cardiovascular or renal complications.14,25–28 The discrepancies might be originating from the differences of characteristics of participants or definitions of outcomes. Our cohort enrolled the subjects with and without cardiovascular or renal complications at baseline. Therefore, the subgroup analyses and results of regression models in our study supported that the associations between sTNFR1 levels and cardiovascular as well as renal outcomes can be generated for both diabetic subjects with and without documented cardiovascular or renal disease.
Whether the occurrence of renal complication was a risk factor or only a marker of the cardiovascular outcome in subjects with T2DM was still a debatable issue. 29 The precedential microvascular complications were recognized as risk factors of cardiovascular disease. 30 However, the pathogenesis of cardiovascular disease was different from that of renal complications of T2DM. The major pathogenic way of cardiovascular disease was related to atherosclerosis but the crucial pathogenesis of renal complications of T2DM was due to cellular injury caused by detrimental effects from glucose-mediated endothelial dysfunction and oxidative stress.31,32 Our study followed cardiovascular and renal outcomes simultaneously rather than defined either one as the target of interest. Therefore, the timeline of renal and cardiovascular complications of T2DM can be clarified in our study. The insufficient power of predictability for cardiovascular outcomes by occurrences of renal composite events and borderline associations between occurrences of cardiovascular composite events and the renal outcomes in our study indicated that the renal and cardiovascular complications did not occur sequentially but should appear simultaneously. Therefore, the managements of subjects with T2DM should include the strategies of macrovascular as well as microvascular protection rather than focus on either one only. 33 In other words, the biomarkers, such as sTNFR1 levels, which were involved in the pathogenesis of both kinds of vascular complications of T2DM were extremely useful predictors before any occurrences of vascular complications in subjects with T2DM
The bioactivities of tumor necrosis factors, which reflected by the levels of sTNFR1, were important factors of chronic inflammation and were involved in the early process of chronic complications of T2DM rather in the terminal cascade.11,34,35 Therefore, it was reasonable to find sTNFR1 levels exhibited better associations with outcomes of subjects with T2DM than occurrences of cardiovascular or renal composite events and to demonstrate the consistent associations among the subjects with or without history of coronary artery disease or signs of renal impairment in our study. Since low-grade inflammation was a common pathway for microvascular and macrovascular complications, the associations between sTNFR1 levels and cardiorenal outcomes in the study proved our results were in line with the pathogenesis of chronic complications of T2DM. 33
Some limitations of our study should be mentioned. First, this was an observational study with modest sample size and all participants were Chinese. The predictability of sTNFR1 levels should be further validated in other prospective studies with greater sample sizes and the results may not be generalizable to other ethnics. Second, not all microvascular or macrovascular complications were set as the observations of interest in our study. Whether increasing levels of sTNFR1 predicted risks of retinopathy, neuropathy, or peripheral vascular disease was unknown. Third, although our study was not the first one to report the associations between sTNFR1 levels and cardiovascular or renal complications of T2DM, there was not yet intervention study to prove the clinical efficacy of mitigating complications by diminishing the activities of tumor necrosis factor. 36 Furthermore, our results can’t be applied to non-dialytic subjects with eGFR less than 30 mL/min/1.73 m2 who were excluded in our study. Fourth, associations between some crucial factors, such as history of severe hypoglycemia and heart failure, was discrepant with previous studies because of few numbers of cases.37,38 However, the burdens of heart failure and hypoglycemic events could be underestimated solely by the reports of the patients or investigators in observational study which was not specifically designed for exploring the fields of heart failure or severe hypoglycemia in diabetic subjects.39,40 Moreover, the ejection fraction of left ventricle was not available in our cohort because this was not a conventional parameter assessed in all subjects with T2DM. Further study should be conducted for evaluating the impact of heart failure and severe hypoglycemia on the cardiorenal outcome in the subject with T2DM. The last, the users of SGLT2i were not at significantly lower risks of cardiovascular, renal, and cardiorenal events in our cohort. The finding could be explained by limited cases of primary cohort, relatively small proportion of users of SGLT2i, selection bias due to observational designs, and unbalanced cardiovascular and renal risks at baseline between subjects with and without the therapies of SGLT2i.
Conclusion
Circulating sTNFR1 were associated with cardiorenal complications of T2DM and the predictability of sTNFR1 levels were better than precedential cardiovascular or renal events.
Footnotes
Acknowledgements
We are grateful to all the members for their contribution to the study. We also thank the Clinical Research Core Laboratory and Medical Sciences & Technology Building of Taipei Veterans General Hospital for providing us with an experimental space and facilities.