
Abstract
Background:
In recent years, many studies have reported the relationship between non-alcoholic fatty liver disease (NAFLD) and sex hormones, especially total testosterone (TT) and sex hormone–binding globulin (SHBG). However, the relationship between sex hormones and the severity of NAFLD is still unclear.
Methods:
PubMed, Embase, Cochrane Library, Web of Science, WanFang, China National Knowledge Infrastructure and VIP databases were searched for relevant studies from inception to 31 August 2021. Values of weighted mean differences (WMDs) and odds ratios (ORs) with their 95% confidence intervals (CIs) were combined by Stata 12.0 software to evaluate the relationship between TT, SHBG and the severity of NAFLD in males.
Results:
A total of 2995 patients with NAFLD from 10 published cross-sectional studies were included for further analysis. The meta-analysis indicated that the moderate-severe group had a lower TT than the mild group in males with NAFLD (WMD: −0.35 ng/ml, 95% CI = −0.50 to −0.20). TT and SHBG were important risk factors of moderate-severe NAFLD in males (ORTT = 0.79, 95% CI = 0.73 to 0.86; ORSHBG = 0.22, 95% CI = 0.12 to 0.39; p < 0.001). Moreover, when the analysis was limited to men older than age 50, SHBG levels were lower in those with moderate-severe disease (WMD: −11.32 nmol/l, 95% CI = −14.23 to −8.40); while for men with body mass index (BMI) >27 kg/m2, moderate-severe NAFLD had higher SHBG levels than those with mild disease (WMD: 1.20 nmol/l, 95% CI = −2.01 to 4.42).
Conclusion:
The present meta-analysis shows that lower TT is associated with the severity of NAFLD in males, while the relationship between SHBG and severity of NAFLD is still to be further verified.
Keywords
Introduction
Non-alcoholic fatty liver disease (NAFLD) is a chronic liver disease mainly characterized by fatty infiltration of the liver. The prevalence of NAFLD is increasing in parallel with the global increase in obesity and type 2 diabetes mellitus (T2DM). 1 NAFLD is estimated to affect at least 25% of the adult population and is considered a public health problem worldwide.2,3 NAFLD starts as hepatic steatosis, which may progress to non-alcoholic steatohepatitis (NASH), even liver cirrhosis and hepatocellular carcinoma. Around 10–25% of patients with NAFLD progress to NASH, and 20% of NASH progress result in liver fibrosis, which is significantly associated with the increase in liver-related mortality. 4 Liver biopsy is considered to be the gold standard for clinical diagnosis and staging of NAFLD today. 5 However, due to the invasiveness of liver biopsy, it is difficult to be widely carried out in clinical practice. 6 Therefore, the discovery of blood biomarkers associated with NAFLD contributes to early identification and assessment of the severity of NAFLD. 7
Studies have shown that male sex, obesity and T2DM were independent risk factors for NAFLD.8,9 The prevalence of NAFLD in young and middle-aged males was higher than in females (28.0% versus 10.8%). 10 A multi-national study with biopsy-confirmed NAFLD and advanced hepatic fibrosis showed that male sex was associated with worse survival and greater incidence of hepatocellular carcinoma. 11 Hence, male sex could be associated with higher prevalence and severity of NAFLD. Acquired hypogonadism in males is commonly accompanied with obesity and metabolic syndrome. 12 Deficiency of total testosterone (TT) or sex hormone–binding globulin (SHBG) is associated with the accumulation of visceral adipose tissue and insulin resistance (IR).13,14 Plasma SHBG and TT levels were reduced in obese SHBG-transgenic mice when compared with lean mice. 15 In addition, obesity is also closely associated with the prognosis of NAFLD patients. 16 In recent years, many studies have reported the relationship between NAFLD and sex hormones (especially levels of TT and SHBG).17,18 A meta-analysis reported that lower TT levels were associated with NAFLD in men, whereas higher SHBG levels were associated with lower NAFLD odds in both men and women. 19 However, the relationship between sex hormones and the severity and prognosis of NAFLD remains uncertain. Therefore, we performed a meta-analysis to explore the relationship between TT, SHBG levels and the severity of NAFLD in males, for early identification of the severity and prediction of the prognosis of patients with NAFLD.
Materials and methods
Research strategy
This meta-analysis was conducted and reported following the MOOSE (Meta-analyses Of Observational Studies in Epidemiology) guideline. All the included studies were filtered through PubMed, Embase, the Cochrane Database, Web of Science, WanFang, China National Knowledge Infrastructure and VIP databases from inception to 31 August 2021. We used the following keywords and terms as follows: (‘Non-alcoholic Fatty Liver Disease’ or ‘Non alcoholic Fatty Liver Disease’ or ‘NAFLD’ or ‘Nonalcoholic Fatty Liver Disease’ or ‘Fatty Liver, Nonalcoholic’ or ‘Liver, Nonalcoholic Fatty’ or ‘Nonalcoholic Fatty Livers’ or ‘Steatohepatitis, Nonalcoholic’) and (‘Testosterone’ or ‘Sex hormone binding globulin’ or ‘SHBG’ or ‘Sex hormone’ or ‘Gonadal hormone’ or ‘Gonadal Steroid Hormone’ or ‘Sex Steroid Hormone’). The retrieved studies and references related to meta-analysis were carefully reviewed to obtain studies that met the criteria. The search strategy is attached in Supplementary Table 1.
Inclusion criteria
The inclusion criteria were as follows: (1) study types: clinical studies evaluating the relationship between the levels of serum TT and/or SHBG and severity of NAFLD; (2) participants and grouping: adult male patients with NAFLD, which were divided into mild and moderate-severe groups based on the degree of fatty infiltration; (3) diagnostic methods: NAFLD was diagnosed with ultrasound, computed tomography, magnetic resonance imaging or pathological biopsy.
Exclusion criteria
The exclusion criteria were as follows: (1) other diseases that could cause NAFLD were excluded, such as viral infections, alcohol intake, and the use of drugs; (2) case reports, abstracts, reviews, comments and letters; (3) duplicate publications; (4) language was not Chinese or English; and (5) data that could not be extracted, transformed or obtained.
Data collection
Data extraction was conducted independently by two authors (Z.H. and Z.Y.). The data extracted from the studies include the research topics, the details of the first author, year of publication, study type, number of NAFLD patients in the mild and moderate-severe groups, diagnostic methods of NAFLD, basic characteristics of participants, mean values and standard deviations (SDs) of TT, SHBG, and odds ratios (ORs) for moderate-severe NAFLD with 95% confidence interval (CI). We contacted the authors of the primary reports to request the related unpublished data. If the authors did not reply, we used the available data for our analyses. If the included studies provided data of median and range or median and interquartile range, the data were transformed to mean and SD using an online computing tool (http://www.math.hkbu.edu.hk/~tongt/papers/median2mean.html).20,21
Quality assessment
The Newcastle Ottawa Scale (NOS) was used to assess the quality of the involved studies. The NOS assessed quality based on three main domains, including selection, comparability and outcome. 22 Studies with a score of 6–9 points were considered to be of high quality.
Statistical analysis
Stata Statistical Software (ver. 12.0; StataCorp LP, College Station, TX, USA) was utilized in the meta-analysis, and p < 0.05 was regarded as statistically significant. Continuous variables were presented as weighted mean differences (WMDs). If I2 was more than 50%, heterogeneity was recognized as significant. If no obvious heterogeneity existed in the research results, a fixed effects model was used for the meta-analysis. When the heterogeneity was high, a random-effects model, subgroup analysis or sensitivity analysis was used. Publication bias was assessed by Egger’s test. 23 If a significant publication bias existed, the trim-and-fill method was used to adjust its potential effect. 24 Subgroup analyses were performed for different mean ages, mean BMIs, NOS stars and regions.
Results
Literature selection
A total of 774 studies were selected from the databases mentioned at the beginning. After eliminating 164 duplicated studies and screening the titles and abstracts for studies that were not relevant because of the topic or research type, 56 studies were included in the full-text review. Finally, there were 10 studies25–34 included in our meta-analysis. The flow chart of the review is shown in Figure 1.

Flow diagram of the study selection.
Characteristics of the included studies
The basic characteristics of the 10 included studies are shown in Table 1. A total of 2995 adult male patients with NAFLD, including 1595 cases in the moderate-severe group and 1400 cases in the mild group, were reviewed. By scanning the full texts of these 10 studies, we found that the study types were all cross-sectional. Among the included studies, seven studies were performed in Asia,26–31,33 two studies were performed in North America,25,34 and one was performed in Europe. 32 Ultrasound and liver biopsy were used for the diagnosis of NAFLD. In addition, the NOS stars of all included studies are attached in Supplementary Table 2.
Main characteristics of included studies and quality assessment score.

BMI, body mass index; NA, non-available; NOS, Newcastle Ottawa scale; SHBG, sex hormone-binding globulin; TT, total testosterone.
The data of ORTT and ORSHBG are included in Figure 3(a) and (b), and not listed in Table 1.
Contrast indicator of TT (ng/ml)
In this section, eight studies involving TT were included in the meta-analysis, including 1435 cases in the moderate-severe group and 1341 cases in the mild group. The results of the heterogeneity test showed that I2 = 49.0%, p = 0.056. A meta-analysis was conducted using a fixed-effects model to evaluate the difference between the moderate-severe and mild groups with respect to TT, which showed that the levels of TT in the moderate-severe group were lower than those in the mild group (WMD: −0.35 ng/ml, 95% CI = −0.50 to −0.20, p < 0.001; Figure 2).
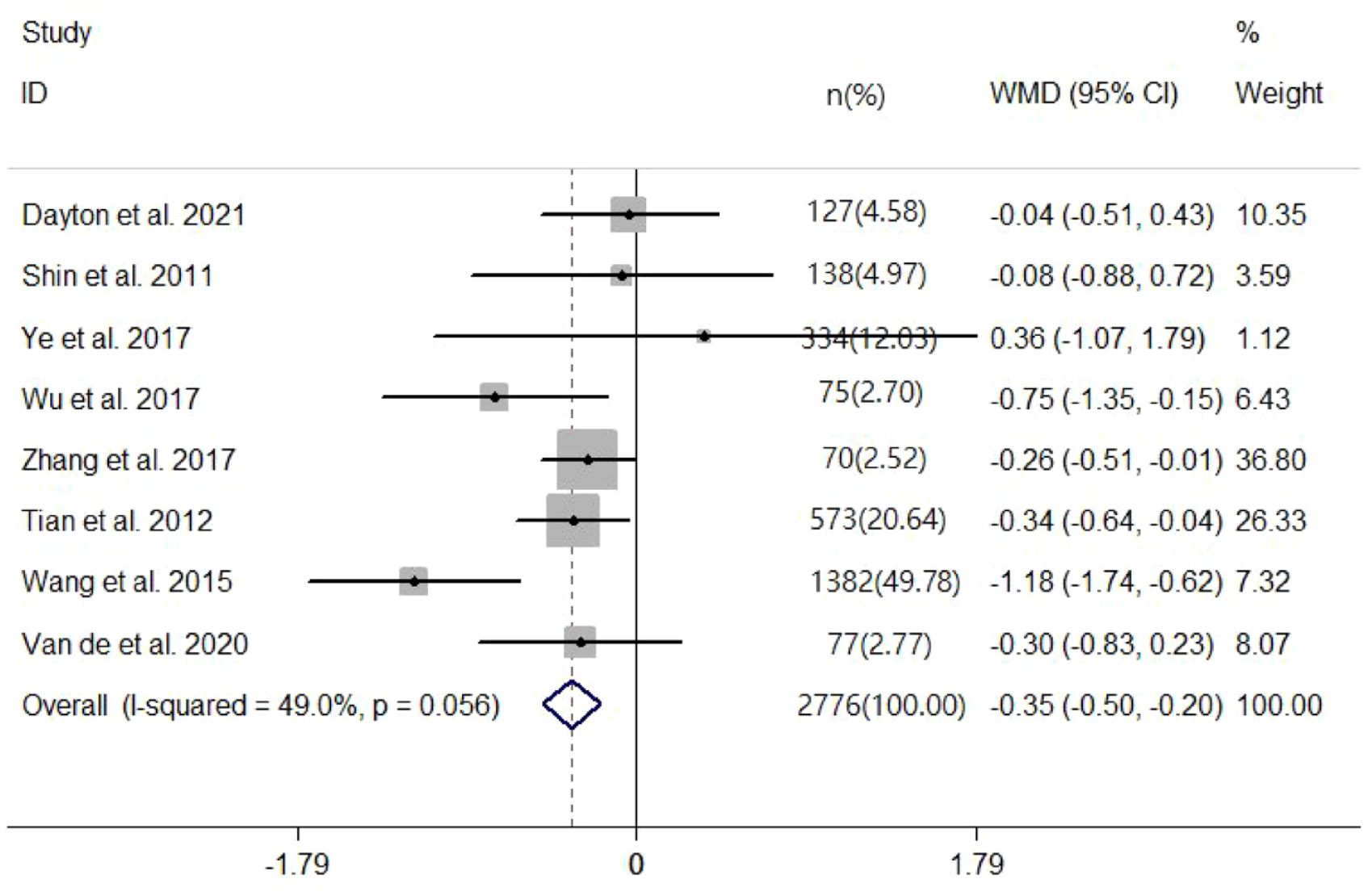
Adjusted forest plot of TT levels (ng/ml) in patients with mild and moderate-severe NAFLD (fixed-effects model). The X-axis represents the value of the effect size [TT levels (ng/ml)]. Each line segment represents the effect size of each study and its 95% CI. The black dot represents point estimates of the effect size for each study. The square represents the weight of each study, and the greater the weight, the greater the area of the square. The diamond represents the combined effect size and CI of multiple studies, and the centre of the diamond represents a point estimate of the combined effect size and is indicated by a dotted line perpendicular to the X-axis. The width of the diamond represents the 95% CI of the combined effect size.
Contrast indicator of SHBG (nmol/l)
There were six studies involving SHBG in the meta-analysis, including 1317 cases in the moderate-severe group and 1247 cases in the mild group of males with NAFLD. Because of the significant heterogeneity (I2 = 97.2%, p < 0.001), we used a random-effects model. There was no significant difference in the moderate-severe and mild groups with respect to SHBG (WMD: −3.70 nmol/l, 95% CI = −9.90 to 2.50, p = 0.242). The sensitivity analysis under a random-effects model showed that no single study dramatically affected the robustness of the pooled result across studies (Supplementary Figure 1). Egger’s test in SHBG suggested that there was little possibility of publication bias (p = 0.191). As shown in Table 2 and Supplementary Figures 2 and 3, we performed subgroup analyses stratified by mean age and body mass index (BMI) of patients. The median of the mean age was 50 years, and 24 and 27 kg/m2 were the quartiles of the mean BMI in these included studies, which were used as cut-off points of subgroup analysis to explore the differences of SHBG levels in different subgroups with different severities of NAFLD. When the mean of age was more than 50 years, the levels of SHBG in the moderate-severe group were lower than those in the mild group (WMD: −11.32 nmol/l, 95% CI = −14.23 to −8.40, p < 0.001; I2 = 44.4%, p = 0.180). When the mean of BMI was more than 27 kg/m2, the levels of SHBG in the moderate-severe group were higher than those in the mild group (WMD: 1.20 nmol/l, 95% CI = −2.01 to 4.42, p = 0.048; I2 = 0%, p = 0.830). Therefore, the difference between the moderate-severe and mild groups in SHBG might be more significant in men older than age 50 or BMI >27 kg/m2.
Subgroup analyses of SHBG in patients with mild and moderate-severe NAFLD.

BMI, body mass index; CI, confidence interval; NAFLD, non-alcoholic fatty liver disease; NOS, Newcastle Ottawa Scale; SHBG, sex hormone–binding globulin; WMD, weighted mean difference.
Relationship between TT, SHBG and the severity of NAFLD
The meta-analysis was conducted using fixed-effects models to evaluate the relationship between TT, SHBG and the severity of NAFLD in males. Analysis of OR estimates for the relationship between TT and the severity of NAFLD comprised 1171 patients in the moderate-severe group and 842 individuals in the mild group from four studies. The results showed lower TT was closely associated with the severity of NAFLD in males [OR = 0.79, 95% CI = 0.73 to 0.86, p < 0.001; I2 = 41.5%, p = 0.145; Figure 3(a)]. Analysis of OR estimates for the relationship between SHBG and the severity of NAFLD comprised 952 patients in the moderate-severe group and 628 individuals in the mild group from three studies. The results of pooled analysis showed that lower SHBG was also associated with the severity of NAFLD in males [OR = 0.22, 95% CI = 0.12 to 0.39, p < 0.001; I2 = 46.4%, p = 0.155; Figure 3(b)].

(a) Forest plot of the relationship between TT and the severity of NAFLD in males; (b) forest plot of the relationship between SHBG and the severity of NAFLD in males (fixed effects model). The X-axis represents the value of the effect size (ORTT or ORSHBG). Each line segment represents the effect size of each study and its 95% CI. The black dot represents point estimates of the effect size for each study. The square represents the weight of each study, and the greater the weight, the greater the area of the square. The diamond represents the combined effect size and CI of multiple studies, and the centre of the diamond represents a point estimate of the combined effect size and is indicated by a dotted line perpendicular to the X-axis. The width of the diamond represents the 95% CI of the combined effect size. The arrow represents a 95% CI of the effect size of the study that is beyond the display range of the graph. The data of ORTT and ORSHBG are included in Figure 3, and not listed in Table 1.
Discussion
According to this meta-analysis enrolling 2995 patients with NAFLD in 10 studies, we can conclude that patients categorized into the moderate-severe group had lower levels of TT than the mild group in male patients with NAFLD, and TT and SHBG might be important risk factors of the moderate-severe NAFLD in males. However, the difference in SHBG between the moderate-severe and mild groups was affected by the variations in age and BMI. This is the first meta-analysis to our knowledge to investigate the relationship between TT, SHBG levels and the severity of male patients with NAFLD.
Testosterone is the main sex hormone in males, which is produced and synthesized by the interstitial cells of the testis. Several studies have shown that compared with patients without NAFLD, male patients with NAFLD had lower levels of TT, and decreased TT was closely related to NAFLD.35–37 After adjusting for those known risk factors such as age, other sex hormones (SHBG, oestradiol), obesity and lifestyle, the concentrations of TT remained inversely associated with NAFLD in males (OR = 0.43, p = 0.044). 18 The results of our meta-analysis also showed that the TT levels of male patients with NAFLD in the moderate-severe group were lower than those in the mild group (WMD: −0.35 ng/ml, 95% CI = −0.50 to −0.20), and levels of TT were negatively correlated with the severity of NAFLD (OR = 0.79, 95% CI = 0.73 to 0.86). Fujihara et al. 38 reported that low free testosterone was associated with the fibrosis-4 index, a non-invasive marker of liver fibrosis, which also supported our results. Testosterone is a key substance in glucolipid metabolism and is associated with IR. 39 IR is one of the important pathogenic mechanisms of NAFLD, which is prone to increase the levels of free fatty acids, promote the production of low-density lipoprotein and triglyceride, and activate oxidative stress response, leading to the occurrence and development of NAFLD.40,41 In addition, the possible mechanism of low TT promoting NAFLD development was related to upregulation of lipid synthesis and inhibition of fatty acid oxidation. The decrease in TT can cause the accumulation of triacylglycerol in abdominal adipose tissue and lead to visceral obesity.42,43 An experimental study in animals showed that the levels of blood lipid and subcutaneous or visceral fat in rats treated with orchiectomy were significantly increased, which would improve after testosterone replacement therapy. 44 Mice with knockout of liver androgen receptor would develop more severe IR and hepatic steatosis than normal obese mice fed with high-fat diet. 45 Several studies showed that testosterone therapy could increase insulin sensitivity and muscle mass, and reduce liver fat in males.46–49 Moreover, a prospective study also showed that long-term testosterone replacement could improve hepatic steatosis and abnormal liver function, IR, dyslipidaemia, obesity and other metabolic diseases in males with hypogonadism, and reduce cardiovascular disease (CVD)-related mortality, 50 indicating that testosterone can improve the prognosis of NAFLD in males through improving metabolic abnormalities. 51 However, other studies showed that testosterone treatment could reduce subcutaneous fat, adiponectin and other cardiovascular risk parameters, but could not change liver fat and visceral fat content.52,53 The results have been inconsistent possibly due to the application of different methods for assessment of regional abdominal adipose tissue, inclusion of various patient cohorts and the use of a variety of testosterone doses and administration forms (oral, patch, gel or injections).46,54 Combining the results of previous studies and our meta-analysis, we conclude that low TT levels are strongly associated with the severity of NAFLD in males.
The results of our meta-analysis showed that there was no significant difference in SHBG levels between the moderate-severe and mild groups (WMD: −3.70 nmol/l, p = 0.242), while low SHBG was a risk factor for high-grade NAFLD in multivariate analysis (OR = 0.22, 95% CI = 0.12 to 0.39). Therefore, the relationship between SHBG and the severity of NAFLD seems to remain uncertain according to the results of current researches. SHBG is produced primarily in the liver and is a binding protein with high binding affinity for testosterone, oestradiol and dihydrotestosterone, 55 and SHBG regulates their biological availability in the circulation. 56 The level of SHBG, which binds testosterone with high affinity and transports testosterone in the circulation, is strongly positively correlated with the level of testosterone in plasma.57,58 Therefore, the relationship between SHBG and NAFLD may be affected by TT levels, which may also be a combined association of SHBG and TT. Studies showed that low SHBG and TT were associated with IR-related diseases (T2DM, metabolic syndrome and NAFLD).59–61 Cytokines, fat accumulation in liver and IR are important determinants of SHBG production, and SHBG expression in human and SHBG-transgenic mice are perhaps mediated through effects on the transcription factor hepatocyte nuclear factor 4-α.62,63 However, the excessive accumulation of liver fat might lead to damage of liver function and further affect the synthesis of SHBG. In addition, a study showed that SHBG could predict cardiovascular events [hazard ratio (HR) = 1.07, 95% CI = 1.00 to 1.14), p = 0.03] and all-cause mortality (HR = 1.13, 95% CI = 1.06 to 1.21, p < 0.01) in males at high risk of CVD. 64 Therefore, we conducted subgroup analyses according to mean or quartile of age and BMI to explore the factors that might influence the difference in SHBG level between the moderate-severe and mild groups. The results showed that when the age was more than 50 years, the SHBG levels of the moderate-severe group were lower than those of the mild group; when the BMI was over 27 kg/m2, the SHBG level of the moderate-severe group was higher than that of the mild group. It can be seen that the relationship between SHBG and NAFLD severity was affected by BMI and age. In a multicentre study, the results showed that the association between SHBG and mortality in males with T2DM was age-dependent, with mortality in patients older than 66 years significantly higher than in those younger than 66 years. 65 It was well established that BMI was also an important embodiment of obesity, which was the central part of metabolic syndrome.66,67 Serum SHBG levels differ in the normal life cycle and are affected by BMI, 68 which might depend on metabolic syndromes such as IR and obesity and affect the occurrence and progression of NAFLD. Therefore, the changes in levels of SHBG might be related to the severity of NAFLD in men older than age 50 or BMI >27 kg/m2.
However, there are several limitations of this meta-analysis. First, this is a pooled analysis of observational cross-sectional studies, which can prove only the correlation, not the causal relationship. Second, most of included studies in this meta-analysis were from Asian countries (7 studies), and studies by Tian et al. and Wang et al. from China account for over 60% of the testosterone data and 73% of the results for SHBG. As a result, the representation of Western countries is limited. Third, most of the patients with NAFLD in the included studies were diagnosed by ultrasonography, and the severity of NAFLD was divided into two groups according to the degree of fatty infiltration on ultrasound. NAFLD diagnosis was variably based on techniques with different accuracy, although the diagnostic accuracy of ultrasonography in NAFLD is indeed higher than that previously reported. In addition, the criteria for definition of NAFLD severity were unlikely to be exactly the same among the various studies. Due to the limitations of the number of studies, only two groups (mild versus moderate-severe) were divided for comparison. The severity of NASH could also affect the results. Fourth, low testosterone values may have different biological explanations according to the different age groups. Finally, only three studies analysed the ORs for relationship between SHBG and the severity of NAFLD. Therefore, the results of this meta-analysis need to be further validated by pooling more relevant studies.
Conclusion
In conclusion, lower TT is associated with the severity of NAFLD in males, while the relationship between SHBG and the severity of NAFLD is limited to men older than age 50 or BMI >27 kg/m2. However, due to the quality and quantity of the included studies, further studies are needed to reveal the relationship between TT, SHBG and the severity of male patients with NAFLD.
Supplemental Material
sj-docx-1-tae-10.1177_20420188221106879 – Supplemental material for Relationship between total testosterone, sex hormone–binding globulin levels and the severity of non-alcoholic fatty liver disease in males: a meta-analysis
Supplemental material, sj-docx-1-tae-10.1177_20420188221106879 for Relationship between total testosterone, sex hormone–binding globulin levels and the severity of non-alcoholic fatty liver disease in males: a meta-analysis by Man-Qiu Mo, Zi-Chun Huang, Zhen-Hua Yang, Yun-Hua Liao, Ning Xia and Ling Pan in Therapeutic Advances in Endocrinology and Metabolism
Footnotes
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Author contribution(s)
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation of China, No. 8176030057.
Conflict of interest statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Availability of data and materials
Not applicable.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.