
Abstract
Background:
Immunoassay (IA) measurements of thyroid hormones have previously given inaccurate results of triiodothyronine (T3), free triiodothyronine (FT3), and free thyroxine (FT4) when concentrations of TBG are low. We evaluate the hypothesis that abnormal concentrations of specific binding proteins (BPs) affect IA measurements and provide results which might misguide the diagnosis and treatment of patients. This study assesses IAs for the measurement of T3, FT3, and cortisol when levels of TBG and CBG are high or low. Comparisons are made between IA and LC-MS/MS.
Methods:
Serum or plasma samples with high (>95th percentile, n = 25) or low (<5th percentile, n = 27) concentrations of BP were collected. The concentrations of T3, FT3, and cortisol were measured by validated IA and liquid chromatography tandem mass spectrometry (LC-MS/MS) methods. Spearman correlation and Wilcoxon matched-pairs signed rank analyses were used to compare the two methods.
Results:
When TBG levels are <5th percentile, the differences between the IA and LC-MS/MS results for T3 and FT3 are statistically significant (T3, p = 0.0011; FT3, p = 0.0003). When CBG levels are >95th percentile, the difference between the IA and LC-MS/MS measurements of cortisol is statistically significant (p = <0.0001).
Conclusion:
Abnormal BP concentrations appear to affect the accuracy of IA measurements of T3, FT3, and cortisol. The population of patients with either high or low levels of BPs is significant. Our samples reflect that 65% of women aged between 15 and 49 years are taking oral contraceptives in the US, and thus have elevated levels of BPs. In this group, IA results for cortisol are falsely low. Our samples reflect that patients with protein losing diseases have low BP concentrations. Among a group with renal complications, IA measurements of T3 are overestimated, while those of FT3 are underestimated. Are the Food and Drug Administration and diagnostic companies adequately assessing the accuracy of IA tests?
Keywords
Introduction
Thyroid and sex hormones are small molecule chemical messengers that present several well-characterized challenges to analysis by immunoassay (IA).1–6 The majority of circulating thyroid and sex steroid hormones are bound to serum proteins, enabling transport and increased stability. Hormone levels in the body are regulated by both specific binding proteins (BPs) [thyroxine binding globulin (TBG), corticosteroid binding globulin (CBG), sex-hormone binding globulin], which bind to their respective hormones with high affinity, and non-specific BPs [albumin (ALB) and pre-albumin], which bind hormones with much lower affinity.
Historically, IA methods for the quantification of low molecular weight hormones, like estradiol, required key purification steps such as solvent extraction and chromatography to meet original validation criteria. 7 With the simplification of IA techniques for small molecule hormone analysis, these additional purification steps have been omitted. An editorial 8 by Cali published in 1973 succinctly addresses the cost of adapting these simplified ‘direct’ IA methods, which deliver precision at the expense of accuracy. Despite consistent reports of problems with the validity of IA methods over the past 33 years, these methods are, remarkably, still routinely performed in the laboratory.9–23
Investigations by our laboratory over the past two decades have revealed that IA measurements of free thyroxine (FT4), free triiodothyronine (FT3), and triiodothyronine (T3) are often overestimated when concentrations of these analytes are low and in scenarios with low TBG.4,5,16–21,24 Inaccurate results for ‘free’ (FT4 and FT3) and bioactive (FT3 and T3) thyroid hormones present a major problem when it comes to diagnosing and treating hypothyroidism. In fact, we demonstrated that two-thirds of patients classified as subclinical hypothyroidism by IA were reclassified as clinically hypothyroid when FT4 and FT3 were measured by liquid chromatography tandem mass spectrometry (LC-MS/MS) following ultrafiltration to remove BPs. 17
More recently, we reported observing falsely low cortisol measurements using both Siemens and Abbott IAs in a series of women who were taking oral contraceptives (OCPs), and thus had elevated levels of CBG. 25 A number of common conditions, including pregnancy,26–28 adrenal insufficiency 29 and renal failure, 30 as well as the use of widely prescribed medications such as synthetic thyroid hormones,27,31,32 OCPs,33–35 and glucocorticoid therapies, 28 can lead to variations in BP concentrations that affect the accuracy of hormonal IA measurements for a significant population of patients.
In this study, we evaluate the hypothesis that abnormal concentrations of high affinity BPs (TBG and CBG) will effect routine IA testing of thyroid (T3, FT3) and steroid (cortisol) hormones, referencing these measurements to those obtained by validated LC-MS/MS methods.
Methods
Subjects and specimens
The abnormal BP study was a prospective study of samples received at the NIH Clinical Center, Department of Laboratory Medicine from February 2020 to November 2020. Samples were selected for inclusion in the study if they were identified as having concentrations of specific binding globulins (TBG or CBG) above the 95th percentile, or below the 5th percentile. To identify samples with low concentrations of binding globulins, we commonly screened for samples with serum albumin concentrations less than the 2.5th percentile. In total, we have included 52 independent samples for analysis, 21 samples containing high concentrations of TBG, 18 with high concentrations of CBG, 27 containing low concentrations of TBG, and 24 with low concentrations of CBG. This study was approved by the Institutional Review Board (IRB) at the National Institutes of Health (protocol 93-CC-0094). Written informed consent for inclusion in the study is waived by our IRB. Through this protocol, we are allowed to re-purpose discarded samples submitted to the Department of Laboratory Medicine for research.
A retrospective assessment of sample origin revealed that 12 of the 18 samples with high TBG and CBG concentrations were from women between the ages of 15 and 49 years taking OCPs. The samples containing low TBG and CBG levels were from patients who were confirmed to be undergoing treatment for renal complications.
Serum and plasma samples included in the investigation were collected between 05:00 h and 10:00 h. All blood sampling was performed by certified phlebotomists, and collected in heparin/gel-containing plasma- or preservative/gel-free serum-specimen collection tubes. All samples were kept chilled and centrifuged within 1 h of collection to separate plasma or serum. Samples were stored at −20°C short-term (24 h) or −80°C long-term (>24 h) storage until assayed by IA and LC-MS/MS.
Sample size determination
This comparison of methods evaluation questions the accuracy of IA measurements at concentrations of specific BPs that are reflective of the upper or lower 5% of the reference interval. Our sample populations are not normally distributed. p-values are dependent on sample size, such that larger sample sizes tend to result in smaller p-values. Thus, our sample sizes for this initial investigation were guided by the ability to see a statistically significant difference in the means, even with relatively small sample sizes (15 ⩽n <30).
Colorimetric assay
ALB was measured using the Roche Cobas 6000 (Indianapolis, MN, USA). See Supplemental material online for data and reference interval used.
Immunoassay
Thyroid hormones (T3, FT3) were measured using the Roche Cobas 6000 (Indianapolis, MN, USA). TBGs were measured using the Siemens Immulite 2000 XPi analyzer (Tarrytown, NY, USA). CBG was measured by radioimmunoassay by Esoterix Endocrinology (Calabasas Hills, CA, USA). Cortisol was measured using the Abbott Architect ci8200 (Chicago, IL, USA). See Supplemental material for data and reference intervals used for TBG and CBG.
LC-MS/MS
T3 was measured by isotope dilution LC-MS/MS using the Agilent 6460 triple quadrupole MS coupled with an ESI source and Agilent 1200 Infinity series HPLC (Agilent Technologies, Santa Clara, CA, USA) as previously described.16,19 FT3 and FT4 were separated from protein-bound hormones by ultrafiltration at 37°C, followed by measurement by isotope dilution LC-MS/MS using an AB Sciex Triple Quad 6500 (AB Sciex, Concord, ON, Canada) and Shimadzu LC-20AD HPLC (Shimadzu Instruments, Columbia, MD, USA) as previously described. 36 Complete method validation studies and diurnal reference intervals for thyroid hormones have been established. 37
Cortisol was measured by isotope dilution LC-MS/MS using the Agilent 6490 triple quadrupole MS coupled with an atmospheric pressure photoionization source and Agilent 1200 Infinity series HPLC (Agilent Technologies, Santa Clara, CA, USA) as previously described.38,39 Complete method validation studies and diurnal variations have been established. 40
Analysis
Correlation between analytes measured by IA and LC-MS/MS was determined using the Spearman correlation coefficient (r). p-values less than 0.05 were considered statistically significant. Wilcoxon matched-pairs signed rank tests were used to determine whether the difference in mean measurements by IA versus LC-MS/MS was statistically significant for a given analyte. p-values less than 0.05 for the comparison of the difference in mean measurements obtained by IA versus LC-MS/MS were considered statistically significant. Statistical analyses were performed using GraphPad Prism version 8 for Macintosh (GraphPad Software, San Diego, CA, USA; www.graphpad.com). Descriptive statistics were calculated for each analyte separately and grouped according to BP concentration, either high (>95th percentile) or low (<5th percentile) (see Supplementary material for additional statistical calculations related to each analyte).
Results and discussion
Previous method comparisons and case studies from our laboratory5,16,21,41,42 and others43,44 provide preliminary evidence that IA measurements for thyroid hormones are influenced by TBG concentrations. Specifically, our laboratory has established that direct measurements of FT4 by LC-MS/MS, which physically separate BPs by ultrafiltration, show the expected inverse log-linear relationship with TSH and no correlation to TBG or ALB concentrations. By contrast, FT4 measurements by automated IA, a sequential two-step electrochemiluminescent assay—which does not require the physical removal of TBG or ALB, or the measurement of thyroxine-binding capacity—do not result in an inverse log-linear relationship with TSH, and strongly correlate to TBG or ALB concentrations. 16 Our results also complement a prior investigation 42 examining the accuracy of FT4 measurements by IA. In the aforementioned study, the concentration of FT4 was kept constant, while levels of TBG-bound T4 were increased to reflect the pathophysiological range found in patient sera. The study concluded that FT4 measurements by IA were not accurate at certain levels of TBG-bound T4. While BP interference is frequently alluded to in many critiques of IA techniques2,15,45,46 and becoming more widely discussed, 47 there are few investigations which evaluate the role of BP concentration on routine IA measurements of hormones, aside from FT4.
In this study, we explicitly assessed the influence of naturally occurring variations of TBG on IA measurements of the biologically active thyroid hormones (T3 and FT3) that are the most clinically relevant for evaluating thyroid disorders.5,48 It is important to mention that we cannot make predictions as to how high or low levels of BPs will interfere with IA measurements. Specific BP binding constants can differ by more than one order of magnitude when compared with IA antibodies. 49 Since the proprietary antibody binding constants are not made available, we cannot form hypotheses as to whether certain analyte values will be under- or overestimated as a result of variable binding interactions taking place in the presence of high or low BP concentrations.
When we compared our current analysis with prior investigations of IA performance from our laboratory,4,16–21,23 we found complementary trends. In inclusive analyses, T3 values by IA and LC-MS/MS assays correlated relatively well ( Table 1 ); however, the correlation was significantly diminished when only the low BP measurements were considered ( Table 2 ).20,21,23 Correlations of FT3 were poor under all BP scenarios. These trends highlight the importance of performing critical evaluations of IA accuracy that take into consideration pathologically relevant conditions.
Within-analyte and between-assay correlation among analytes with all samples (both high and low concentrations of binding proteins).
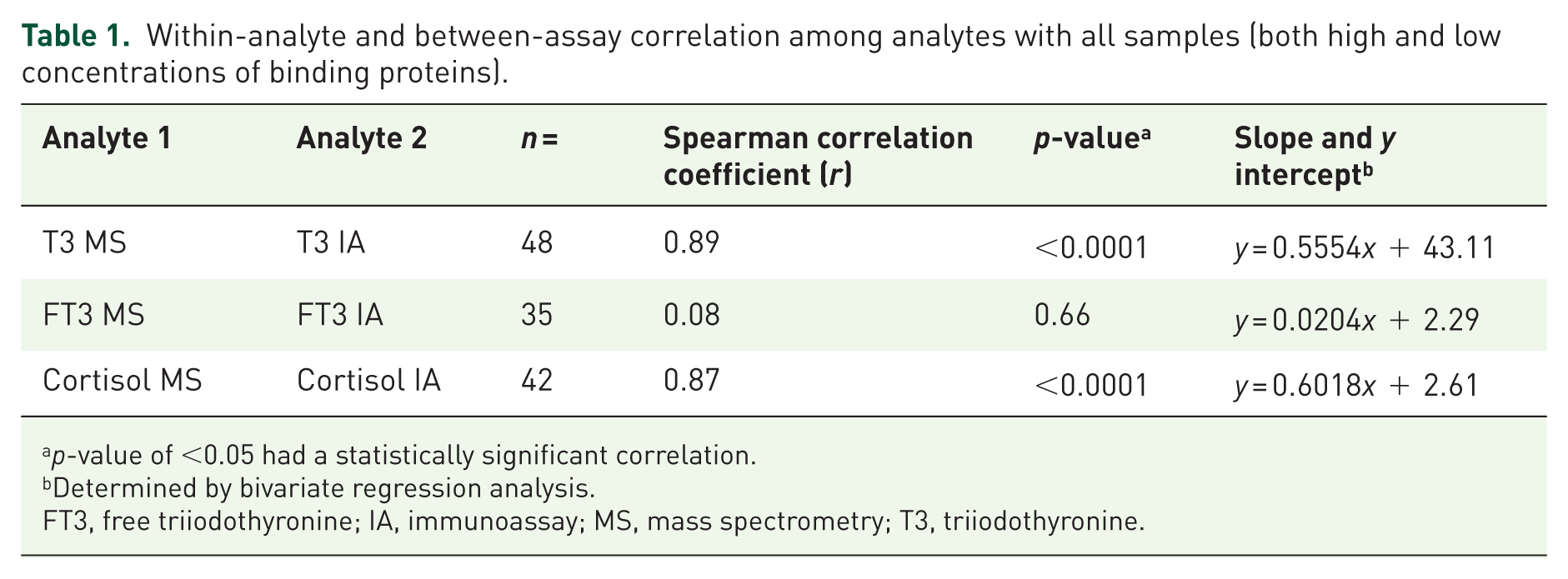
p-value of <0.05 had a statistically significant correlation.
Determined by bivariate regression analysis.
FT3, free triiodothyronine; IA, immunoassay; MS, mass spectrometry; T3, triiodothyronine.
Within-analyte and between-assay correlations separating high and low binding protein sample groups.

p-value of <0.05 had a statistically significant correlation.
Determined by bivariate regression analysis.
FT3, free triiodothyronine; IA, immunoassay; MS, mass spectrometry; T3, triiodothyronine.
When measurements of T3 were analyzed considering low and high TBG subsets separately, the correlation was significantly affected ( Table 2 ). In samples with TBG levels <5th percentile (as should be expected in at least 15% of US adults who have chronic kidney disease), 50 IA measurements of T3 are significantly overestimated ( Table 3 ). The difference between measurements of T3 by IA versus LC-MS/MS was statistically significant. The overall poor correlations between IA and LC-MS/MS measurements for FT3 in the presence of high and low concentrations of TBG were not surprising since a number of studies have established the dependence of FT4 measurements on BP conditions.16,44,51–53 By comparison, the correlation among FT3 measurements seems to be more greatly impacted by high TBG concentrations. IA measurements of FT3 are underestimated as compared with measurements by LC-MS/MS when levels of TBG are high or low. However, the difference between the IA and LC-MS/MS measurements for FT3 was only statistically significant when TBG concentrations were low ( Table 3 ).
Wilcoxon matched-pairs signed rank evaluation of each analyte with poor Spearman correlation (r <0.6) between immunoassay and liquid chromatography tandem mass spectrometry measurements in the presence of high or low BP.

Mean concentration of respective specific BP (TBG reference interval: 11–27 µg/mL; CBG reference interval: 1.7–3.1 mg/dL).
BP, binding protein; FT3, free triiodothyronine; IA, immunoassay; MS, mass spectrometry; T3, triiodothyronine.
In summary, IA should no longer be trusted to provide accurate measurements of active thyroid hormones T3 and FT3 in populations suspected of having low TBG concentrations. The limitations presented by IA demonstrate that LC-MS/MS techniques allow optimization of diagnosis and treatment for patients with thyroid disorders.
This study provides more evidence that the accuracy of cortisol measurements by IA can be affected by the presence of high concentrations of CBG. While previous studies54–58 have investigated the reliability of cortisol measurements by IA, very few24,59 have described the accuracy of IA cortisol measurements taking into consideration both BP fluctuation and comparison with a reference LC-MS/MS method. Similar to the trend observed for T3, when cortisol measurements are analyzed and include both high and low CBG subsets, the correlation between IA and LC-MS/MS is good ( Table 1 ). However, when cortisol measurements in the presence of just high concentrations of CBG are considered, the correlation between the two methods is dramatically decreased ( Table 2 ), and the difference between measurements by IA versus LC-MS/MS was statistically significant ( Table 3 ). In our study, IA underestimates cortisol measurements in the presence of significantly elevated levels of CBG ( Table 3 ).
Falsely low cortisol measurements by IA are an unusual finding. It is well known that lack of specificity of IAs typically leads to an overestimation of analyte concentrations. 2 In our prior report, 24 we hypothesized that the unusually low IA cortisol results were likely the result of high CBG levels (caused by OCPs) 34 based on three patient profiles. After evaluating an additional 11 samples in this study, with the majority collected from women between the ages of 15 and 49 years taking OCPs, we can conclude that there is a strong correlation between falsely low cortisol results by IA and elevated CBG concentrations.
Accurate measurements of thyroid and steroid hormones are necessary to optimize both diagnosis and treatment of various endocrine disorders. Standard immunoassay-based approaches for detecting these essential small molecule hormones do not control for common fluctuations in the concentrations of associated binding globulins, which can occur during pregnancy, renal failure, and as a result of regularly prescribed medications (synthetic thyroid hormones, OCPs, corticosteroids).
This study verifies the concerns expressed by Cali 8 back in 1973. We report that high levels of BPs strongly correlate to inaccurate IA measurements of cortisol. The population of patients presenting with high binding globulins is significant, and arguably biased toward women. More than 65% of women between the ages of 15 and 49 years are taking OCPs, 60 and likely have abnormally high levels of CBG and TBG, including the subset represented by this study. We also demonstrate that both men and women with protein losing diseases, a common symptom of renal complications and diabetes, can be affected by inaccurate IA results for T3 and FT3. Clinicians can optimize the diagnosis and treatment of endocrine disorders by relying on LC-MS/MS to accurately measure small molecule hormones.
While LC-MS/MS is frequently characterized as impractical to implement due to cost, a recent assessment reveals how LC-MS/MS can actually be more cost effective than immunoassay over a 5-year timeline (after the initial purchasing and installation). 61 Unfortunately, many institutions will not implement LC-MS/MS services for thyroid and steroid hormone assays without a concerted effort by the endocrinology community calling for accurate test results that support the effective diagnosis and treatment of patients.
Finally, what role should the FDA and diagnostic companies play in ensuring that the products that they license for diagnostic tests conform to acceptable standards of accuracy?
Supplemental Material
sj-pdf-1-tae-10.1177_2042018821989240 – Supplemental material for The effect of specific binding proteins on immunoassay measurements of total and free thyroid hormones and cortisol
Supplemental material, sj-pdf-1-tae-10.1177_2042018821989240 for The effect of specific binding proteins on immunoassay measurements of total and free thyroid hormones and cortisol by Anastasia Gant Kanegusuku, Katherine A. Araque, Hung Nguyen, Bin Wei, Saman Hosseini and Steven J. Soldin in Therapeutic Advances in Endocrinology and Metabolism
Supplemental Material
sj-pdf-2-tae-10.1177_2042018821989240 – Supplemental material for The effect of specific binding proteins on immunoassay measurements of total and free thyroid hormones and cortisol
Supplemental material, sj-pdf-2-tae-10.1177_2042018821989240 for The effect of specific binding proteins on immunoassay measurements of total and free thyroid hormones and cortisol by Anastasia Gant Kanegusuku, Katherine A. Araque, Hung Nguyen, Bin Wei, Saman Hosseini and Steven J. Soldin in Therapeutic Advances in Endocrinology and Metabolism
Footnotes
Author contributions
Anastasia Gant Kanegusuku: Conceptualization; investigation; data curation; formal analysis; writing-original draft preparation; writing-review and editing.
Katherine Araque: Conceptualization; writing-review and editing.
Hung Nguyen: Investigation; writing-review and editing.
Bin Wei: Investigation; writing-review and editing.
Saman Hosseini: Investigation; writing-review and editing.
Steven J. Soldin: Conceptualization; data curation; project administration; resources; writing-original draft preparation; writing-review and editing.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Steven J. Soldin is funded by an NIH Intramural Research Award.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.