
Abstract
Objective
The aim of our study was to explore the association between serum cystatin C (CysC) and euthyroid Hashimoto’s thyroiditis.
Methods
There were 119 female euthyroid Hashimoto’s thyroiditis patients and 225 healthy controls who were recruited. Serum CysC, thyroid function, thyroid autoantibodies, fasting glucose, liver enzymes, and lipid profile were determined. Clinical parameters were compared between two groups.
Results
Serum CysC levels were significantly higher in euthyroid Hashimoto’s thyroiditis patients compared with controls. In the lowest, middle, and highest tertile groups of CysC, the percentage of Hashimoto’s thyroiditis was 15.9%, 34.2%, and 53.5%, respectively. The percentage of Hashimoto’s thyroiditis was significantly higher in the highest tertile than in the lowest and middle tertiles. Spearman’s correlation analysis showed that serum CysC levels were negatively correlated with free triiodothyronine (FT3), and positively correlated with serum thyroid peroxidase antibody (TPOAb) and thyroglobulin antibody (TGAb). Logistic regression analysis showed that serum CysC was independently related to the status of euthyroid Hashimoto’s thyroiditis.
Conclusions
The present study shows the first evidence suggesting that serum CysC levels are positively correlated with TPOAb and TGAb. Serum CysC might underlie the pathophysiologic features of euthyroid Hashimoto’s thyroiditis.
Keywords
Introduction
Hashimoto’s thyroiditis is the most common autoimmune thyroid disease. It is related to genetic, environmental, immune, and inflammatory factors, but its pathogenesis has not been fully elucidated. 1 The main features of Hashimoto’s thyroiditis include increased serum thyroid peroxidase antibody (TPOAb) and thyroglobulin antibody (TGAb), and infiltration of lymphocytes and plasma cells into the thyroid.2–5 In urban areas of China, the prevalence of TPOAb positive and TGAb positive were 11.5% and 12.6%, respectively. 6 Hashimoto’s thyroiditis can also cause primary hypothyroidism, thyroid cancer, atherosclerosis, diabetes, and adverse pregnancy outcomes.7–11
Cystatin C (CysC) is a soluble basic protein that belongs to the cysteine protease inhibitor family, which is a 13.3-kDa protein (120 residues).12,13 The kidney is the only organ that can clear CysC in the blood. CysC is produced at a constant rate by most nucleated cells, filtered through the renal glomerular membrane, and almost completely reabsorbed by kidney tubular cells.14,15 CysC is expressed in all human tissues and detected in all body fluids. 16 CysC is a clinically recognized indicator of early renal function impairment.17,18 Moreover, CysC is a potent inhibitor of cathepsins, which are proteolytic enzymes that are primarily localized in the endosomal/lysosomal system. 13 Cathepsins degrade intracellular and endocytosed proteins, and play a role in remodeling and degrading the extracellular matrix. 19 CysC protects against widespread tissue damage due to proteolysis that is caused by leaked cathepsins. CysC has been linked to neurological and cardiovascular disorders.13,20,21
Previous studies have shown that serum CysC was related to thyroid function. Wiesli et al. 22 found that serum CysC increased when thyroid stimulating hormone (TSH) was normalized in patients with subclinical hyperthyroidism. Mild thyroid dysfunction significantly alters CysC levels. Therefore, thyroid function has to be considered when CysC is used as a marker of kidney function. Ye et al. 23 found that serum the CysC level was significantly elevated, and the estimated glomerular filtration rate (eGFR) was significantly reduced in both subclinical hypothyroidism and subclinical hyperthyroidism. Thyroid hormone replacement therapy attenuated the rate of decline in renal function in chronic kidney disease patients with subclinical hypothyroidism, which suggesting that thyroid hormone replacement therapy may delay the progression to end-stage renal disease in these patients. 24 Other studies have found that thyroid function had no significant impact on the diagnostic and predictive accuracy of CysC in detecting acute kidney injury in patients.25,26 Therefore, these studies on the correlations between CysC and thyroid function remain controversial. Moreover, there are few studies on the relationship among serum CysC, thyroid autoantibodies, and Hashimoto’s thyroiditis.
To rule out the influence of thyroid function on CysC, we selected euthyroid Hashimoto’s thyroiditis patients as the study population in this research. The aim of the study was to observe the correlations between serum CysC and euthyroid Hashimoto’s thyroiditis in adult female Chinese patients. This could provide a theoretical basis for the clinical diagnosis and treatment of Hashimoto’s thyroiditis.
Materials and methods
Study design and population
This study was conducted from January 2018 to December 2019. There were 119 female euthyroid Hashimoto’s thyroiditis patients who were recruited from outpatients and inpatients in the Department of Endocrinology at the Shanghai Fifth People’s Hospital, Fudan University. Hashimoto’s thyroiditis was diagnosed on the basis of the presence diffuse goiter in the thyroid, which was observed using B-ultrasound, and a high titer of TPOAb (>34 IU/mL) and/or TGAb (>115 IU/mL). There were 225 healthy female controls who were recruited from the physical checkup center at the hospital. Control subjects were normalized for parameters such as gender, age, normal thyroid function, and normal thyroid autoantibodies. They were in self-proclaimed good health, and had no family or personal history of thyroid disease. The exclusion criteria included a history of other autoimmune diseases, severe renal insufficiency, severe hepatic insufficiency, pregnancy during the study period, or any medication history that involved administration of immunosuppressive agents.
The study protocols were approved by the medical ethics committee of the Shanghai Fifth People’s Hospital, Fudan University (No. 2018-114). Consent was obtained from each patient or subject after full explanation of the purpose and nature of all procedures that were used.
Data collection
The patients’ age, medical history, medication history, body mass index (BMI), systolic blood pressure (SBP), and diastolic blood pressure (DBP) were recorded. After a 12-hour overnight fast, the patient’s blood samples were collected for the measurements of serum CysC, liver enzymes, fasting plasma glucose (FPG), renal function, and lipid profile, thyroid function (including free triiodothyronine [FT3], free thyroxin [FT4], and TSH), and thyroid autoantibodies (including TPOAb and TGAb).
Laboratory data
Serum alanine aminotransferase (ALT), urea nitrogen (UN), creatinine (Crea), uric acid (UA), CysC, FPG, total cholesterol (TC), and triglyceride (TG) were analyzed using an automatic analyzer (Cobas 702, Roche Corporation, Mannheim, Germany). Thyroid function and thyroid autoantibody levels were tested using an electrochemical method (Cobas 800, Roche Corporation). eGFR was calculated using the modification of diet in renal disease (MDRD) equation that was developed for the Chinese population: eGFR (mL/minute/1.73 m2) = 186× (Crea×0.011)−1.154 × (age)−0.203× (0.742 if female/1 if male)×1.233, where Crea was in µmol/L and 1.233 was the adjusting coefficient for Chinese patients. 27
Statistical analysis
All data analyses were performed using the Statistical Package for Social Sciences (SPSS) version 22.0 (IBM Corp., Armonk, NY, USA). Normally distributed continuous variables were expressed as the mean ± standard deviation (SD) and analyzed using the Student’s t-test. Non-normally distributed variables were expressed as the median and interquartile range (IQR) and analyzed using a nonparametric test (Wilcoxon test). The categorical variables were presented as frequencies and proportions and analyzed using the χ2 test. Furthermore, Spearman’s correlation analysis was performed to evaluate the association of Hashimoto’s thyroiditis parameters. The binary logistic regression analysis was performed to evaluate the association of serum CysC and euthyroid Hashimoto’s thyroiditis after adjusting for other clinical and biochemical variables. P values of less than 0.05 were regarded as statistically significant.
Results
Demographics of the study population
The clinical characteristics of the study populations are shown in Table 1. Compared with the control (CON) group, serum CysC (P < 0.001), Crea (P = 0.026), TPOAb (P < 0.001), and TGAb (P < 0.001) in the euthyroid Hashimoto’s thyroiditis group were significantly increased, while eGFR was significantly decreased (P = 0.047). There were no significant differences in age, BMI, SBP, DBP, UN, UA, ALT, FPG, TC, TG, FT3, FT4, and TSH between the two groups.
Demographics of the study population.
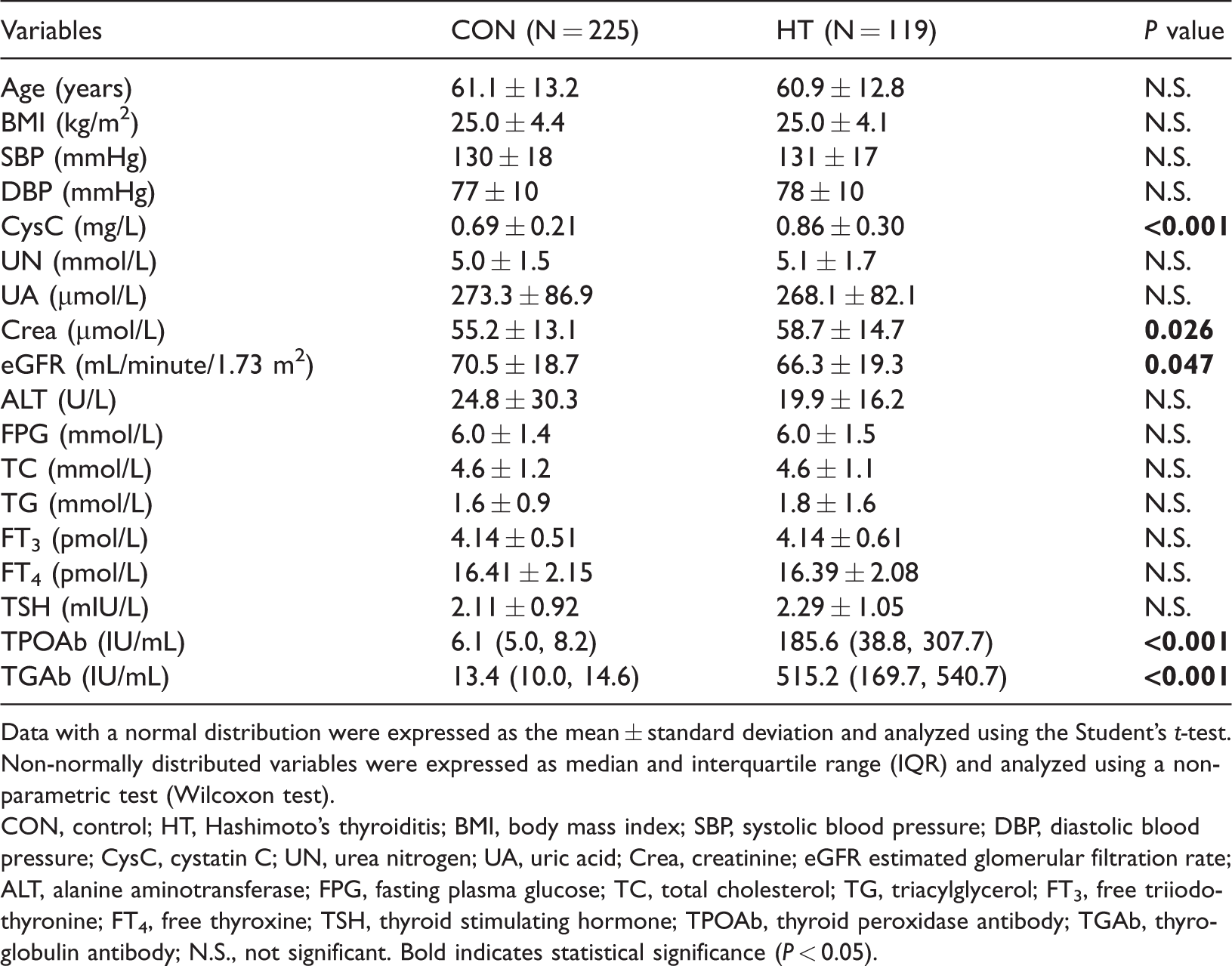
Data with a normal distribution were expressed as the mean ± standard deviation and analyzed using the Student’s t-test. Non-normally distributed variables were expressed as median and interquartile range (IQR) and analyzed using a nonparametric test (Wilcoxon test).
CON, control; HT, Hashimoto’s thyroiditis; BMI, body mass index; SBP, systolic blood pressure; DBP, diastolic blood pressure; CysC, cystatin C; UN, urea nitrogen; UA, uric acid; Crea, creatinine; eGFR estimated glomerular filtration rate; ALT, alanine aminotransferase; FPG, fasting plasma glucose; TC, total cholesterol; TG, triacylglycerol; FT3, free triiodothyronine; FT4, free thyroxine; TSH, thyroid stimulating hormone; TPOAb, thyroid peroxidase antibody; TGAb, thyroglobulin antibody; N.S., not significant. Bold indicates statistical significance (P < 0.05).
Serum CysC levels were significantly higher in patients with euthyroid Hashimoto’s thyroiditis (Table 1, P < 0.001). Patients were divided into tertile group based on serum CysC (the lowest tertile < 0.62 mg/L, the middle tertile 0.62 to 0.82 mg/L, the highest tertile ≥0.82 mg/L). In the lowest, middle, and highest tertile groups for CysC, the percentages of Hashimoto’s thyroiditis were 15.9%, 34.2%, and 53.5%, respectively (Figure 1). The percentage of Hashimoto’s thyroiditis was significantly higher in the highest tertile than in the lowest and middle tertiles (Figure 1, P < 0.001, P = 0.004, respectively). The percentage of Hashimoto’s thyroiditis was significantly higher in the middle tertile than in the lowest tertile (Figure 1, P = 0.001).
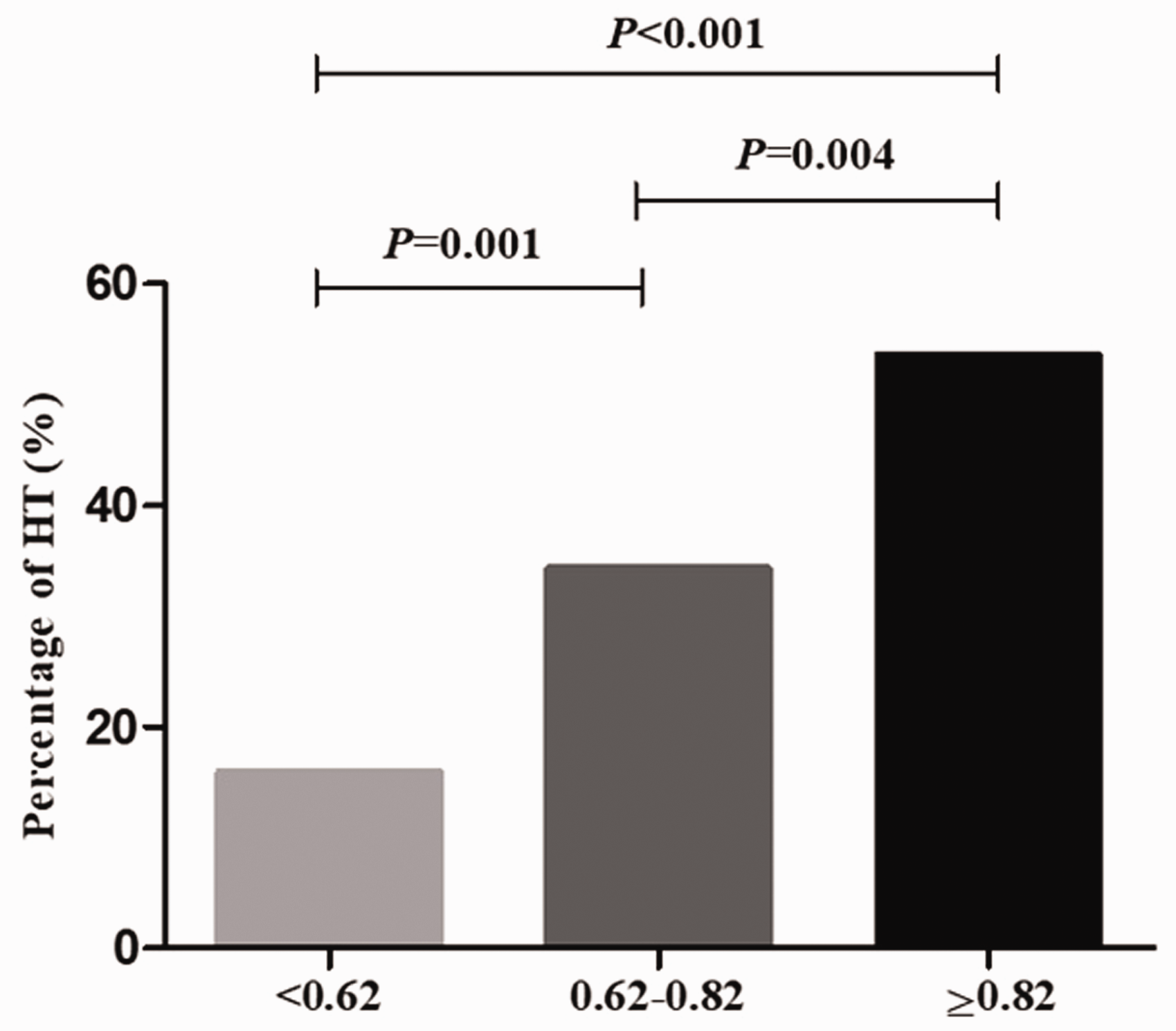
Percentage of Hashimoto’s thyroiditis in different CysC tertile groups.
Association between serum CysC and Hashimoto’s thyroiditis
Spearman’s correlation analysis showed that serum CysC levels were negatively correlated with FT3 (Table 2, P = 0.035), while serum CysC levels were positively correlated with TPOAb (P < 0.001) and TGAb (P < 0.001; Table 2).
Association of serum CysC with parameters of thyroid function and thyroid autoantibodies.

Spearman’s correlation analysis was used to evaluate the association of serum CysC with parameters of thyroid function and thyroid autoantibodies.
CysC, cystatin C; FT3, free triiodothyronine; FT4, free thyroxine; TSH, thyroid stimulating hormone; TPOAb, thyroid peroxidase antibody; TGAb, thyroglobulin antibody; N.S., not significant. Bold indicates statistical significance (P < 0.05).
Binary logistic regression analysis
The relationship between serum CysC and euthyroid Hashimoto’s thyroiditis was evaluated using binary logistic regression analysis (Enter method). The following five models were fitted: Model 1 only included serum CysC (P < 0.001); Model 2 added age and BMI to the predictors of Model 1 (P < 0.001); Model 3 added UN, UA, and Crea to the predictors of Model 2 (P < 0.001); Model 4 added ALT to the predictors of Model 3 (P < 0.001); and Model 5 added FPG, TC and TG to the predictors of Model 4 (P < 0.001). After adjusting for these potentially related factors, serum CysC was independently related to the status of euthyroid Hashimoto’s thyroiditis (Table 3, P < 0.001).
Serum CysC associated with the presence of euthyroid Hashimoto’s thyroiditis in logistic regression.

Data are presented as regression coefficient (standard error), odds ratio (95% confidence interval), and P value
Binary logistic regression analysis was used to evaluate the association of euthyroid Hashimoto’s thyroiditis and CysC after adjusting other clinical and biochemical variables.
M1 is a regression model including serum CysC only; M2 adds age and BMI to the predictors of M1; M3 adds UN, UA, and Crea to the predictors of M2; M4 adds ALT to the predictors of M3; M5 adds FPG, TC, and TG to the predictors of M4
CysC, cystatin C; BMI, body mass index; OR, odds ratio; 95%CI, 95% confidence interval; UN, urea nitrogen; UA, uric acid; Crea, creatinine; ALT, alanine aminotransferase; FPG, fasting plasma glucose; TC, total cholesterol; TG, triacylglycerol. Bold indicates statistical significance (P < 0.05).
Discussion
Currently, the relationship between CysC and Hashimoto’s thyroiditis remains unclear. In this study, we innovatively analyzed the relationship between serum CysC and euthyroid Hashimoto’s thyroiditis in adult female Chinese patients. We found that serum CysC levels were higher in euthyroid Hashimoto’s thyroiditis. Additionally, serum CysC levels were correlated with thyroid autoantibodies. Serum CysC is an indicator of early renal damage in euthyroid Hashimoto’s thyroiditis.
Most studies confirmed that serum CysC levels were related to abnormal thyroid function. Serum CysC levels were significantly elevated, and eGFR was significantly reduced in both subclinical hypothyroidism and subclinical hyperthyroidism. 23 Thyroid hormone replacement therapy attenuated the rate of decline in renal function in chronic kidney disease patients with subclinical hypothyroidism. 24 Serum CysC levels were significantly increased in hyperthyroid patients compared with the control group.28–30 In our study, we also found that serum CysC levels were significantly increased and negatively correlated with FT3, and eGFR was significantly reduced in euthyroid Hashimoto’s thyroiditis patients compared with controls.
Bocchetta et al. 31 first reported a link between renal function and the presence of thyroid antibodies including TPOAb and TGAb. They studied 394 patients who were treated with lithium. The potential role of comorbidities, including diabetes, concurrent antihypertensive medication, treatment with L-thyroxine, and presence of thyroid autoantibodies were analyzed. They found that circulating thyroid antibodies were associated with a decline in eGFR that was lower than 45 mL/minute/1.73 m2. Ellervik et al. 32 found that TPOAb were robustly associated with decreased eGFR from Crea (eGFRCrea) and decreased eGFR from CysC (eGFRCysC). In this study, we found a positive correlation between serum CysC levels and thyroid autoantibodies in euthyroid Hashimoto’s thyroiditis patients. Further statistical analysis found that the percentages of Hashimoto’s thyroiditis were significantly higher in the highest tertile of serum CysC levels than in the middle and lowest tertiles. After adjusting for potentially related factors, serum CysC levels were independently related to the status of euthyroid Hashimoto’s thyroiditis. All of these results demonstrated that serum CysC levels are independently related to the status of euthyroid Hashimoto’s thyroiditis.
With an aging population, an increasing number of elderly people are being diagnosed with Hashimoto’s thyroiditis, but few studies have focused on this population. In this study, we enrolled elderly Hashimoto’s thyroid patients with an average age of 60 years, so the results were different from other studies in young women or premenopausal women.
This study has some limitations. First, the cross-sectional method allows limited exploration of the causal relationship between CysC and Hashimoto’s thyroiditis. In the future, longitudinal studies may provide better information about these relationships. Second, we only studied adult female patients. By increasing the sample size, the relationship among serum CysC, thyroid antibodies, and Hashimoto’s thyroiditis in male patients can be further explored.
In conclusion, the present study is the first evidence that suggests that serum CysC levels are positively correlated with TPOAb and TGAb. Serum CysC levels are independently related to euthyroid Hashimoto’s thyroiditis. Thus, CysC might underlie the pathophysiologic features of euthyroid Hashimoto’s thyroiditis.
Footnotes
Author contributions
Heyuan Ding designed the research; Min Yang and Jinying Zhao performed the experiments; Wencai Ke analyzed the data; Qiaojing Qin wrote the manuscript; Heyuan Ding revised the manuscript; and all authors read and approved the final manuscript.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This work was supported in part by Health Profession Clinical Foundation of Shanghai Municipal Health Commission (No. 201840119), Minhang District Natural Science Foundation of Shanghai (No. 2017MHZ06), Science Foundation of Shanghai Fifth People's Hospital (No. 2018WYZT03), and Medical Key Faculty Foundation of Shanghai (No. ZK2019B15).