
Abstract
Background:
Despite current interest, enthusiasm and progress in the development of therapies for gastroenteropancreatic (GEP) neuroendocrine tumors (NETs), there are substantial gaps in the published literature regarding cost-of-illness analyses, economic evaluation and budget impact analyses. Compounding the issue is that data on resource utilization and cost-effectiveness of different diagnostic and therapeutic modalities for GEP-NETs are scarce.
Methods:
A systematic review on the economic impact of GEP-NETs was carried out using four databases: EMBASE, PubMed, the National Health Service Economic Evaluation Database and Cochrane review. Fully published articles from January 2000 to May 2017, in English and Spanish, were included. All articles that satisfied the inclusion criteria were included in the systematic review; summary descriptive statistics were used to describe the methodological characteristics.
Results:
The 14 studies selected included cost-of-illness analyses (n = 4), economic evaluations (n = 7) and budget impact analyses (n = 3). Almost all studies were performed in the United States. Healthcare costs for patients with NETs included medication, outpatient visits, hospitalizations, and check-ups/tests. Reducing adverse events is an area where cost savings could be achieved; however, there was not enough evidence on the cost impact of adverse events.
Conclusion:
There is a lack of data related to resource utilization in the field of GEP-NETs. Therefore, cost-effectiveness and budget impact studies of existing and emerging treatments are urgently needed to help the decision-making process for patients with NETs.
Keywords
Introduction
Neuroendocrine tumors (NETs) are neoplasms arising from neuroendocrine cells which are distributed widely throughout the body. 1 These tumors can cause clinical conditions, including Zollinger–Ellison syndrome, hypoglycemia and watery diarrhea hypokalemia-achlorhydria (WDHA) syndrome, bronchospasms, flushing and other symptoms due to the release of specific hormones and neuroamines into the bloodstream. NETs localized to the gastrointestinal tract (GI-NETs) or pancreas (P-NETs) are collectively referred to as gastroenteropancreatic (GEP)-NETs.
The incidence of GI-NETs has consistently and significantly increased over the past three decades.2,3 During this time, estimates in the United States (US) have shown a 6.4-fold increase in incidence from 1973 to 2012 across all sites, stage and grades. 4 In some European countries, the annual GEP-NET incidence has reached 5.83 per 100,000 people. 5 This may reflect a true increase in the number of new cancers, or the impact of new or improved diagnostic tests and technologies. This increase in prevalence has resulted in a higher financial burden of this disease in European countries. According to the surveillance, epidemiology and end results (SEER) program registry data, prevalence of GEP-NETs is among the highest incidence rate, with 3.56 per 100,000 people in GEP sites and 0.84 per 100,000 people in NETs. 4
GEP-NETs are diagnosed at all stages; approximately 45.1% of diagnoses occur at the localized stage, 23.1% of diagnoses occur when the patient has metastases, while 16.5% occur when the patient has regional lymph node involvement. 4 In patients with P-NETs, advanced disease is particularly common at diagnosis; approximately 60% of patients are diagnosed at a metastatic stage. 6 Clinical management of GEP-NETs is also challenging due to the heterogeneous nature, anatomical location, and clinical course of these tumors. Clinical interest in GEP-NETs has substantially increased in recent decades, possibly due to the development of novel diagnostic and therapeutic modalities, including targeted agents. Despite the current interest and enthusiasm for classical and newly developed therapies for GEP-NETs, data on economics, including cost-of-illness, budget impact and economic evaluations of different diagnostic and therapeutic modalities are scarce.
In an era of healthcare budget restrictions, this information is crucial for decision-making of patient management and resource allocation. In an increasing number of countries, new healthcare interventions must show clinical efficacy and cost-effectiveness before reimbursement or addition to formularies. This increased emphasis on demonstrating value for money using economic evaluation has arisen because of the increased pressures on healthcare expenditure in health services, driven largely by demographic changes, increased patient expectations and the rapid development of technology. Economic evaluation to assess the cost-effectiveness of medicines has been widely labeled as the ‘fourth hurdle’ to market, in addition to the traditional three hurdles of safety, efficacy and quality, required for the licensing of a new medicine. While pharmacoeconomics is undoubtedly useful for purchasers, it does not address the issue of affordability, which is an increasing concern. 7 Healthcare purchasers are not only concerned with maximizing efficiency but also with remaining within their annual budgets. These two objectives are not always consistent. Therefore, there is a role for both economic evaluation and budget impact analyses to independently inform healthcare decision-making. The complementary role of these approaches has already been recognized by some decision-making bodies.8,9
The aim of this paper was to review the recent literature on the pharmacoeconomics of GEP-NET diagnostics and management strategies, as such, the cost-of-illness, economics and budget impact evaluations and to identify gaps in knowledge to guide decision-making in the management of these tumors.
Methods
The systematic literature review used four databases: EMBASE, PubMed, the National Health Service (NHS) Economic Evaluation Database and Cochrane reviews. The articles were searched in these databases by title and abstract using two different groups of keywords. In order to select the search terms, we considered the Health Information Research Unit at McMaster University (Hamilton, ON, Canada), which specified the search filters for MEDLINE (in Ovid syntax) and the PubMed translation, and the NHS Centre for Reviews and Dissemination, which also specified the recommended search terms in a systematic search. Therefore, the following search terms were used: [(neuroendocrine AND tumor) OR (neuroendocrine AND tumo*) OR (neuroendocrine AND neoplas*) OR (carcinoid AND tumo*) OR (carcinoid AND syndrom*)) AND ((cost AND benefit*) OR (cost AND effect*) OR (cost AND utilit*) OR (cost AND minim*) OR cost* OR (economic AND evaluation*) OR economic* OR (budget AND impact) OR (economic AND impact) OR (resource AND util*)]. Grey literature was included from a search in Google Scholar; in addition, other papers were included using citation tracking from the retrieved and selected papers.
The systematic review followed recommendations of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines on reporting systematic reviews. 10 Papers published from January 2000 to May 2017, in English and Spanish, were included. Exclusion criteria comprised studies that were: neither cost-of-illness analyses, nor economic evaluations, nor budget impact analyses; economic evaluations that were not completed (and therefore did not include the incremental cost-effectiveness ratio); reviews; not focused on the disease of interest; and only published as an abstract. A data extraction form included questions on the studies’ context (e.g. geographical study location), sampling and sample characteristics (e.g. disease), methods and results (e.g. type of costs, measure of outcome, perspective) and conclusions (e.g. results summary, study funding). The first screening was conducted by two researchers. Subsequently, each abstract and paper selected was reviewed by two investigators and data extraction was performed independently. The decision for inclusion of an article in the review was made by agreement among other experienced investigators. Whenever there was a disagreement, the papers were reviewed by another investigator. Microsoft Excel was used to summarize the results from the systematic literature review.
After all articles that satisfied the inclusion criteria were collected, summary descriptive statistics were used to describe the methodological characteristics. Costs were converted to 2017 Euros (€) using country-specific or country-group-specific inflation on average consumer prices. 11 The annual costs and mean unit values were adjusted by the interannual inflation rate from the price year to 2017. If required, the unit and annual costs from 2015 were multiplied by the European Central Bank’s 2017 exchange rates. For papers not reporting the year in which the costs were calculated, the publication year was used.
Results
The search identified a total of 288 studies. Of those, 30 studies were duplicates and were excluded. Of the remaining studies (n = 258), 222 were excluded because they were congress abstracts, or not associated with NETs. A total of 36 articles that met the initial inclusion criteria were included in the full-text review. Finally, eight studies were selected, which consisted of cost-of-illness analyses (n = 4); economic evaluations (n = 3) and budget impact analyses (n = 1), shown in Figure 1.

Flow chart search strategy.
The number of publications about the economics of GEP-NET diagnostics and therapies trended upwards from 2012, with five out of eight included studies published since 2015. Details of the cost-of-illness, economic evaluations and budget impact analyses are summarized in Tables 1, 2, and 3, respectively. Almost all studies (seven out of eight) were conducted in the US, except one economic evaluation which was conducted in Mexico. The average age, weighted by sample size, of populations included was 53 years, although only two out of eight studies reported age. All studies specified the diagnosed disease of patients included, which were: carcinoid syndrome (CS; n = 3), NETs in general (n = 2), P-NETs (n = 2), GI-NETs (n = 2), lung NETs (n = 2), and pancreatic islet cell tumors (n = 1). Half the studies indicated the degree of severity of diagnosed diseases. None of the economic evaluations and cost-of-illness studies specified whether or not patients included in the study had received previous treatments. Overall, two of three economic evaluations and three of four cost-of-illness analyses were based on clinical trials.
Summary of cost-of-illness studies (n = 4).

NS, not stated.
Summary of economic evaluations (n = 7).
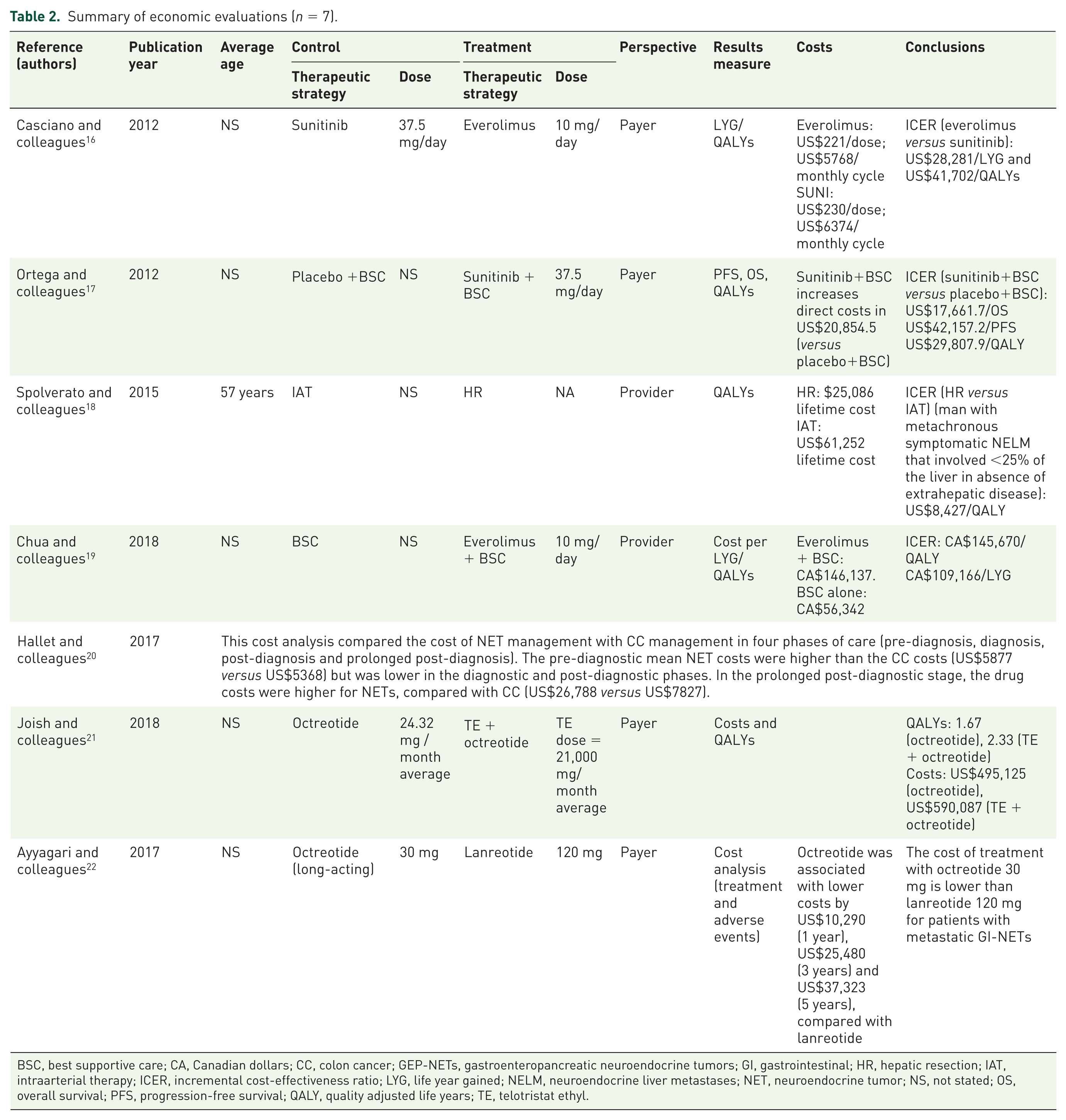
BSC, best supportive care; CA, Canadian dollars; CC, colon cancer; GEP-NETs, gastroenteropancreatic neuroendocrine tumors; GI, gastrointestinal; HR, hepatic resection; IAT, intraarterial therapy; ICER, incremental cost-effectiveness ratio; LYG, life year gained; NELM, neuroendocrine liver metastases; NET, neuroendocrine tumor; NS, not stated; OS, overall survival; PFS, progression-free survival; QALY, quality adjusted life years; TE, telotristat ethyl.
Summary of budget impact evaluations (n = 3).

LAR, long-acting release; NS, not stated; SSA, somatostatin analog; TE, telotristat ethyl; US, United States.
Cost-of-illness analysis
In terms of economic burden or cost-of-illness analysis, four studies were found.12–15 Overall, two articles investigated the resource utilization or economic burden generated in patients treat-ed for NETs;12,13 two articles examined the economic impact of reduction of adverse events, such as diarrhea, in patients with CS (Table 1).14,15
Both studies that analyzed treatments for NETs also evaluated pharmacological and chemotherapy treatments; the economic burden was not calculated using a decision analysis because the time horizons for the analyses were 1 and 3.5 years. Therefore, there was no need to do complex long-term cost estimations. Strosberg and colleagues 12 reported primary data and carried out a deterministic and probabilistic sensitivity analysis, but did not report the perspective of analysis, whereas Chuang and colleagues 13 reported secondary data, used the National Health System and patient perspectives, but did not report the perspective of the analysis. In both studies, the costs included were medication, outpatient visits, hospitalizations, and diagnostic tests. Stroberg and colleagues 12 concluded that advanced NET progression had an impact on resource utilization regardless of tumor site, particularly with respect to hospitalizations, surgeries, imaging and lab tests, chemotherapy and somatostatin analogs (SSAs). The authors also suggested that more research was necessary to elucidate differences in adverse event reporting between patients receiving chemotherapy versus targeted agents. Chuang and colleagues 13 highlighted the existence of economic impact among individuals with NETs and pointed out the importance of investigating the economic burden of patients with longer follow up in the future.
Of the two studies that examined resource utilization associated with adverse events in patients treated for NETs,14,15 neither used a decision analysis to estimate the costs generated. Broder and colleagues 14 evaluated a retrospective database with a time horizon of 10 years and Huynh and colleagues 15 analyzed data for a 1-year follow up. The latter study also conducted a deterministic sensitivity analysis. Both studies included costs on medication, outpatient visits and hospitalizations; it was concluded that adverse events, such as diarrhea associated with CS, accounted for higher total healthcare spending compared with no adverse events. In addition to these savings, the improvement of quality of life should be also taken into account. Therefore, healthcare costs could be reduced if effective preventive treatment for adverse events associated with pharmacological treatments for NETs could be used.
Economic evaluation
Of eight economic evaluations, seven were on pharmacological treatment.16,17,19–22 The remaining study analyzed a surgical strategy (Table 2). 18 Only one study compared pharmacological therapies with equivalent doses. 16 Most studies that evaluated pharmacological treatment provided dosing information of the intervention group, with the exception of Hallet and colleagues. 20 Cost-effectiveness was evaluated in all analyses, except those conducted by Hallet 20 and Ayyagari and colleagues, 22 which used cost analysis. A total of four studies used a Markov model to estimate costs and health outcomes.16–18,21 The time horizons were established as 5 years, 22 10 years,16,17,19 and a lifetime18,21 or were not specified. 20 Overall survival and quality adjusted life years (QALYs) were used across six studies. Overall, four studies used the National Health System perspective,16,17,21,22 whereas two studies used the provider perspective.18,19 All costs and outcomes were discounted according to the recommended rate in each country. All studies included costs such as medication; outpatient visits hospitalizations, check-ups and tests. These costs were the same as those included in studies of economic burden. The incremental cost-effectiveness or cost-utility ratios were specified in seven studies16–22 and were all below the cost-utility threshold recommended for that particular country, which indicated the cost-effectiveness of the intervention. A probabilistic and deterministic sensitivity analysis was performed in all studies, although the acceptability curve was detailed in only four studies.17–19,21
Budget impact
Rose and colleagues 23 assessed the budget impact of everolimus for the treatment of GI-NETs and advanced or metastatic lung NETs and established the total population using prevalence data, although no data was provided regarding the percentage of patients diagnosed and treated (Table 3). The authors established a clear comparison between the current scenario without everolimus on the market for GI-NETs and the potential scenario with everolimus on the market. The same scenarios were built for lung NETs. The total budget impact on a US managed healthcare plan and a pharmacy budget was evaluated. The time horizon for both perspectives was 3 years. In the first perspective, costs included drug therapies, other cost of treatment, treatment administration, hospitalizations, physician visits and monitoring/management of adverse events. Costs included in the second perspective only included the drug therapy costs. The total budget impact and the impact on pharmacy budget were expected to increase in GI-NETs and lung NETs with the introduction of everolimus, although the changes were minimal. For GI-NETs, in the first 3 years, the difference between having everolimus on the market or not was 0.0568 and 0.1443 cents per member per month (PMPM), resulting in a −0.0875 cent PMPM difference, and for lung NETs 0.0181 cents and 0.0355 cents PMPM, resulting in a −0.0174 cent PMPM difference. A deterministic univariate sensitivity analysis was carried out in order to study the impact of a 10% variation in drug costs, treatment duration, number of patients eligible for treatment, and new treatment market share. The most significant impact was caused by drug price and treatment duration, which were expected to alter the budget impact by a magnitude of 2.04 cents PMPM and 0.79 cents PMPM in the third year after launch for GI-NETs and lung NETs, respectively. According to the sensitivity analysis of the budget impact model, the impact of drug costs and treatment duration is greater for GI-NETs, compared with lung NETs. 23
In the evaluation of the short-term affordability of reimbursing telotristat ethyl for CS diarrhea in patients who were not controlled with long-acting release SSAs, the net budget impact of was found to be minimal to a US health plan. The incremental cost PMPM of reimbursing telotristat ethyl was US$0.013, US$0.019 and US$0.025 for 1, 2 and 3 years, respectively. 24
Furthermore, a model-predicted per-patient cost for SSAs was US$83,473 and US$89,673, for lanreotide and octreotide, respectively, for patients with locally advanced or metastatic GEP-NETs. 25
Discussion
Despite new treatment approvals, representing important therapeutic advances, there are substantial gaps in the published literature in the understanding of several key domains relevant to the economics of NETs, particularly with respect to cost-of-illness, economic evaluation and budget impact. The present systematic review highlights the scarcity of data on resource utilization in patients with GEP-NETs.
A previous systematic review on resource utilization in NETs was performed to review available data in advanced NETs for cost-of-illness/resource utilization, economic studies/health technology assessment and quality of life. 26 Chau and colleagues found a lack of consistent and comprehensive documentation of resource utilization in the management of NETs. 26 It could be argued that diagnosis and surgical resection (primary treatment) and therapeutics should be treated as separate categories. However, despite the relevance of separating these categories the lack of evidence on the economic burden of NETs still remains a problem.
There is a lack of studies that quantify the potential cost reduction associated with CS symptom resolution or improvement, following treatment of patients with NETs. In addition, patients with NETs have significantly higher rates of mortality and hepatic and gastrointestinal morbidities, compared with patients without NETs. 27 There is a need to quantify this burden economically in order to have a clear picture of the total economic burden.
Due to the limited number of studies, robust conclusions could not be drawn in terms of effectiveness of pharmacological therapies. Further cost savings may be achieved by reducing adverse events, however, there is currently not enough evidence on the cost of adverse events and more studies are required in this field. The conclusions from the economic evaluations in this review highlight the lack of data on the estimated utilities of different health states among patients with NETs. While it is optimal to compare pharmacological therapies in head-to-head trials, due to data restrictions, indirect comparisons may still provide useful information.
Since 2009, pharmacological treatments of NETs28–32 have demonstrated improvements, in progression-free survival and overall survival, compared with placebo,33–35 although some patients had drug-related adverse events, such as diarrhea, fatigue and respiratory infections. The use of lanreotide 30 and telotristat ethyl31,32 can improve symptoms of CS in NETs. This review showed that there was enough published evidence to conduct further research into the effectiveness of these treatments taking in account direct healthcare costs, such as the drug-related events, direct nonhealthcare related costs and productivity losses. The latter two are important for this type of disease due to the high degree of dependency on family members and impact on caregivers, which contributes to the cost of illness from a societal perspective. 36 If the differences in terms of additional health benefits between available treatments are not significant, this implies that the end differences on drug price are going to be relevant in order to convince decision-makers to publicly fund these types of treatments. In this sense, studies on the treatment costs for different options37,38 are useful in clarifying the direct healthcare costs of these treatment options.
Some research concluded that surgical therapy is the only curative treatment in individuals with NETs and when adequately indicated, no further treatment is need, thereby reducing future healthcare resource use and costs. 39 However, with innovative pharmacological treatments, more evidence of resource utilization with longer follow up is needed to evaluate and compare healthcare resource utilization and the economic burden of surgery and pharmacological treatments. Other costs such as productivity losses have also not been evaluated. 13 Therefore, more research is required to evaluate the overall impact on the economic burden of NETs.
Regarding the limitations of the present review, its main weaknesses are due to the limited available data included in the identified literature. However, the review of existing international data has resulted in a clearer picture of the current burden of the disease that can be useful to inform clinical and healthcare policy decisions. The limitation of the budget impact study was the availability of data found only in the US. Costs and prices may not be generalizable to other countries or health systems. Another limitation included uncertainty surrounding some of the most important inputs used in this analysis. Prevalence estimates were not accurate enough in order to do fair approximations of the real number of patients diagnosed with NETs. The number of patients with progressive tumors is not available in the published literature and there is no available information from real-world studies. Moreover, there was a lack of evidence on the estimation of treatment market share and treatment duration. Specific estimates of healthcare resource utilization associated with each therapy were not available; therefore, the results might be affected by the uncertainty of these parameters. The lack of real estimates and data might indicate that the 10% of variation used to run a deterministic sensitivity analysis might be not enough in order to estimate the potential uncertainty around these model results.
In conclusion, management of advanced GEP-NETs has changed substantially in the past few decades due to improved diagnostic tests and increased availability of targeted treatments; further economic evaluations are required to inform healthcare decision-making.
Supplemental Material
PRISMA_2009_Checklist_03Oct18_TC_Ok – Supplemental material for Economics of gastroenteropancreatic neuroendocrine tumors: a systematic review
Supplemental material, PRISMA_2009_Checklist_03Oct18_TC_Ok for Economics of gastroenteropancreatic neuroendocrine tumors: a systematic review by Enrique Grande, Ángel Díaz, Carlos López, Javier Munarriz, Juan-José Reina, Ruth Vera, Beatriz Bernárdez, Javier Aller, Jaume Capdevila, Rocio Garcia-Carbonero, Paula Jimenez Fonseca and Marta Trapero-Bertran in Therapeutic Advances in Endocrinology and Metabolism
Footnotes
Acknowledgements
The authors thank Rudi Subirà Gómez, Sara González and Marc Gil Fornaguera for their contribution to this manuscript. The authors also thank Mimi Chan, PhD, of Springer Healthcare Communications, who edited this manuscript for English language. This medical writing assistance was funded by Novartis Pharmaceuticals.
Funding
This work was funded by Novartis Pharmaceuticals. The funder had no influence over the conduct of this study or the drafting of this manuscript.
Conflict of interest statement
E.G. received honoraria as a speaker, and participated in advisory boards at Novartis, Pfizer, IPSE, Adacap and Lexicon. All other authors have no conflicts of interest to declare.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.