
Abstract
Objective
Bronchiectasis is a common chronic airway disease. We investigated the economic burden and associated factors of bronchiectasis in China.
Methods
In this multicenter retrospective cohort study, we reviewed medical records of patients admitted to 18 tertiary hospitals during 2010 to 2014 with a bronchiectasis-related diagnosis.
Results
A total 5469 patients with bronchiectasis were admitted, accounting for 3.13% ± 1.80% of all discharged patients with any diagnosis during the same period; 13 patients died upon discharge. The median hospitalization cost was RMB 8421.52 (RMB 5849.88–12,294.47). Risk factors associated with hospitalization costs included age at admission (>70 vs. <40 years, odds ratio (OR) = 1.221, 95% confidence interval (CI) = 1.082–1.379; >80 vs. <40 years, OR = 1.251, 95% CI = 1.089–1.438), smoking (≤15 packs/year vs. non-smokers, OR = 1.125, 95% CI = 1.006–1.271; >15 packs/year vs. non-smokers, OR = 1.127, 95% CI = 1.062–1.228), length of hospitalization (OR = 1.05, 95% CI = 1.046–1.054), combination antibiotic treatment (OR = 1.089, 95% CI = 1.033–1.148), cough (OR = 0.851, 95% CI = 0.751–0.965), dyspnea (OR = 0.93, 95% CI = 0.878–0.984), chronic obstructive pulmonary disease (OR = 0.935, 95% CI = 0.878–0.996), respiratory failure (OR = 0.923, 95% CI = 0.862–0.989), cor pulmonale (OR = 0.919, 95% CI = 0.859–0.982), and death (OR = 1.816, 95% CI = 1.113–2.838).
Conclusions
Age, smoking status, symptoms, and respiratory comorbidities were associated with hospitalization costs of bronchiectasis.
Keywords
Introduction
Bronchiectasis is a chronic airway disease characterized by permanent structural bronchial dilation, which can be triggered by both congenital and acquired causes, the latter being more common. Cystic fibrosis (CF) accounts for up to 50% of patients, which is rare in the Asian population. Bronchiectasis without CF is known as non-CF bronchiectasis. 1 Non-CF bronchiectasis is characterized by recurrent exacerbations and persistent airway inflammation. Non-CF bronchiectasis leads to neutrophilic airway inflammation, impairment of pulmonary host defenses, and repeated bronchial infection.2,3 Patients have chronic bacterial infections, which can result in chronic sputum, cough, shortness of breath, worsened quality of life, and potentially life-threatening hemoptysis. Recent studies from the United States and Europe have shown that the prevalence and incidence of non-CF bronchiectasis is substantially higher than previously reported.4,5 In China, bronchiectasis is a frequently seen chronic respiratory disease that can affect the quality of life and life expectancy of the affected individual. 6 Between 2002 and 2004, an urban population-based and cross-sectional survey of bronchiectasis conducted in China showed that the overall prevalence of physician-diagnosed bronchiectasis in people age ≥40 years was 1.2%, 7 which was higher than the incidence recently reported in the United States and Europe.4,5
Studies have focused on characteristics of bronchiectasis such as the etiology,8,9 lung function impairment, 10 and infectious agents,11,12 since the first Chinese guideline for the diagnosis and management of bronchiectasis was published in 2012. 13 However, the economic burden associated with bronchiectasis remains unknown. 14 Therefore, we performed this study to elucidate the economic burden and related factors of hospitalized patients with bronchiectasis in China based on a multicenter retrospective cohort study. The results may provide important guidance for the management of bronchiectasis and for the allocation of resources in health care.
Methods
Ethical approval
This study was supported by the Chinese Association of Chest Physicians (CACP). The study protocol was approved by the institutional review boards at all involved institutions (No. 2015PHB202-01). Written informed consent was not required from patients because this study was based on anonymous and publicly accessible data.
Study design
This retrospective, multicenter study included hospitalized patients diagnosed with non-CF bronchiectasis.
Patients and inclusion criteria
Patient data were collected from 18 CACP member hospitals for inclusion in this retrospective study. All hospitals were tertiary hospitals in different provinces across China, and all had the equipment needed to perform high-resolution computed tomography (HRCT) for routine diagnosis of bronchiectasis. HRCT images were evaluated to record the sites (within six lobes; the lingula segment was considered a separate lobe) and types (cystic, columnar, mixed) of bronchial dilation.
The inclusion criteria were: 1) discharged from a respiratory and critical care medicine department between 2010 and 2014; and 2) diagnosed with bronchiectasis, exacerbation of bronchiectasis, bronchiectasis with hemoptysis, or bronchiectasis with infection at discharge. For hospitals that have more than one separate inpatient area within the department of respiratory and critical medicine, patients discharged from one particular inpatient area were included. We excluded patients age <18 years.
Data collection
An electronic form generated using EpiData software, version 3.1 (EpiData Association, Denmark) was used to collect demographic data, clinical data, and cost variables for included patients from the 18 hospitals participating in this study. The medical records of all included patients were retrospectively reviewed, and the following data were extracted: 1) clinical characteristics including demographic data, initial symptoms at admission, duration of symptoms, smoking history, cause of bronchiectasis, physical examination findings, and respiratory comorbidities; 2) laboratory results including blood routine testing, sputum smears, and culture; 3) predicted percentage of forced expiratory volume in 1 s (FEV1/pred), and forced expiratory volume in 1 s/forced vital capacity (FEV1/FVC); 4) duration, application route (intravenous, oral, intravenous sequential oral), type, and dose of antibiotics; and 5) length of hospital stay, cost of hospitalization, and the outcome at discharge.
Statistical analysis
Statistical analysis was performed using IBM SPSS, version 20.0 (IBM Corp., Armonk, NY, USA). Normality and homogeneity of variance tests were determined for the measurement data. Normally distributed data are represented as mean ± standard deviation (SD); non-normally distributed data are represented as median (Q1, Q3). Numerical data are represented as frequency (percentage). The associated relative risk was estimated as the odds ratio (OR) with a 95% confidence interval (CI). Using MLwiN software version 2.30 (Centre for Multilevel Modelling, University of Bristol, UK), we applied a multilevel linear model to analyze the risk factors associated with cost. Two-tailed P<0.05 was considered statistically significant.
Results
Study population
From 2010 to 2014, 5469 patients with bronchiectasis were hospitalized 5915 times in the respiratory departments of the 18 designated hospitals; 342 patients hospitalized more than once (Figure 1). The hospital locations included: Baotou, Inner Mongolia (n = 148): Beijing (n = 214): Binzhou, Shandong (n = 148): Cangzhou, Hebei (n = 455): Kunming, Yunnan (n = 24): Nanchong, Sichuan (n = 436): Dalian, Liaoning (n = 981): Yulin, Guangxi (n = 333): Chengdu, Sichuan (n = 367): Jinhua, Zhejiang (n = 75): Jinzhou, Liaoning (n = 522): Nanchang, Jiangxi (n = 512): Linyi, Shandong (n = 46): Changzhi, Shanxi (n = 99): Shanghai (n = 101): Xian, Shanxi (n = 91): Urumchi, Xinjiang (n = 650): and Zunyi, Guizhou (n = 713).

Flow diagram of the study including 5469 patients hospitalized 5915 times.
Additional information for patients discharged from the same inpatient area during the same period was provided by 15 hospitals. Among 247,648 patients who were discharged during 2010 to 2014, 5266 (3.13% ± 1.80%) were diagnosed with bronchiectasis.
Demographic data and clinical features
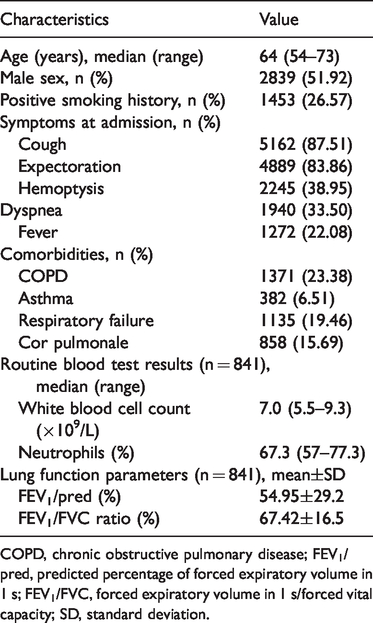
Demographic data of the included patients are shown in Table 1. The mean patient age was 62.91 years, and male patients (51.92%) predominated. A total 1453 patients (26.57%) had a history of smoking.
Baseline characteristics of the 5469 included patients hospitalized for treatment of bronchiectasis.

COPD, chronic obstructive pulmonary disease; FEV1/pred, predicted percentage of forced expiratory volume in 1 s; FEV1/FVC, forced expiratory volume in 1 s/forced vital capacity; SD, standard deviation.
Infectious agents identified in sputum examination
Sputum culture was performed in 2907 cases, and 1321 sputum samples from 1259 individuals showed the presence of potentially pathogenic microorganisms. Pseudomonas aeruginosa was the most frequently observed microorganism (n = 399, 30.2%), followed by Streptococcus pneumonia in 88 patients (6.66%), Klebsiella pneumonia in 50 patients (3.78%), Haemophilus influenza in 11 patients (0.83%), and Staphylococcus aureus in 10 patients (0.75%). Among the 2759 cases with sputum smears, 14 specimens stained positively by Zeihl–Neelsen acid-fast stain.
Localization of infection
The results of HRCT examination were recorded for 5147 patients (Table 2). More than one lobe was affected in most patients (i.e., the lingula segment was considered a separate lobe), and 677 patients (13.16%) had involvement of all six lobes. The lower lobe of the left lung (3302 patients, 64.15%) was the most common site of infection. Cystic dilatation (2145 patients, 41.67%) was the most common type of lesion.
HRCT findings for 5147 patients hospitalized with bronchiectasis.

HRCT, high-resolution computed tomography.
Antibiotic use
Antibiotics were used in 5681 cases (96.04%) and administered intravenously in 5443 cases (95.81%). More than one antibiotic was used in 2465 (43.39%) cases. Cephalosporin was the most commonly used antibiotic (Table 3).
Type of antibiotics used in patients hospitalized with bronchiectasis.

Prognosis
The average length of hospital stay was 10.96 ± 5.86 days. In a total of 5735 cases (96.95%), the patient improved and was discharged from the hospital. However, 13 patients died, accounting for 0.24% of the total number of included patients.
Hospitalization expenses
The hospitalization expenses were recorded in 5288 cases from 17 hospitals. The median hospitalization cost was RMB 8421.52 (RMB 5849.88–12,294.47). The differences in average hospitalization cost among hospitals (median rate ratio, MRR = 1.2; proportional change variance (PCV%) = 25%) and individual patients (MRR = 1.48; PCV% = 56.85%) were statistically significant. A multilevel linear model analysis showed that the risk factors associated with increased hospitalization costs included age at admission (>70 years vs. <40 years, OR = 1.221, 95% CI = 1.082–1.379; >80 years vs. <40 years, OR = 1.251, 95% CI = 1.089–1.438), smoking (≤15 packs/year vs. non-smokers, OR = 1.125, 95% CI = 1.006–1.271; >15 packs/year vs. non-smokers, OR = 1.127, 95% CI = 1.062–1.228), length of stay (OR = 1.05, 95% CI = 1.046–1.054), combination antibiotic treatment (OR = 1.089, 95% CI = 1.033–1.148), cough (without cough vs. cough, OR = 0.851, 95% CI = 0.751–0.965), dyspnea (without dyspnea vs. dyspnea, OR = 0.93, 95% CI = 0.878–0.984), presence of chronic obstructive pulmonary disease (COPD; without COPD vs. COPD, OR = 0.935, 95% CI = 0.878–0.996), respiratory failure (without respiratory failure vs. respiratory failure, OR = 0.923, 95% CI = 0.862–0.989), cor pulmonale (without cor pulmonale vs. cor pulmonale, OR = 0.919, 95% CI = 0.859–0.982), and death (death vs. improvement, OR = 1.816, 95% CI = 1.113–2.838) (Table 4).
Multivariate logistic regression analysis of clinical features as risk factors associated with costs in 5288 patients with bronchiectasis.
OR, odds ratio; CI, confidence interval; BMI, body mass index; COPD, chronic obstructive pulmonary disease; FEV1/pred, predicted percentage of forced expiratory volume in 1 s; FEV1/FVC, forced expiratory volume in 1 s/forced vital capacity.
Discussion
This is the largest cohort study to date to investigate the economic burden of patients hospitalized with non-CF bronchiectasis in China. Patients hospitalized with bronchiectasis accounted for 3.13% ± 1.80% of all patients admitted to respiratory departments during the same period. This proportion was similar to that for patients with asthma in China, according to a previous study 15 in which patients hospitalized owing to asthma exacerbation accounted for 3.14% (6,480/206,135) of all respiratory department admissions in 29 hospitals. Although not a large-scale epidemiological survey, the present study provides evidence that bronchiectasis is a common reason for admission to respiratory wards. The demographic features and symptoms among patients included in this multicenter survey were similar to those described in our previous single-hospital study; 10 however, the rates of co-diagnosis with chronic obstructive pulmonary disease (COPD) or asthma were lower, and the rates of respiratory failure and cor pulmonale were higher than in our previous report.
The economic burden of bronchiectasis is substantial, with a mean annual cost (including both hospital and primary care costs) between USD 26,868 (in patients without exacerbation during 2008–2011) to USD 35,718 (in patients with exacerbation during 2009–2010), 16 which is higher than the average total annual medical care expenses reported for patients with COPD (USD 11,000–13,000) in the United States (US). 17 Hospitalization costs constitute a major economic burden associated with bronchiectasis. 18 In the US, the median expense for inpatient care was found to be USD 7827 for bronchiectasis-associated hospitalization in 12 states during 1999–2006. 19 In Spain, the total mean cost for the overall hospitalization period was EUR 5284.7 ± 2,445.7 during 2014 to 2015. 20 We also confirmed the heavy economic burden caused by non-CF bronchiectasis in China. The median hospitalization expense for each patient was RMB 8421.52 (RMB 5849.88–12,294.475), equivalent to USD 1269.07, which is lower than the hospitalization expenses reported for patients with COPD in China (RMB 14,828.47 in Tianjin during 2013, RMB 12,666.57 in Guangzhou during 2008). 21 The average length of hospital stay in our patients was 10.96 ± 5.86 days, which was nearly equal to that reported in Spain (10.8 ± 5.5 days). 20 In other countries, the average length of hospital stay in patients with bronchiectasis ranges from 2 to 17 days. 18 Thus, the hospitalization expenses of patients with bronchiectasis in China are lower than those in other countries, but the consumption of hospital-bed resources is similar.
We also investigated the influencing factors of hospitalization expenses. Although all the selected hospitals are tertiary hospitals, there were significant differences in hospitalization expenses among the different hospitals as these hospitals are distributed throughout different parts of the country. Older age, smoking history, longer length of hospital stay, combination antibiotic treatment, cough, dyspnea, presence of COPD, respiratory failure, cor pulmonale, and death were also key factors associated with higher expense. In our study, 23.38% of patients were co-diagnosed with COPD, which is similar to the rate described in a single-hospital study 10 and in other countries. 20 Respiratory failure and cor pulmonale were also common respiratory comorbidities in this multicenter survey. Bronchiectasis can cause severe respiratory system damage in patients. Measures should be taken to strengthen early identification, early intervention, and standardized management in patients with bronchiectasis, to reduce the occurrence of complications and thereby reduce the economic burden of disease.
Combination antibiotic treatment was another factor related to expense. Antibiotics were used in nearly all patients, and more than one antibiotic was used in nearly half of patients. Contrary to the extensive use of antibiotics, the rate of etiological diagnosis was very low. Therefore, most antibiotics were prescribed empirically and lacked bacteriological evidence. Isolation of potential pathogenic microorganisms may lead to more accurate targeted treatment. Thus, paying greater attention to pathogen screening and avoiding overuse of antibiotics may lower the economic burden of non-CF bronchiectasis.
Despite age and symptoms such as dyspnea, other important factors are predictive of bronchiectasis prevalence such as body mass index (BMI), FEV1, previous hospitalization, exacerbation frequency, colonization status, and radiological findings, as included in the FACED bronchiectasis prognostic score 22 and Bronchiectasis Severity Index (BSI). 23 The annual cost of treatment has been found to be higher in patients with bronchiectasis who have more severe bronchiectasis, older age, more comorbidities, lower FEV1, more exacerbations or hospital admissions, chronic bronchial infection with P. aeruginosa, and an association with COPD. 24 However, BSI was not related to the cost of hospitalization in Spain. 20 We also did not find a relationship between the cost of hospitalization and BMI, FEV1, and radiological findings. Therefore, these factors may have a greater influence on prognosis and expenses during stable periods but have less influence on expenses during periods of acute exacerbation.
Several limitations in this study should be considered when interpreting the results. As a retrospective study, many important parameters such as exacerbation events, severity of symptoms, predisposing factors for bronchiectasis, and other complications beyond the respiratory system, which may be associated with an increased economic burden, were not documented in most medical records. Colonization by P. aeruginosa is related to more frequent exacerbations, a greater number of hospital admissions, prolonged hospital stay, and poor lung function, 25 and has been considered an important factor that is independently associated with a higher overall cost of hospitalization. 20 Owing to the low positive rate for potential pathogenic microorganisms among our patients, we did not include colonization status in the multivariate analysis. In Spain, the high costs among patients with colonization by P. aeruginosa was correlated with the use of inhaled antibiotic treatment, 20 which is unavailable in China at present; therefore, we are still unable to determine the impact of P. aeruginosa colonization on hospitalization expenses in China. Moreover, we did not include patients admitted to the intensive care unit, so as to obtain a homogeneous sample. Therefore, a prospective study involving more investigation centers is needed, to improve our understanding of the burden caused by non-CF bronchiectasis and its management in China.
In conclusion, non-CF bronchiectasis is a common reason for patient admission to the departments of respiratory or critical care medicine, which leads to a heavy economic burden. Early intervention to prevent the occurrence of respiratory complications and accurate targeted antimicrobial therapies may be effective ways to reduce hospitalization expenses owing to bronchiectasis.
Footnotes
Acknowledgements
We thank Qianqian Sun from People’s Hospital, Peking University and Xinying Zeng from the Chinese Center for Disease Control and Prevention for competent and kind assistance in data processing.
Authors’ contributions
All the authors participated in the study design, acquisition and analysis of the data, the statistical analyses, and writing of the manuscript. All authors reviewed and approved the final manuscript.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This work was supported by a grant from the Beijing Higher Education Young Elite Teacher Project (YETP0071).