
Abstract
Background:
Despite the known detrimental socio-economic consequences of leprosy morbidity, disability and social exclusion at the household level, research investigating the precise economic burden of leprosy remains scarce. This study aims to address this gap by examining the socio-economic burden of leprosy in Ho municipality in the Volta Region of Ghana.
Methods:
This was a cross-sectional cost of illness study, and quantitative data were collected from leprosy patients between October and December 2023. Data collected included socio-demographic characteristics, direct and indirect costs related to treatment of leprosy from the patient’s perspective. Stata version 14 was used for the analysis.
Results:
A total of 35 respondents participated in the study, comprising 51.43% females and 48.57% males. All respondents (100%) reported having a valid National Health Insurance Scheme membership. The average total cost of leprosy treatment per patient, encompassing both direct and indirect expenses, was US$361.54 (SD ± 286.87). Disaggregating this cost further revealed a medical cost of US$44.30, a non-medical cost of US$47.07 and an indirect cost of US$290.16. The estimated annual household income of respondents was US$446.4 and 60% of respondents incurred expenditure that was more than 10% of their annual income and were deemed to have experienced catastrophic payment. Patients with sequelae incurred additional costs of US$46 (range: US$8.3–US$166.7) per case.
Conclusion:
The costs of treating leprosy were considerably high leading to catastrophic health payments. This highlights the need for an all-encompassing strategy that addresses medical, non-medical and indirect costs. Implementing targeted support programs and ensuring medication affordability are key steps towards mitigating the economic susceptibility of leprosy patients and facilitating successful treatment outcomes.
Background
Leprosy (Hansen’s disease), which is one of the Neglected Tropical Diseases, is a chronic infectious disease that normally affects the peripheral nerves, the skin, the eyes and parts of the upper respiratory tract and hence recognized as the major cause of permanent physical disability among communicable diseases. It is caused by Mycobacterium leprae and comes in two clinical forms: multi-bacillary (MB) and pauci-bacillary (PB). Leprosy is a curable disease and the current recommended treatment regimen consists of three drugs: dapsone, rifampicin and clofazimine. The combination is referred to as multi-drug therapy (MDT). The duration of treatment is 6 months for PB and 12 months for MB cases. 1 Apart from the physical deformity, persons affected by leprosy also face stigmatization and discrimination. 2 According to the World Health Organization (WHO), 120 nations record about 200,000 new cases annually.1,3 Even though Ghana achieved the WHO target for eliminating leprosy as a public health concern – defined as less than one case per 10,000 inhabitants 1 – over 2 decades ago, the country has continued to record new leprosy cases yearly. Between 2017 and 2022, 258, 276, 279, 261, 263 and 277 new cases were detected, respectively. 4
Despite the known deleterious socio-economic ramifications to households of leprosy-related morbidity, disability and social exclusion, very few studies have been conducted on the socio-economic burden of leprosy. These few studies reported the substantial economic burden of leprosy treatment to households. For instance, Xiong et al. 5 investigated the economic cost of leprosy among migrants and residents in the Guandong Province of China and found that the annual treatment cost of leprosy after diagnosis was US$300.6 among migrant patients and that of resident patients was US$309.7. Tembei et al. 6 also found that leprosy reduced the number of working days by 115 days in the Northwest Region of Cameroon.
To the best of our knowledge, no study has investigated the socio-economic burden of leprosy in Ghana. Investigating the socio-economic burden of leprosy is very important because even though patients are supposed to get free treatment for leprosy in Ghana, and despite the existing National Health Insurance Scheme (NHIS) covering over 95% of disease conditions in the country, there are reports of patients incurring direct and indirect costs in seeking care. 7 This study therefore sought to investigate the socio-economic burden of leprosy in the Ho municipality in the Volta Region of Ghana.
Methods
Study site
The study was conducted in the Ho municipality in the Volta Region of Ghana. The Ho municipality is the capital of the Volta Region. Ho Municipal is one of the 18 districts in Volta Region. The main ethnic group in the municipality is Ewe. According to the 2021 population census, the Ho municipality has a population of 180,420 with a total area of 573.2 km2. The Volta Regional Health Directorate reported leprosy cases in the Volta Region from 2016 to 2021 as 30, 35, 27, 23, 21 and 29, respectively. 8 In the Ho municipality, in the past 5 years, there have been an average of 10 leprosy cases reported annually in the Ho municipality. 8
Study design
This was a cross-sectional study design, and data were collected using a quantitative approach between October and December 2023.
Data collection
Two graduate-level data collectors with experience in data collection were trained for the data collection. The data collectors were trained on the protocol and interviewing techniques. A structured questionnaire was used in the data collection for the study. The questionnaire (see Supplemental file 1) was developed using literature reviews2,5,9 –11 and pilot-tested. Pre-testing was conducted on five leprosy cases residing in the Hohoe District. These individuals were not part of the primary study area, Ho Municipality.
Data were collected with Tablets using the REDCap platform. Data collected included patient socio-demographics, health-seeking and cost of treatment. The questionnaire for the data collection was developed by reviewing relevant literature and incorporating insights from expert knowledge.
We collected general expenses during diagnosis and treatment which included the costs incurred by the patient to get the confirmed leprosy diagnosis and for each subsequent visit to the health facility for physical checks and collection of MDT drugs (free of charge). Extra expenses after the recommended 12-month treatment duration were defined as aftereffects (Sequela) or disease complications, such as lepra reactions, as well as the cost of physical and psychological rehabilitation. 5
Inclusion and exclusion criteria
Inclusion criteria:
• Laboratory-confirmed leprosy cases (both male and female) aged 18–80 years, with names recorded in the Disease Control Department register at the Municipal Health Directorate (MHD) in Ho. This includes both treated individuals and those currently undergoing treatment.
• Individuals diagnosed with leprosy within the period from January 2019 to December 2023.
• Individuals who provide consent to participate in the study.
Exclusion criteria:
• Cases of leprosy that are not confirmed by laboratory tests.
• Leprosy cases younger than 18 years or older than 80 years, as these age groups are either considered minors or potentially unable to provide accurate information due to age-related factors.
• Confirmed leprosy cases are not recorded in the Disease Control Department register at MHD in Ho, regardless of treatment status.
Individuals who refuse to provide consent to participate.
Sample size and sampling strategy
All individuals diagnosed with leprosy within a 5-year period (January 2019–December 2023) residing within the Ho municipality were considered eligible for study participation. A list of leprosy cases within the stipulated timeframe was sought from the MHD, Disease Control Department, Ho (treated and those under treatment).
The sample size was determined using the Krejcie and Morgan 12 table for determining sample size, which has been utilized in various studies.13,14 According to this method, with a known population of 40 leprosy cases recorded in the register during the specified timeframe, the estimated sample size was 36 cases.
A two-stage approach was applied to ensure that all respondents have fully consented to participate in the study. Prior to releasing the list of leprosy cases to data collectors, the leprosy focal person within the Disease Control Department contacted all individuals on the list to seek their informed consent for participation in the study. Out of the initial 40 cases identified, 35 individuals were successfully reached for consent acquisition. The remaining five cases could not be contacted due primarily to inaccurate or unavailable telephone numbers. Subsequently, all 35 consented leprosy cases were reached by the data collectors to conduct the interviews with them.
Data processing and analysis
Data were transferred from the REDCap platform to Stata 14 for analysis. Data cleaning by way of identifying outliers and checking for consistency among variables were carried out by running frequencies and cross-tabulations.
The cost of illness was analysed from the patient’s (household) perspective. Both direct and indirect costs due to leprosy treatment were analysed.15,16 The direct medical costs covered all Out-Of-Pocket-Payments (OOPPs) for consultation, diagnosis (laboratory) and medicines due to the treatment of leprosy not covered by the free leprosy treatment. The direct non-medical costs included all OOPPs for transportation to and from health facilities (patient and caregiver), special foods and lodging (including extra rent in the location of the health facility) due to the illness and for patients and caregivers associated with treatment.
Productivity costs often referred to as indirect costs are costs associated with lost or impaired ability to work attributable to illness.15,16 Productivity losses were estimated using the human capital approach, the most commonly used method for measuring productivity costs in health care.10,17,18 We used the average minimum daily wage of Ghana in 2023 of GHc14.88/USD1.2419 and multiplied by the number of days patients were unable to work due to the main leprosy treatment. In addition, we collected respondents’ reported monthly income and this was also analysed.
The total cost of treatment of leprosy was calculated by summing the direct and indirect costs incurred by patients.
Catastrophic health expenditure for leprosy was also calculated. Catastrophic payments occur when total OOPPs for health care exceed a certain threshold (typically between 5% and 40%) of a household’s resources (income or expenditure).20 –22 In this study, catastrophic payment was said to have occurred when the leprosy treatment cost was ⩾10% of the household’s annual income.
In addition, aftereffect (sequela) cost was estimated to determine how much cost leprosy patients still incur after the usual 12 months of MDT treatment.
To assess potential differences in socio-demographic variables relative to the total cost of leprosy treatment, factors such as age, sex, educational level, and occupation were evaluated utilizing the Kruskal–Wallis test.
All costs in the study were collected in Ghana Cedis (GHC) and converted into USD using the average exchange rate of 2023 (USD 1 = GHC 12). 23
Results
Table 1 presents the socio-demographic characteristics of respondents. As shown in the table, the total number of respondents was 35 and they were roughly balanced between females (51.43%) and males (48.57%). All respondents were Ewes (100%). The majority of the respondents (94.29%) were Christians, while a smaller minority (5.71%) were Muslims. The respondents were evenly distributed across marital statuses with 28.57% divorced, 28.57% married, 11.43% single and 31.43% widowed. The average age of respondents was approximately 56 years with the minimum being 27 years and the maximum being 79 years old.
Socio-demographic characteristics of respondents.

A high proportion of the respondents (45.71%) have never been to school while 28.57% had basic school education and 25.71% had senior high school education. Many of the respondents were unemployed (40.00%), followed by farmers (25.71%), artisans (17.14%), traders (11.43%), government employees (2.86%) and students (2.86%). All respondents (100%) reported having valid National Health Insurance (NHIS). The average monthly household income reported by respondents was US$41.08.
Cost of treatment
Table 2 presents insights into the economic burden of leprosy treatment, categorized into three main expense areas – non-medical, medical and indirect costs. Respondents reported receiving treatment for MB with MDT over a course of 12 months. This was done through monthly MB-MDT through Directly Observed Treatment (DOT) at health facilities. The treatment involved both direct and indirect costs.
Cost of treatment.
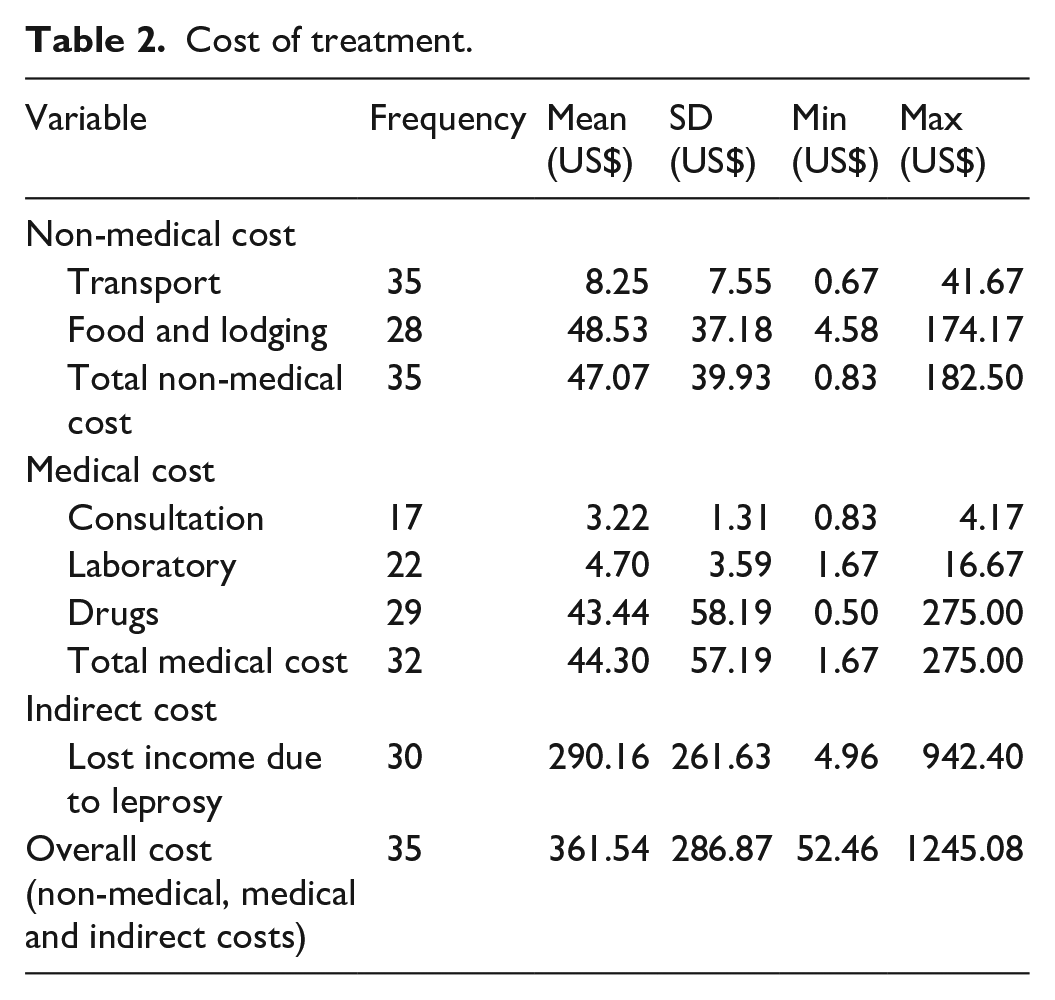
The average non-medical cost per patient was US$47.07. Examining this category in further revealed that patients incurred an average cost of US$ 48.53 per case on food and lodging. With regards to distance to the health facility for treatment, the majority used a taxi/motor tricycle to the health facility for treatment and 37.14% of respondents spent more than 1 h to the health facility (Figure 1). The average transport cost to the health facility and back using the taxi/motor tricycle was US$8.25.

Time spent to go to a health facility for treatment.
The average direct medical expenditure per patient was US$44.30. When we break this down further, the average cost of drugs was US$43.44, which accounts for the majority of medical expenses. While the primary leprosy treatment (MDT) is provided free of charge, respondents reported additional costs associated with managing their condition. These costs primarily stemmed from the purchase of analgesics (paracetamol, pain ointments), hydrogen peroxide and multivitamins. The average cost incurred on medications at the health facilities was US$25.42 while the cost incurred at the pharmacy shops was US$ 22.43.
The indirect cost associated with productivity loss was estimated at an average cost of US$290.16. Notably, 30 respondents (85.7%) reported being unable to work during treatment, with an average duration of work absence of 234 days (approximately 8 months).
The total cost, encompassing medical, non-medical and indirect expenses, was US$361.54 (SD ± 286.87). It is noteworthy that the indirect cost component, associated with productivity loss, was the largest contributor to this overall figure.
Cost by socio-demographic variables
Table 3 presents the results of a Kruskal–Wallis test examining the relationship between the cost of leprosy treatment and various socio-demographic variables. The results showed that the socio-demographic variables (age, sex, education and occupation) have no statistically significant association with the cost of leprosy treatment.
Cost of leprosy treatment by socio-demographic variables.

Catastrophic payment
Using the human capital approach, the average monthly household income was estimated at US$37.2 equivalent to an annual income of US$446.4 per respondent. The estimated income was almost the same as the average monthly household income reported by respondents as US$41.08.
Comparing the average treatment cost (US$361.54), 60% of respondents incurred expenditure that was more than 10% of their annual income and were deemed to have experienced catastrophic payments. When treatment expenditure was compared to monthly income, all households experienced catastrophic payments.
Aftereffect (sequelae)
Out of the 35 cases, 60% reported sequelae or other medical conditions after the treatment. Of the 21 cases, 57.14% reported high body temperature, 47.62% reported red skin patches, 33.33% reported sores on the skin and organs and 28.57% reported numbness in hands, feet, arms and legs as conditions they faced after the recommended 12 months of leprosy treatment (Figure 2). The average cost of treating these conditions was estimated at US$46 (range: US$8.3–US$166.7) per case.

Aftereffect conditions.
Discussion
Leprosy has been a persistent public health concern, and the disease is closely associated with poverty; therefore, understanding the economic implications of its treatment is crucial for developing targeted interventions. The study therefore sought to examine the economic burden of the treatment of leprosy to households in the Ho municipality in the Volta Region of Ghana.
This study determined the total cost of leprosy treatment to be US$361.54 per case, encompassing medical, non-medical and indirect expenses. Notably, when comparing the average treatment cost to the estimated annual household income of US$446.4, 60% of participants incurred expenses exceeding 10% of their annual income. This suggests that a significant portion of the study population experienced catastrophic health expenditure due to leprosy treatment. Furthermore, considering the average monthly income of respondents (US$41.08 or US$37.2), a figure significantly below the Ghanaian poverty line of US$1.90 per day (US$57 per month), 24 it is evident that all participants were living in poverty prior to incurring leprosy treatment expenses. The additional financial burden imposed by leprosy treatment is likely to further exacerbate their economic hardship. Our study’s cost of treatment (US$361.54) per patient is comparable to a previous study in China that reported leprosy treatment per patient to be US$300.6 (158.4–868.5). 5
The average medical cost of US$44.30 did not originate from the primary leprosy medication (MDT) because this medication is provided free of charge at government healthcare facilities. Rather, these costs stem from additional medications used to manage the condition, such as pain relievers, hydrogen peroxide, shampoo, etc. Importantly, these additional medications may not be available at the health facilities or not covered by the NHIS which will require OOPP. Medications not available at the health facilities are purchased at private pharmacies where the NHIS benefit package may not always be applicable. This finding aligns with previous studies demonstrating that NHIS members still incur significant OOPPs for medical care.11,22 This reinforces the observation that, in Ghana, even individuals enrolled in the NHIS scheme may continue to face substantial treatment costs.
The study showed that leprosy cases incurred an average non-medical cost of US$47.07, which highlights the substantial financial hardship faced by leprosy patients that extends beyond direct medical expenditures. This is consistent with many studies that reported higher non-medical costs than medical costs such as transportation, food and lodging. 25
Among the various cost components of leprosy treatment, food and lodging emerged as the most significant direct cost, accounting for US$48.53 per case. The substantial expenditure respondents incurred on food during treatment underscores the critical importance of food security in leprosy management, reflecting the well-recognized role of nutrition within the Ghanaian context. Having access to sufficient and nutritious food is a critical component of health, and this finding indicates the need for interventions that address not only medical costs but also nutritional needs during leprosy treatment in Ghana. If proper nutritional support is not given, it may even result in malnutrition given the leprosy patient’s relative susceptibility to food insecurity. 26 In addition, in Ghana, where healthcare facilities and accessibility may vary, ensuring affordable and accessible lodging for patients undergoing leprosy treatment becomes an important consideration. 27
The study revealed an average transportation cost (a component of non-medical expenses) of US$8.25 per round trip to the health facility, with respondents reporting travel times exceeding 1 h. Proximity to leprosy healthcare facilities therefore becomes crucial for effective disease management, as evidenced by prior research demonstrating an increased risk of disability at diagnosis among leprosy cases residing further from primary health care. 27
The income lost by patients due to leprosy, amounting to US$290.16, highlights the substantial indirect costs associated with the disease. The average number of days lost was 234 days (about 8 months) which is within the 6–12 months recommended guideline treatment duration for leprosy (6 months for paucibacillary; and 12 months for multibacillary).1,8 In the Ghanaian context, where livelihoods are often linked to manual work and agricultural activities, the income loss could have far-reaching implications for individuals and their families. This highlights how crucial it is to put social support programmes and efforts for vocational rehabilitation into place in order to lessen the socio-economic effects of leprosy. It has been reported that leprosy patients may face barriers to employment due to stigma, disability and treatment schedules, which can exacerbate their poverty cycle. 28 Similar to our findings, indirect cost has also been reported to be the largest cost component in leprosy treatment in a study in India. 10
Out of the 35 cases, 60% reported sequelae or other medical conditions which is not surprising as previous studies have reported high rates of after-effects of leprosy.5,9,10,29 The additional treatment cost for sequalae was US$46 (range: US$8.3–US$166.7) per patient. This amount is somehow comparable to the median yearly cost of leprosy complications of $69.5 (11–178.4) reported by Xiong et al. 5
Study limitations
This study potentially suffers from recall bias as respondents were asked to recall cost information over a 5-year period (January 2019–December 2023). This could lead to underestimation or overestimation of actual costs. However, it is worth noting that significant health expenditures impacting household resources are less likely to be forgotten, potentially mitigating the impact on overall results.
The small sample size may restrict the generalizability of the findings to the wider population. Nevertheless, this study’s findings are particularly relevant for a rare disease like leprosy and a starting point for other studies with large sample sizes.
The study did not include pre-diagnosis costs in the analysis due to concerns about recall bias. This decision might have led to an underestimation of the total treatment cost, as patients may incur significant expenses during consultations before receiving a confirmed leprosy diagnosis.
The study did not differentiate costs among leprosy patients with Grade 1 Disability (G1D) and Grade 2 Disability (G2D). This exclusion limits the understanding of how varying degrees of disability impact treatment costs. While the study acknowledges this limitation, the aggregated cost provides a general overview but might miss specific cost variations.
Despite these limitations, the study offers valuable insights into the economic burden of leprosy treatment in Ghana. It serves as a foundation for future research with larger, more representative samples and more comprehensive cost data collection methods.
Conclusion
The costs of treating leprosy were considerably high leading to catastrophic health payments. The study provides insights into the economic burden of leprosy treatment in the Ho Municipality of Ghana, highlighting the need for an all-encompassing strategy that addresses medical, non-medical and indirect costs. Implementing targeted support programmes and ensuring medication affordability are key steps towards mitigating the economic susceptibility of leprosy patients and facilitating successful treatment outcomes. Furthermore, the development of more effective strategies for active surveillance and early detection of leprosy is crucial in reducing the burden of the disease.
Supplemental Material
sj-docx-1-smo-10.1177_20503121241281424 – Supplemental material for The economic burden of leprosy treatment to households in Ghana: A cross-sectional study in the Volta Region of Ghana
Supplemental material, sj-docx-1-smo-10.1177_20503121241281424 for The economic burden of leprosy treatment to households in Ghana: A cross-sectional study in the Volta Region of Ghana by Maxwell Ayindenaba Dalaba, Alfred Kwesi Manyeh, Mustapha Immurana, Martin Amogre Ayanore, Isaiah Agorinya, James Akazili, Patricia Akweongo and Benedict Okoe Quao in SAGE Open Medicine
Footnotes
Acknowledgements
The authors would like to express their sincere gratitude to the individuals who generously participated in this study and shared their experiences. Their contributions are essential to advancing our understanding of the economic burden of leprosy treatment in Ghana. We extend our thanks to the Ho Municipal Leprosy Control Department for providing us with the list of leprosy cases and for their support during the initial consenting process. Their collaboration was instrumental in facilitating participant recruitment. Finally, we appreciate the dedication and hard work of the data collectors who diligently gathered and recorded the data for this study. Their meticulous efforts have ensured the accuracy and integrity of our findings.
Authors’ contributions
MAD, AKM, MI and BOQ contributed to the conception, design, data collection, analysis, interpretation and drafting of the manuscript. MAA, IA, JA and PA contributed to the analysis, interpretation and drafting of the manuscript. All authors have read and agreed to the published version of the manuscript.
Availability of data and materials
Relevant data and materials based on which conclusions were made are included in the manuscript. However, the study data are available from the corresponding author upon reasonable request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by the Anesvad Foundation (GHA-3639/22).
Ethics approval and consent to participate
Ethical approval was sought from the Ghana Health Service-Ethics Review Committee (Approval number: GHS-ERC: 006/05/23). Also, written consent was obtained from all the respondents.
Ethical consideration
Ethical approval was sought from the Ghana Health Service-Ethics Review Committee (Approval number: GHS-ERC: 006/05/23). A two-step approach was employed to ensure that all respondents have fully consented to participate in the study voluntarily. In the first stage, the leprosy focal person within the Disease Control Department of MHD used the list of registered leprosy cases to approach them by phone to explain the nature of the study and objectives. Only those individuals who provided verbal consent were included in a list made available to the data collectors. In the second stage, data collectors contacted individuals on the consented list and personally re-explained the study to them, and then written consent was obtained again from all respondents before proceeding with the interview. For the respondents who could not speak the English language (illiterates), the consenting was done in the local language (Ewe).
Informed consent
Only those individuals who provided verbal consent were included in a list made available to the data collectors. In the second stage, data collectors contacted individuals on the consented list and personally re-explained the study to them, and then written consent was obtained again from all respondents before proceeding with the interview. For the respondents who could not speak the English language (illiterates), the consenting was done in the local language (Ewe).
Consent for publication
Not applicable.
Trial registration
Not applicable.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.