
Abstract
Background:
This research study investigates the degree of medication-related satisfaction experienced by Palestinian patients with diabetes. In addition, this study further assesses the association between certain clinical and socio-demographic factors and the degree of satisfaction among the patients.
Methods:
This cross-sectional, descriptive study design consisted of 415 randomly selected patients from the Palestine Medical Complex (PMC), the Palestinian Ministry of Health Clinics, and from the Palestinian Diabetes Institute (also known as: Al-Bireh Medical Center). The Diabetes Medication Satisfaction (DiabMedSat) questionnaire measured patients’ satisfaction levels regarding their medications.
Results:
Odds ratios from binomial logistic analysis and the analysis of variance determined statistically significant correlations. The analysis has displayed the presence of significant associations between clinical and socio-demographic factors and treatment satisfaction. Significance was determined at p values < 0.05 and p values < 0.01.
Conclusion:
This research identified statistically significant associations between certain clinical and socio-demographic factors and diabetic patients’ satisfaction regarding their treatment. Addressing the concerns and difficulties experienced by the patients may impede treatment incompliance and hinder the development of complications, or at least postpone them.
Keywords
Introduction
It is known that diabetes mellitus (DM) is increasing dramatically in both developed and developing countries. According to the World Health Organization, the prevalence of diabetes worldwide has risen from 4.7% in 1980 to 8.5% in 2014. 1 Similarly, in Palestine, the prevalence of DM is increasing tremendously. This disease affected 9.7% of the population in the year 2000. Surprisingly, the figure rose to 15.3% in 2010. In 2013, Abu-Rmeileh and colleagues conducted studies predicting that the prevalence of DM would increase to 20.8% of the general population in 2020 and 23.4% of the general population in 2030. 2 In any of its forms, DM is a major concern among Palestinians given the fact that 5.7% of all deaths are due to diabetes and its complications (macrovascular and microvascular). 3
Uncontrolled DM can lead to serious complications, thus, increasing the need for additional care. Glycemic control plays a major role in preventing the development of complications. 2 Many individuals with diabetes develop complications due to their lack of medication adherence. Several factors exist that may correlate to treatment incompliance. Medications may be too expensive, cause uncomfortable or unbearable side effects, or even be inaccessible, causing an unstable glucose level in the bloodstream. 4 In this case, complications are inevitable. Thus, diabetic patient satisfaction regarding DM drugs is vital, for it determines the occurrence of complications and thus, the expense of providing care.
The purpose of our research was to determine the level of medication satisfaction among Palestinians with diabetes. In addition, the second aim of our study was to determine the effect of certain factors on the level of patient satisfaction. These factors include sex, age, marital status, occupational status, educational level, monthly salary, type of diabetes, HbA1C level, and type of medication.
Methods
Study design
A cross-sectional, descriptive study design was used to conduct this study.
Ethical consideration
The study was approved by the Palestinian Ministry of Health (No: MoH/162/581/2017) and the Helsinki Palestinian Ethical Committee (No: PHRC/HC/279/17). Written informed consent was obtained from all individual participants included in the study before taking part in the research. Finally, the participants were informed that they had the right to refuse to participate or withdraw at any time.
Study setting, sample, and sampling
The sample consisted of 415 patients from the Palestine Medical Complex (PMC), The Palestinian Ministry of Health Clinics, and from the Palestinian Diabetes Institute (also known as: Al-Bireh Medical Center). Initially, a minimum sample size of 196 from each sex was determined based on the following formula:

where, n is sample size, Z is the value from standard normal distribution (set to 1.96 for a 95% confidence level), P is the prevalence rate (an estimate of 0.15 was used), and C is the margin of error (set to 0.05).
A total of 415 patients (205 males and 210 females) were included in this study which ran from June 2017 to June 2018. The participants were selected against eligibility criteria. The following must have been met in order for the individual to be considered: age ⩾ 18 years, male or female, DM type I or II, and mentally competent and alert. The recruitment process involved visiting clinics and encountering the patients. Patients who fitted our eligibility criteria were asked to participate in the study. The participants who agreed to take part in our study signed a consent form after thoroughly understanding the research. Thereafter, a questionnaire was delivered to the participants in the Arabic language to assure full understanding. A user agreement was signed with the MAPI Research Institute (Lyon, France) prior to using the Arabic questionnaire. The Diabetes Medication Satisfaction (DiabMedSat) questionnaire assessed the degree of satisfaction towards medication usage. It consisted of 21 items that fell under three subscales: burden (11 items), symptoms (5 items), and efficacy (5 items). The 21 items preceded an overall satisfaction question. This questionnaire, developed from community clinic focus groups, was pretested in patients suffering from diabetes. It assessed treatment experiences including ease and convenience, lifestyle burdens, wellbeing, and medical control. An association treatment complexity (p value < 0.05) supported the construct validity of this tool. An additional tool, ‘Difficulties Faced by the Diabetic Patients Questionnaire’ was also used. 5
Statistical analysis
The data were coded and analyzed using the Statistical Package for Social Sciences (SPSS) software, version 21.0. Outcome variables measured on a binomial response scale (1 = yes, 0 = no) were subject to binomial logistic regression. Meanwhile, outcome variables measured on a multinomial ordinal response scale (0 = never or not at all to 4 = all the time or extremely) were subjected to multinomial ordinal regression analysis with the logit used as a link function. The odds ratio was obtained for each level of the independent variables with the last category taken as the reference. The odds ratio for each category was interpreted as the probability the category had higher score value of the response variable compared with the reference category (which had an odds ratio of 1.0). Outcome variables measured on the 7-point Likert scale (1 = extremely dissatisfied to 7 = extremely satisfied) were analyzed using univariate analysis of variance in the general linear model procedure with all independent factors fitted simultaneously in the model. Tukey’s test was used for multiple pairwise comparisons and differences were considered significant when the p value was <0.05.
Results
The participants of this study were characterized by certain socio-demographic and epidemiological factors. Table 1 displays the distribution of the studied diabetic patients according to these factors. A total of 73% of the research group was suffering from DM type II versus 27% who were diagnosed with type I DM. In addition, 72% of the patients had a glycated hemoglobin (HBA1C) level above 7%. The majority (40.7%) had insulin as the form of treatment. Some were taking medications in the form of tablets (27.5%), and yet, others were taking both tablets and insulin (31.8%). Slightly over half of the participants were female (50.6%). The age group ranged from 20 years to 90 years with the largest portion ranging between 50 and 59 years old (29.4%). A large portion of the research group were married (71.1%) with others being single (13.7%), divorced (4.6%), or widowed (10.6%). Unemployment was experienced by a large portion of our participants (52.8%). On the other hand, a very small percentage were students (2.9%). Some were civil workers (16.6%) while 27.7% were in the private sector or self-employed. The educational level varied among the patients: illiterate (15.7%), elementary school level (24.3%), preparatory school level (15.2%), high school level (16.9%), college level (17.8%), and graduate school level (10.1%). The economic status was also assessed based on the monthly salary: <US$300 (38.3%), US$300–600 (24.1%), >US$600 (37.6%).
Distribution of studied diabetic patients by socio-demographic and epidemiologic factors.

HbA1c, glycated hemoglobin.
In Table 2, we present the odds ratios from logistic binomial analysis of clinical conditions and socio-demographic factors in relation to the factors of burden measured via the questionnaire (difficulties experienced by patients with diabetes); odds ratios with higher values indicate a higher probability of difficulty. There was a statistically significant correlation between type of diabetes and difficulty in changing physical habits (p < 0.05) and difficulty in using a blood glucose meter (p < 0.01). The HbA1C level was significantly associated with difficulty in changing dietary habits (p < 0.01), difficulty in changing physical habits (p < 0.05), difficulty in taking medications (p < 0.05), difficulty in owning a blood glucose meter (p < 0.01), and difficulty in using a blood glucose meter (p < 0.01). The type of medication used (pills, insulin, or both) displayed a significant correlation (p < 0.01) with difficulty in changing physical habits. Sex showed a significant association (p < 0.01) with difficulty in attending follow-up visits and difficulty in regularly self-monitoring blood glucose levels. Age was significantly correlated (p < 0.05) with difficulty in changing dietary habits and difficulty in changing physical habits. There was a significant relation (p < 0.05) between occupation and difficulty in changing dietary habits and difficulty in using a blood glucose meter. The educational level of the participants was significantly associated with difficulty in changing dietary habits (p < 0.01) and difficulty in taking medications (p < 0.05).
Odds ratios from binomial logistic regression analysis of clinical conditions and socio-demographic factors in relation to difficulties faced by the diabetic patients.

HbA1c, glycated hemoglobin; ns, not significant (p > 0.05); **p < 0.05; ***p < 0.01.
The clinical conditions and socio-demographic factors in relation to the factors of the questionnaire measuring the effect of medications on daily life are presented in Table 3. The type of diabetes had a significant association (p < 0.05) with the medications interfering in the flexibility of planning daily meals. Age showed a significant correlation (p < 0.01) with the medications interfering in the ability to follow a recommended diet. In addition, the educational level of the patients was statistically related (p < 0.01) to the interference of medications in the flexibility to plan daily meals.
Odds ratios from multinomial logistic regression analysis of clinical conditions and socio-demographic factors in relation to the effects of medications on the daily activities of the diabetes patients.
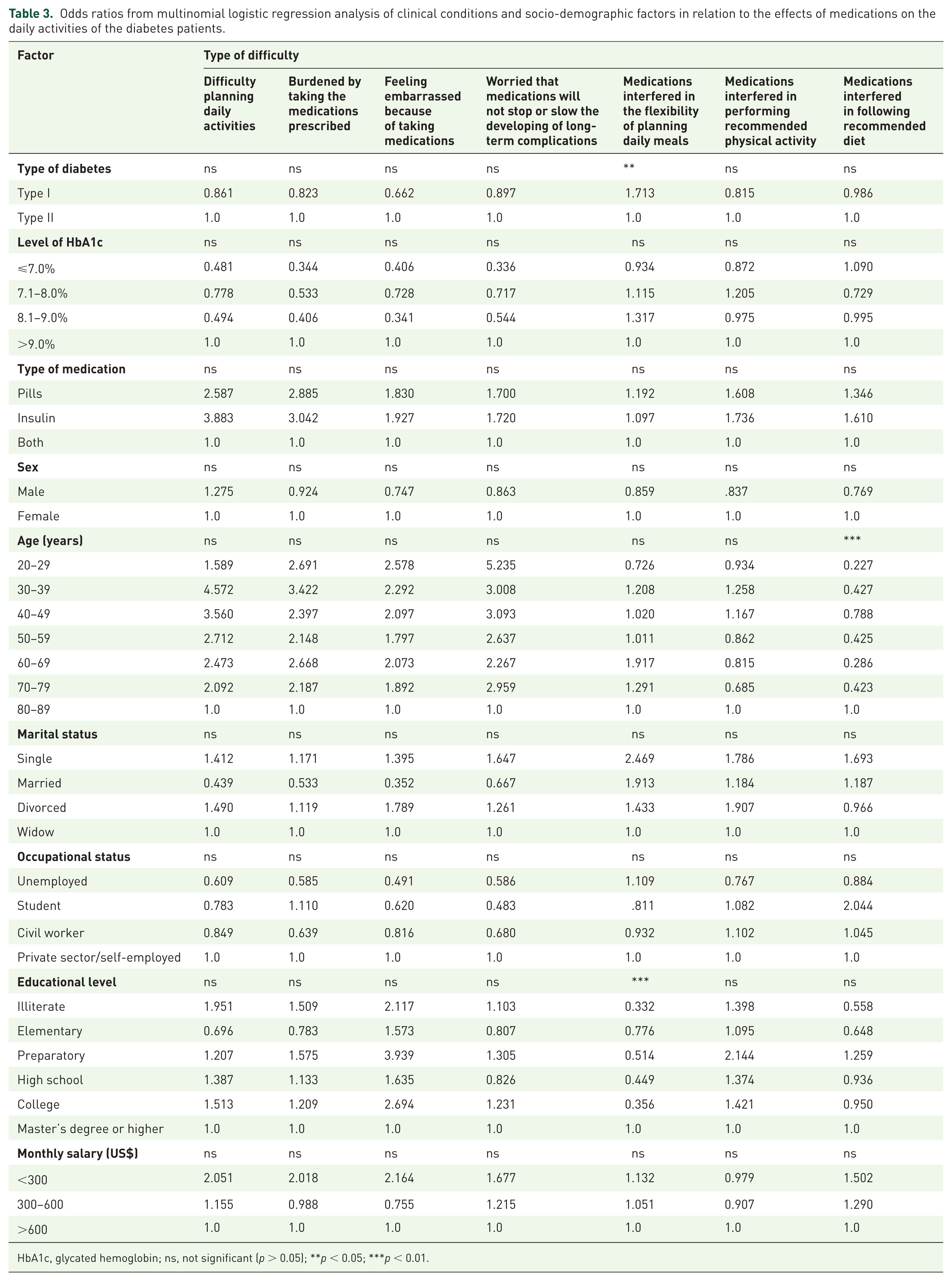
HbA1c, glycated hemoglobin; ns, not significant (p > 0.05); **p < 0.05; ***p < 0.01.
An analysis of variance was used to determine the effect of clinical and socio-demographic factors on the degree of satisfaction among the diabetic patients of this study. The results are presented as mean values in Table 4. A larger mean value indicates a higher satisfaction. The level of HbA1C showed a statistically significant effect on the degree of satisfaction regarding the ability of DM treatment to keep blood sugar stable (p < 0.05), the degree of satisfaction regarding the ability of DM treatment to prevent the feeling of tiredness (p < 0.01), the degree of satisfaction regarding the effects of DM medications on physical wellbeing (p < 0.05), and the overall degree of satisfaction regarding DM medications (p < 0.01). The type of DM medication was a significant factor (p < 0.05) in determining the degree of satisfaction regarding the ability of DM treatment to keep blood sugar stable, the degree of satisfaction regarding the easiness and convenience of DM medications, and the degree of satisfaction regarding the effect of the medications on emotional wellbeing. Age was significantly related (p < 0.05) to the overall interest in changing the type of medication or the route of medication administration. The educational level of the participants showed a significant association with the degree of satisfaction regarding the ability of DM treatment to keep blood sugar stable (p < 0.01), the degree of satisfaction regarding the ability of DM treatment to prevent the feeling of tiredness (p < 0.01), the degree of satisfaction regarding the easiness and convenience of DM medications (p < 0.05), and the overall interest in changing the type of medication or the route of medication administration (p < 0.01).
Effects of clinical conditions and socio-demographic factors on the degree of satisfaction of the diabetic patients: analysis of variance.

HbA1c, glycated hemoglobin; ns, not significant (p > 0.05); **p < 0.05; ***p < 0.01.
Means of the levels of the same factor that have different superscripts are significantly different (p < 0.05) using Tukey’s test for multiple comparisons.
Table 5 displays the prevalence of diabetic complications among studied patients. The prevalence of these complications, demonstrated by a percentage, is presented as a total of the whole group and separately for type I DM and type II DM. Retinopathy was experienced by 19.8% of the entire group, 25.9% of patients with type I DM, and 17.5% of patients with type II DM. Nephropathy made up 19.6% of patients with type I DM, 15.5% of patients with type II DM, and 16.6 % of the whole group. Neuropathy covered 18.3% of the participants, 17.0% of patients with type I DM, and 18.8% of patients with type II DM.
Prevalence of diabetic complications suffered by the participants with diabetes.

Discussion
A number of clinical and socio-demographic factors displayed a significant association with the degree of satisfaction of diabetic patients regarding their medications. As observed from our results, many of the medication-induced difficulties experienced by the patients have a significant relationship with one or more of the clinical and socio-demographic factors tested.
The HbA1C level of patients with diabetes is linked to the development of stress. Hilliard and colleagues report that higher stress leads to poorer glycemic control, as seen in our study. Diabetic patients have to live with a life-long disease that requires management and control. This may cause the patients to feel overwhelmed and they may find it difficult to adhere to changes in their lives such as modifying their diet. 6 In addition, similar to our study, Yang and colleagues concluded that the older the patient is, the greater the amount of knowledge obtained throughout the previous years regarding the disease and its relation to life. Patients with a better understanding of the components of a balanced meal may find it easier to adhere to a healthy diet. 7 Moreover, civil workers showed the greatest amount of difficulty in changing dietary habits in this sector. Poulsen and colleagues suggest that working can cause an individual to feel tired, which in turn makes it difficult to follow a healthy, balanced diet. 8 Finally, the educational level of the patients is critical for adherence to to a modified diet plan. Our results show that illiterate people had the most difficulty in changing their diet. In Yang and colleagues’ study, the same association was concluded. Patients who understand their condition and dietary requirements are more likely to adherence to an appropriate diet. 7
Patients with type I diabetes, as indicated by our results, experienced a higher degree of difficulty related to increasing physical activity. According to a position statement by the American Diabetes Association, both type I and type II diabetes benefit from regular physical activity, for it improves glycemic control and decreases insulin resistance. 9 In addition, patients with type II diabetes usually require diet and exercise as a major component of the treatment plan as opposed to patients with type I diabetes who have insulin as their main treatment factor. This could be the reason behind patients with type II diabetes experiencing more difficulty in becoming more active. Second, previous studies have concluded that an increase in physical activity lowers the HbA1C level 10 , 11 . Thus, a high HbA1C would determine the need for an increase in physical activity. Yang and colleagues support this rationale by concluding that a lack of knowledge regarding the HbA1C level and other disease-related information may lead to treatment incompliance. 7
Our results show that people with diabetes with an HbA1C level between 7.1% and 8.0% experienced the greatest difficulty. Might not yet be fully adjusted to their situation, making them less likely to be compliant with their treatment regime. Futher more, lack of knowledge about new medications may also lead to treatment incompliance. 7 This supports our observed cause-effect relationship between educational level and the difficulty in taking medications. The majority of our participants displayed illiteracy or a low educational level.
Males show a greater difficulty than women. Cameron and colleagues have conducted a study discussing the differences between males and females regarding health and healthcare uses. Contrary to our results, their study suggested that females had less visits with the healthcare provider than men with similar socio-demographic and health characteristics. 12 This may be explained by the fact that the majority of the male population in Palestine have long-hour jobs and find it difficult to attend follow-up visits due to a tight schedule or constantly being overwhelmed with the job.
Our study suggests that patients with diabetes with HbA1C levels between 7.1% and 8.0 % have the greatest difficulty. Moreover, a study conducted by Tenderich supports our findings in that it provides descriptive reasons for the cause of difficulty experienced by patients with type II diabetes in using blood glucose meter. These reasons include the device being expensive, the burden of carrying it around, the painful prick, and forgetting to test, among others. 13 Students were shown to experience the most difficulty in using a blood glucose meter for monitoring their glucose levels. One study carried out by Wagner and colleagues showed that many students face problems in monitoring their blood glucose levels at school due to other students or the environment itself. 14 Finally, our results indicate that men have more difficulty in self-monitoring than women. However, Hawthorne and Tomlinson concluded that women experience difficulty due to a lack in knowledge of its use. 15
Patients with type I diabetes, according to our results, have greater difficulty with medications regarding its interference with planning meals. This may be due to the interference of insulin administration before or after meals and the need to adjust meals with insulin administration. In addition, García-Pérez and colleagues suggested that a major contributing factor to the lack of diabetic patient adherence to treatment may be a result of a missing support system. 16 Age played a role in affecting the degree of difficulty regarding medications interference in following a recommended diet. 17 Beverly and colleagues performed a study showing that the middle-aged and older-aged patients with diabetes benefit from support systems in adhering to a treatment regimen. 18
HbA1C levels equal to or less than 7% showed the least satisfaction. This could be due to patients being newly diagnosed and not yet fully adjusted to the addition of new medications in their life. 19 In addition, the less educated the person, the more difficult it is to understand the benefits of the medications. 6 Third, the highest level of satisfaction was seen with the patients taking pills compared with those taking insulin. Patients may not have adequate knowledge about insulin and its mechanism of action; instead, they are familiar with pills and believe that they are the main curative agent for any type of disease.
As expected, those who are taking pills find it easier to take medications than those who are taking insulin. Many patients with diabetes in our study were between 50 and 59 years of age. This age group may find it more difficult to see and adjust an insulin syringe. We also observe that illiterate individuals found it more difficult to take the medications. Patients who do not understand how to take their medications correctly may have decreased satisfaction. 6 Patients with low HbA1C have the least degree of satisfaction. This may be because patients are still adjusting to their new diagnosis. Insulin is known to have effects on blood glucose levels and may cause hypoglycemia, causing patients to feel the patients to feel tired and weak. 19
The prevalence of diabetic complications in our sample is displayed in Table 5. The majority of diabetic individuals exhibited retinopathy. Diabetic retinopathy is the most common complication, affecting patients of working age. 20 The majority of our participants were between 50 and 59 years. The second largest group was between 40 and 49 years. Thus, this explains the largest percentage of diabetic complications being retinopathy (19.8%).
Contribution to literature
Few research studies have been performed in Palestinian patients with diabetes. This research study enables healthcare professionals to better understand patients’ thoughts and feelings regarding their medications. The specific factors that contribute to a lower degree of satisfaction, now, may be taken into consideration. As this study points out, a lower satisfaction level leads to treatment incompliance which then leads to disease complications. If the healthcare team can improve satisfaction level by reviewing certain factors, treatment incompliance may decrease, reducing complications and cost of care.
Limitations
The majority of our patients were had type II DM. The number exceeds the number of type I DM by three times. Our research was not focused on one type of DM; thus, this only affects the results of the correlations associated with the type of diabetes and does not affect our study as a whole. Second, other factors, such as depression and anxiety, were not accounted for. These parameters may have contributed to the degree of satisfaction and may have affected our results. Another limitation is self-reporting. The participants self-reported their satisfaction or dissatisfaction. There are no means to validate their results. Some participants may not have clearly expressed their thoughts, while others may have exaggerated.
Conclusion
Many Palestinians with diabetes are having difficulties with treatment adherence and are developing complications associated with the disease due to medication incompliance. This research identified statistically significant associations between certain clinical and socio-demographic factors and the satisfaction of patients with diabetes regarding their treatment. Addressing their concerns and difficulties may help reduce this incompliance and decrease the development of complications, or at least postpone them.
Footnotes
Acknowledgements
S.B. and S.H. contributed to the design, implementation of the research, and wrote the main manuscript text. A.J. prepared the analysis of the results and Tables 1–5. B.A. and N.E. contributed to the design, implementation of the research and acquisition of data. All contributors reviewed the manuscript.
The Palestinian Ministry of Health, as well as the Helsinki Palestinian Ethical Committee, gave approval for this research study (approval number: PHRC/HC/279/17).
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The authors declare that there is no conflict of interest.