
Abstract
Meglitinides such as repaglinide and nateglinide are useful to treat type 2 diabetes patients who follow a flexible lifestyle. They are short-acting insulin secretagogues and are associated with less risk of hypoglycemia, weight gain and chronic hyperinsulinemia compared with sulfonylureas. Meglitinides are the substrates of cytochrome P450 (CYP) enzymes and organic anion transporting polypeptide 1B1 (OATP1B1 transporter) and the coadministration of the drugs affecting them will result in pharmacokinetic drug interactions. This article focuses on the drug interactions of meglitinides involving CYP enzymes and OATP1B1 transporter. To prevent the risk of hypoglycemic episodes, prescribers and pharmacists must be aware of the adverse drug interactions of meglitinides.
Introduction
Drug interaction is defined as the interference of effects of one drug by the coadministered drugs, nutrients (food), herbs, alcohol or tobacco smoke. 1 The drug interaction results in either increased or decreased beneficial effects or increased adverse effects. The drug interaction leading to undesirable effects, is termed ‘adverse drug interaction’. Polypharmacy, having liver or kidney disease, or a number of underlying chronic disorders elevate the risk of adverse drug interactions. 2
Interacting drugs can alter the pharmacokinetic or pharmacodynamic profile of another. Plasma concentration of one drug is either increased or decreased by altering absorption, distribution, metabolism, or excretion of another drug, and this type of interaction is known as pharmacokinetic drug interactions. The pharmacodynamic interactions are those in which the effect of one drug is altered by the presence of another drug at the same receptor or molecular site.3–5 Object drug is the one affected by the interaction, and the drug causing the interaction is termed precipitant drug. The absorption, distribution, metabolism, excretion, or actual clinical effect of the object drug is usually modified by the precipitant drug. 6
The risk of adverse drug interactions is higher in diabetes patients, as they coadminister the medications to manage their comorbidities such as dyslipidemia, hypertension, heart disease, depression, infections, etc., along with their antidiabetic medications. A Brazil study comprised 140 diabetes patients who attended a tertiary care outpatient center, indicated a prevalence of 75% of potential drug–drug interactions, of which 20.7% were major interactions. 7 And a study from Croatia identified that 80.9% of diabetes patients had at least one potential drug interaction requiring monitoring of therapy. 8 Most of the antidiabetic drug interactions may result in hypoglycemia-related complications. Severe hypoglycemia is a life-threatening emergency and can result in seizures, coma and death.9,10
Meglitinides are short-acting insulin secretagogues and they include repaglinide and nateglinide. Repaglinide is a benzoic acid derivative and nateglinide a
Pharmacokinetic drug interactions of meglitinides
Meglitinides are the substrates of cytochrome P450 (CYP) enzymes and organic anion transporting polypeptide 1B1 (OATP1B1 transporter). Repaglinide is metabolised by CYP2C8 and CYP3A4 enzymes17,18 while nateglinide is metabolized primarily by CYP2C9 enzyme and by CYP3A4 enzyme to a much lesser extent.19–21
Organic anion transporting polypeptides (OATPs) are membrane influx transporters and their family consists of 11 members including OATP1B1, OATP1B3 and OATP2B1. 22 OATPs are the members of solute-linked carriers (SLCO) superfamily and particularly SLCO21A family; they are ATP-independent polypeptides.23–25
OATP1B1 transporter found in sinusoidal membrane of hepatocytes aids liver uptake of their substrate drugs.26–28 The pharmacokinetics of repaglinide is majorly determined by OATP1B1 transporter. 29 Nateglinide is also a substrate of OATP1B1 transporter, which determines the hepatic uptake of nateglinide. 30
Drug interactions of repaglinide
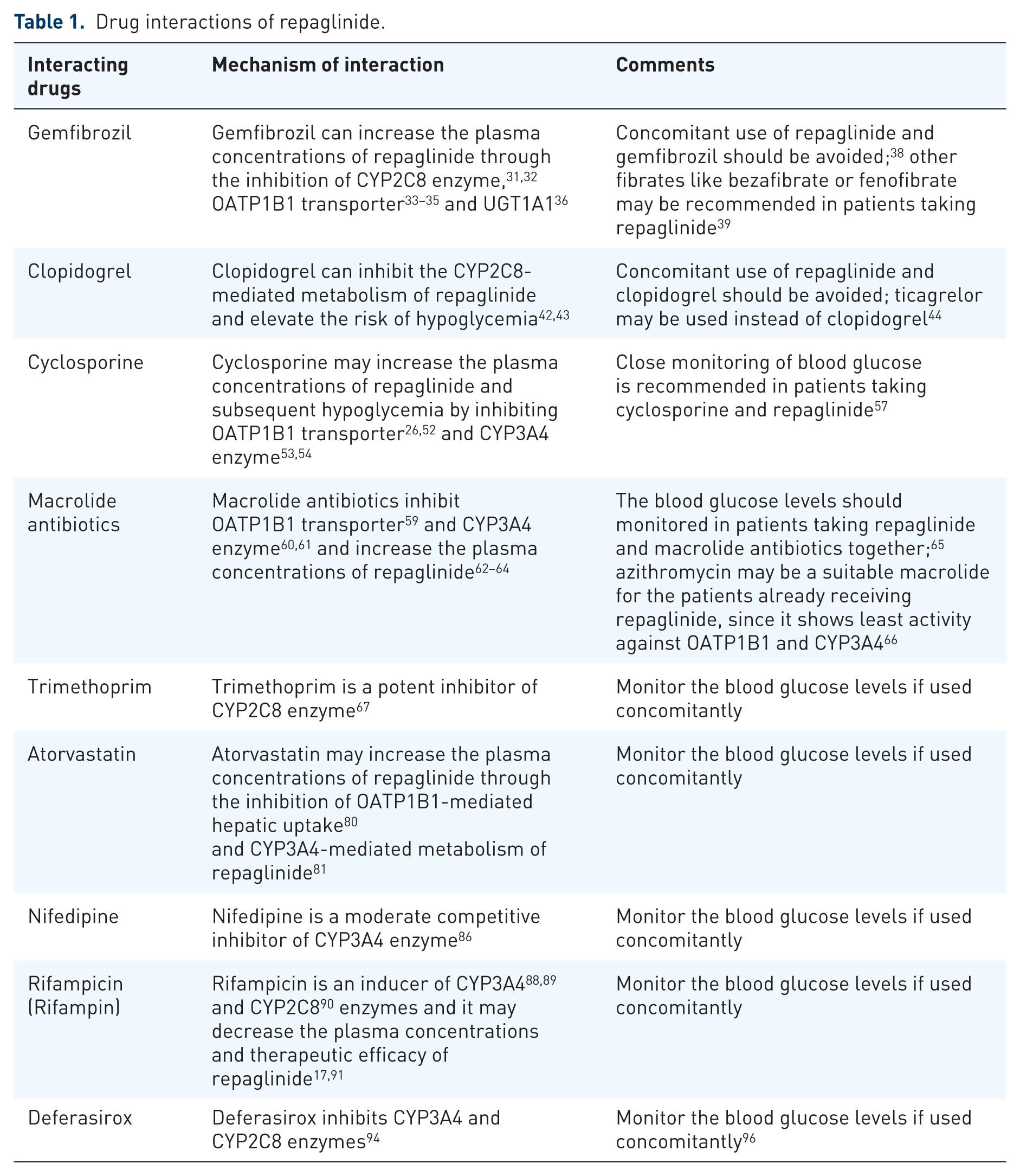
Drugs inducing or inhibiting CYP enzymes (CYP2C8 and CYP3A4) and OATP1B1 transporter do play an important role in the drug interactions of repaglinide (Figure 1 and Table 1).

Drug interactions of repaglinide.
Drug interactions of repaglinide.
Gemfibrozil
Gemfibrozil is an inhibitor of CYP2C8 enzyme.31,32 Gemfibrozil and its glucuronide metabolite also inhibit OATP1B1-transporter-mediated hepatic uptake of repaglinide.33–35 Since repaglinide is the substrate of both CYP2C8 enzyme and OATP1B1 transporter, its concomitant use with gemfibrozil resulted in increased plasma concentrations of repaglinide and subsequent hypoglycemia.36,37 Gemfibrozil is also found to inhibit Uridine Diphosphate (UDP) glucuronosyltransferase 1A1 (UGT1A1) involving in glucuronidation of repaglinide, resulting in additional elevation of plasma concentrations of repaglinide. 36
Hence, the patients on repaglinide should avoid using gemfibrozil. 38 Hypertriglyceridemia of the patients taking repaglinide could be treated with either bezafibrate or fenofibrate due to their lack of interaction with repaglinide. 39
Clopidogrel
Clopidogrel is a second-generation thienopyridine antiplatelet drug and is a P2Y12 receptor antagonist. 40 Nowadays, clopidogrel is prescribed most commonly as an antiplatelet drug. The American Diabetes Association (ADA) recommends using clopidogrel as a secondary prevention strategy in diabetes patients with a history of atherosclerotic cardiovascular disease and an intolerance to aspirin therapy. 41
Use of clopidogrel in diabetes patients taking repaglinide may result in elevated plasma concentrations of repaglinide, since glucuronide metabolite of clopidogrel is a strong CYP2C8 inhibitor.42,43
To avoid hypoglycemia, it is recommended that repaglinide is not coadministered with clopidogrel. Ticagrelor may be a suitable antiplatelet drug to treat diabetes patients taking repaglinide; or else, patients taking clopidogrel may be prescribed nateglinide rather than repaglinide. 44
Cyclosporine
Cyclosporine is an immunosuppressant medication that decreases the production of inflammatory cytokines by T lymphocytes through the blockade of calcineurin’s phosphatase activity by forming the cyclosporine–cyclophilin complex. 45
Cyclosporine is less diabetogenic and with less risk of developing post-transplant diabetes mellitus compared with tacrolimus and corticosteroids. 46 Hence, cyclosporine may be preferred over tacrolimus to treat diabetes patients needing organ transplantation.47,48 Cyclosporine is identified to reduce the risk of rheumatoid-arthritis-associated atherosclerosis 49 and hence it may be useful to treat the patients of rheumatoid arthritis with diabetes. Cyclosporine may also be used in treating the patients of systemic lupus erythematosus (SLE) with diabetes, since it decrease the risk of SLE-associated atherosclerosis. 50 In addition, cyclosporine may be a useful treatment option in patients with resistant Churg-Strauss syndrome (CSS). 51
Cyclosporine is shown to inhibit the OATP1B1 transporter-mediated hepatic uptake of substrates.26,52 Cyclosporine is also an inhibitor of the CYP3A4 enzyme.53,54 Hence, cyclosporine may elevate the exposure of repaglinide and the risk of hypoglycemia by inhibiting OATP1B1-transporter-mediated hepatic uptake and CYP3A4-enzyme-mediated metabolism of repaglinide.55,56 Close monitoring of blood glucose is recommended in patients taking cyclosporine and repaglinide. 57
Macrolide antibiotics
Macrolide antibiotics include erythromycin, clarithromycin and azithromycin. They are widely used to treat respiratory tract infections and skin and soft tissue infections, primarily. 58
OATP1B1-mediated hepatic uptake of substrates is inhibited by macrolide antibiotics such as erythromycin, roxithromycin and telithromycin in a concentration-dependent manner. 59 Macrolide antibiotics such as erythromycin, clarithromycin and roxithromycin can also inhibit intestinal and hepatic CYP3A4 enzyme.60,61 Concomitant use of repaglinide and clarithromycin or telithromycin resulted in increased plasma concentrations and blood-glucose-lowering effect of repaglinide, which may lead to hypoglycemic risk.62–64
The blood glucose levels should be monitored in patients taking repaglinide and macrolide antibiotics together. 65 Azithromycin may be a suitable macrolide for the patients already receiving repaglinide, since it shows least activity against OATP1B1 and CYP3A4. 66
Trimethoprim
Trimethoprim is a potent inhibitor of CYP2C8 enzyme at clinically relevant concentrations. 67 In healthy subjects, the plasma concentrations of repaglinide found elevated by trimethoprim are probably due to the inhibition of CYP2C8-mediated metabolism of repaglinide. 68 The risk of hypoglycemia may be higher in diabetic patients with renal dysfunction and taking repaglinide and trimethoprim concurrently. 69
Hydroxymethylglutaryl coenzyme A reductase inhibitors (statins)
Hydroxymethylglutaryl coenzyme A reductase inhibitors or statins are effective lipid-lowering drugs and they decrease the serum cholesterol by inhibiting hepatic cholesterol biosynthesis, resulting in upregulation of hepatic low-density lipoprotein (LDL) receptors and increased clearance of LDL-cholesterol (LDL-C). 70 In addition, statins can improve endothelial function and blood flow, enhance the stability of atherosclerotic plaques, decrease oxidative stress and inflammation, inhibit vascular smooth muscle proliferation and platelet aggregation, and reduce vascular inflammation as their cholesterol-independent or ‘pleiotropic’ effects.71–74
Statins are very much effective in secondary prevention of cardiovascular diseases (CVDs) and decrease the mortality in people with pre-existing CVD.75,76 Statins are also useful in the primary prevention of cardiovascular diseases (CVD) and reduce the risk of major cardiovascular events like myocardial infarction, stroke, etc. in people without established cardiovascular disease but with cardiovascular risk factors like diabetes, elevated blood pressure, obesity, etc.77–79
The plasma concentrations of repaglinide might be raised by atorvastatin through the inhibition of OATP1B1-mediated hepatic uptake. 80 Atorvastatin may also inhibit CYP3A4-mediated metabolism of repaglinide and increase its activity. 81 The bioavailability of oral repaglinide enhanced by fluvastatin might be due to the inhibition of CYP3A4-mediated metabolism of repaglinide. 82
Nifedipine
Nifedipine is a dihydropyridine calcium channel blocker and it is useful to treat older patients with systolic hypertension and diabetes.83,84 Nifedipine found to improve diabetes-associated cognitive impairment as a pleiotropic effect. 85
Nifedipine is a moderate competitive inhibitor of the CYP3A4 enzyme. 86 The oral bioavailability of repaglinide may be elevated by the coadministration of nifedipine which can inhibit CYP3A4-mediated metabolism of repaglinide. 87
Rifampicin (rifampin)
Rifampicin is an antitubercular drug and it is a potent inducer of the CYP3A4 enzyme.88,89 Rifampicin can also induce the expression of other CYP enzymes, including CYP2C8. 90 Since rifampicin induces both CYP3A4 and CYP2C8 enzymes, it may decrease the plasma concentrations and therapeutic efficacy of repaglinide.17,91
Deferasirox
Deferasirox is the most commonly used oral iron chelator and it is useful for the treatment of chronic iron overload resulting from long-term blood transfusions.92–94 The diabetic patients with β thalassemia may be prescribed deferasirox to treat iron overload. 95
Deferasirox is a weak inhibitor of both CYP3A4 and CYP2C8 enzymes, 96 which are involved in the metabolism of repaglinide. Concomitant use of deferasirox and repaglinide warrants careful monitoring of glucose levels. 97
Drug interactions of nateglinide
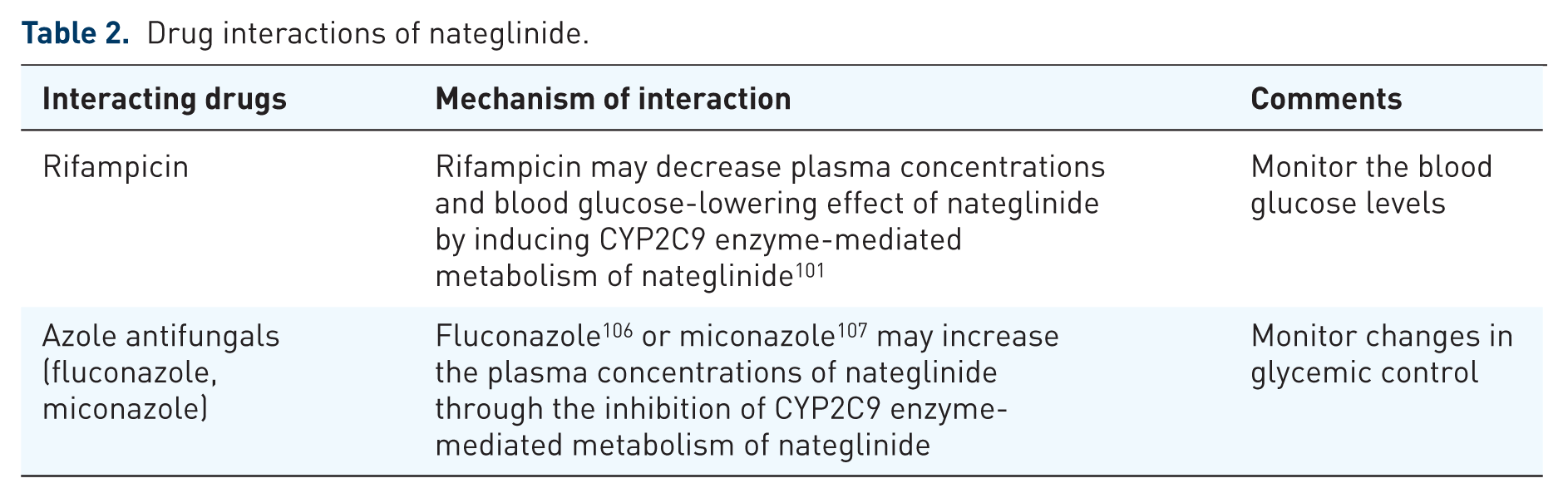
Drugs inhibiting or inducing CYP2C9 enzyme and OATP1B1 transporter do play an important role in the drug interactions of nateglinide (Figure 2 and Table 2).

Drug interactions of nateglinide.
Drug interactions of nateglinide.
Rifampicin
Rifampicin is primarily used in the treatment of tuberculosis. The diabetic patients with tuberculosis would be prescribed with rifampicin along with other anti-TB drugs.98–100
Rifampicin may induce CYP2C9 enzyme-mediated oxidative biotransformation of nateglinide resulting in decreased plasma concentrations and blood-glucose-lowering effect of nateglinide. Monitor the blood glucose levels while the initiation and discontinuation of rifampicin in patients taking nateglinide. 101
Azole antifungals
The rate of fungal infections is higher in patients with diabetes.102–104 Fluoconazole is an azole antifungal drug and is recommended in diabetic patients to treat fungal infections, as it is found effective against cutaneous Candidiasis, oropharyngeal Candidiasis (OPC) and vulvovaginal Candidiasis (VVC). 105
The plasma concentrations of nateglinide might be enhanced by the coadministration of fluconazole, which can inhibit the CYP2C9 enzyme-mediated metabolism of nateglinide. 106 CYP2C9 enzyme-mediated metabolism of nateglinide might also be inhibited by miconazole. 107 It is advisable to monitor changes in glycemic control during their concomitant use.
Conclusion
Repaglinide and nateglinide are the substrates of CYP enzymes and OATP1B1 transporter. Repaglinide is metabolized by CYP2C8 and CYP3A4 enzymes and OATP1B1 transporter determines its hepatic uptake. The patients taking repaglinide should avoid using drugs such as gemfibrozil and clopidogrel due to heightened risk of hypoglycemia. Drugs like cyclosporine, macrolide antibiotics, trimethoprim, statins and nifedipine elevate the risk of hypoglycemia in patients taking repaglinide, so blood glucose levels of such patients should be monitored. Concomitant use of repaglinide or nateglinide and rifampicin may result in reduced blood-glucose-lowering effects. To prevent the adverse drug interactions of meglinide antidiabetics, the prescribers and pharmacists must be aware of these effects.