
Abstract
Objectives
To compare the efficacy, safety and compliance of repaglinide, administered either two or three times daily, regarding glycaemic control in patients with type 2 diabetes mellitus.
Methods
Japanese adults with type 2 diabetes mellitus, who had been treated without sulphonylureas or glinides for >3 months, were randomly assigned to two groups to receive either 0.25 mg repaglinide, oral, twice daily (group A) or 0.25 mg repaglinide, oral, three times daily (group B). Glycosylated haemoglobin (HbA1c), glycoalbumin (GA) and 1,5-anhydroglucitol (1,5-AG) levels were measured at 0, 1, 2 and 3 months after treatment commenced.
Results
Out of 43 patients who enrolled (group A, n = 22; group B, n = 21), 33 patients completed the trial (group A, n = 16; group B, n = 17). No significant between-group differences in HbA1c, GA, or 1,5-AG levels were seen at 1–3 months. No severe hypoglycaemic episodes or other adverse events were observed.
Conclusions
Minimal-dose repaglinide administered twice daily was similar in efficacy and safety to three-times-daily administration, in Japanese patients with type 2 diabetes mellitus. Administration of repaglinide twice daily could be an alternative regimen for patients who cannot take repaglinide three times daily.
Introduction
Epidemiological research has demonstrated that postprandial hyperglycaemia is necessary to reduce the risk of cardiovascular complications, in patients with diabetes mellitus.1,2 One such study in Japan demonstrated that the incidence of cardiovascular complications was significantly higher for patients with diabetes and persons with impaired glucose tolerance, compared with subjects with normal glucose tolerance, but no significant difference was observed between patients with impaired fasting glucose and those with normal fasting glucose. 2 One of the characteristics of Japanese patients with type 2 diabetes mellitus is a decline in insulin secretion from an early disease stage. 3 Glinides are oral hypoglycaemic agents that improve impaired insulin secretion following meals, in patients with type 2 diabetes mellitus.4–6 Repaglinide is available clinically in Japan and has the potential to play an important role in the treatment of Japanese patients with type 2 diabetes. Patients are instructed to take repaglinide before meals (two, three or even four times daily, preprandially) in the USA. 7 Repaglinide must be taken just before a meal three times daily when administered according to the standard therapy regimen in Japan. Like α-glucosidase inhibitors (α-GIs), however, the need to take this drug just before meals and the three-times-daily dosing schedule are associated with poor adherence. 8 Poor compliance with medication instructions is common among patients with diabetes and is associated with adverse clinical outcomes. 9
Poor compliance with glinide therapy may be due, in part, to the need to take the medication immediately before meals, and the three-times-daily standard dosing schedule. The present research group previously evaluated ways of improving drug adherence in patients receiving α-GIs and found that administering α-GIs following meals improved compliance.10–12 Furthermore, administration of miglitol at breakfast was found to increase plasma active glucagon-like peptide-1 levels, and improve plasma glucose levels following lunch, even if miglitol was not taken at lunchtime.13,14 The present researchers also reported that twice-daily administration of acarbose improved glycaemic control in patients with type 2 diabetes mellitus. 15 These studies demonstrated the efficacy, in terms of glycaemic control, of administering α-GIs twice daily.
Administration of repaglinide/metformin in a fixed-dose combination twice daily has been reported as being similar to three-times-daily administration, in terms of glycaemic control. 16 Thus, the theory behind the present study was that administration of repaglinide two times daily might enable similar glycaemic control to that of three-times-daily administration in Japanese patients with type 2 diabetes mellitus, and might also improve treatment compliance. In the present study, the efficacy and safety of two- or three-times-daily administration of a minimum fixed dose of 0.25 mg repaglinide was compared in Japanese patients with type 2 diabetes mellitus.
Patients and methods
Study population
Japanese adults with type 2 diabetes mellitus, treated with dietary therapy alone or fixed-dose oral hypoglycaemic agents (with the exception of sulphonylureas and glinides) for over 3 months at Yokohama City University Hospital, Yokohama, Japan and Nakajima Naika Clinic, Yokosuka, Japan between August 2011 and September 2012, were enrolled.
Primary endpoints were changes in glycosylated haemoglobin (HbA1c), glycoalbumin (GA) and 1,5-anhydroglucitol (1,5-AG) levels; secondary endpoints were changes in body mass index (BMI), drug adherence, and adverse events (particularly the frequency and degree of hypoglycaemia). HbA1c (%) values were expressed in accordance with the National Glycohemoglobin Standardization Program (NGSP). Patients with liver dysfunction (including liver cirrhosis or malignancy) and patients with severe diabetic complications (active proliferative diabetic retinopathy, or severe diabetic nephropathy) were excluded from the study. If a doctor (H.K., K.A., S.N., K.S., K.K. and Y.T.) considered a patient to be at risk of hypoglycaemia, or if the patient refused to provide informed consent, the patient’s participation in the study was terminated and the patient was treated with other appropriate drugs as soon as possible. Patients who experienced hypoglycaemic symptoms were instructed to take glucose, to stop taking repaglinide, and to call or visit the hospital as soon as possible. Doses of oral hypoglycaemic drugs, including repaglinide, were not changed throughout the study.
Since the primary outcome of this study was change in glycaemic control in the two groups, patients who could not take the study drug two or three times daily for 3 months were excluded from analysis.
This study was approved by the Institutional Ethics Review Committee of Yokohama City University, and written informed consent was obtained from all participants. The trial was registered with the UMIN (University Hospital Medical Information Network) Clinical Trials Registry (UMIN000006855).
Study design
Patients were randomized to two groups using the envelope method: group A was assigned to take 0.25 mg repaglinide, oral, twice daily; group B was assigned to take 0.25 mg repaglinide, oral, three times daily. Patients in both groups were instructed to take repaglinide just before meals. Baseline characteristics, including age, sex, duration of diabetes, BMI, and HbA1c, GA, and 1,5-AG levels were recorded immediately prior to initiating repaglinide therapy.
Blood samples were collected at 0, 1, 2, and 3 months following initiation of repaglinide treatment. Blood samples were obtained from the antecubital vein into fluoride tubes containing sodium citrate and ethylenediaminetetra-acetic acid or heparin for the analysis of plasma glucose and HbA1c, and into plain siliconized tubes for the analysis of 1,5-AG and GA. Following collection, samples for analysis of 1,5-AG and GA levels were allowed to stand for ∼5 min at room temperature, then centrifuged at 4℃, 2330
Adherence to the dosing regimen was assessed using a questionnaire survey. Each patient was asked to complete a written questionnaire in the presence of medical doctors at 1, 2, and 3 months following initiation of repaglinide therapy. Adherence was scored for each patient, at each timepoint, as follows: 1, 0–49%; 2, 50%–69%; 3, 70%–89%; 4, 90–100%.
Statistical analyses
Data were presented as mean ± SD and were analysed using Statistical Analysis System (SAS®) software, version 9.2 (SAS Institute Inc., Cary, NC, USA). Between-group differences in age, BMI and duration of diabetes at baseline were estimated using unpaired Student’s t-test. Between-group differences in sex were estimated using χ2-test. Between- and within-group changes in HbA1c, GA, 1,5-AG and BMI levels in patients who completed the trial were analysed using a linear mixed model. A random intercept was used for each patient including time, group and these interactions as covariates, followed by the Bonferroni correction. 1,5-AG levels <1 µg/ml were expressed as 0.9 µg/ml for statistical calculations. Analysis of drug adherence was performed using Mann–Whitney U-test. A P-value <0.05 was considered statistically significant.
Results
A total of 43 Japanese adults with type 2 diabetes were randomized to two groups: 22 into group A, 0.25 mg repaglinide, oral, twice daily; 21 into group B, 0.25 mg repaglinide, oral, three times daily (Figure 1). In group A, 13 patients had been treated with dietary therapy alone (drug-naïve), three patients had been treated with metformin alone, four patients had been treated with a dipeptidyl peptidase (DPP)-4 inhibitor alone, one patient had been treated with metformin, α-GI and pioglitazone, and one patient had been treated with metformin and a DPP-4 inhibitor. In group B, 15 patients had been treated with dietary therapy alone (drug-naïve), three patients had been treated with metformin alone, one patient had been treated with a DPP-4 inhibitor alone, one patient had been treated with metformin and a DPP-4 inhibitor, and one patient had been treated with α-GI and a DPP-4 inhibitor.
Flow chart of Japanese adults with type 2 diabetes mellitus included in the present study. Of 43 patients who initially enrolled, 33 patients completed the trial (group A, 0.25 mg repaglinide, oral, twice-daily, n = 16; group B, 0.25 mg repaglinide, oral, three times daily, n = 17). Six patients in group A and four patients in group B were excluded from the final analyses.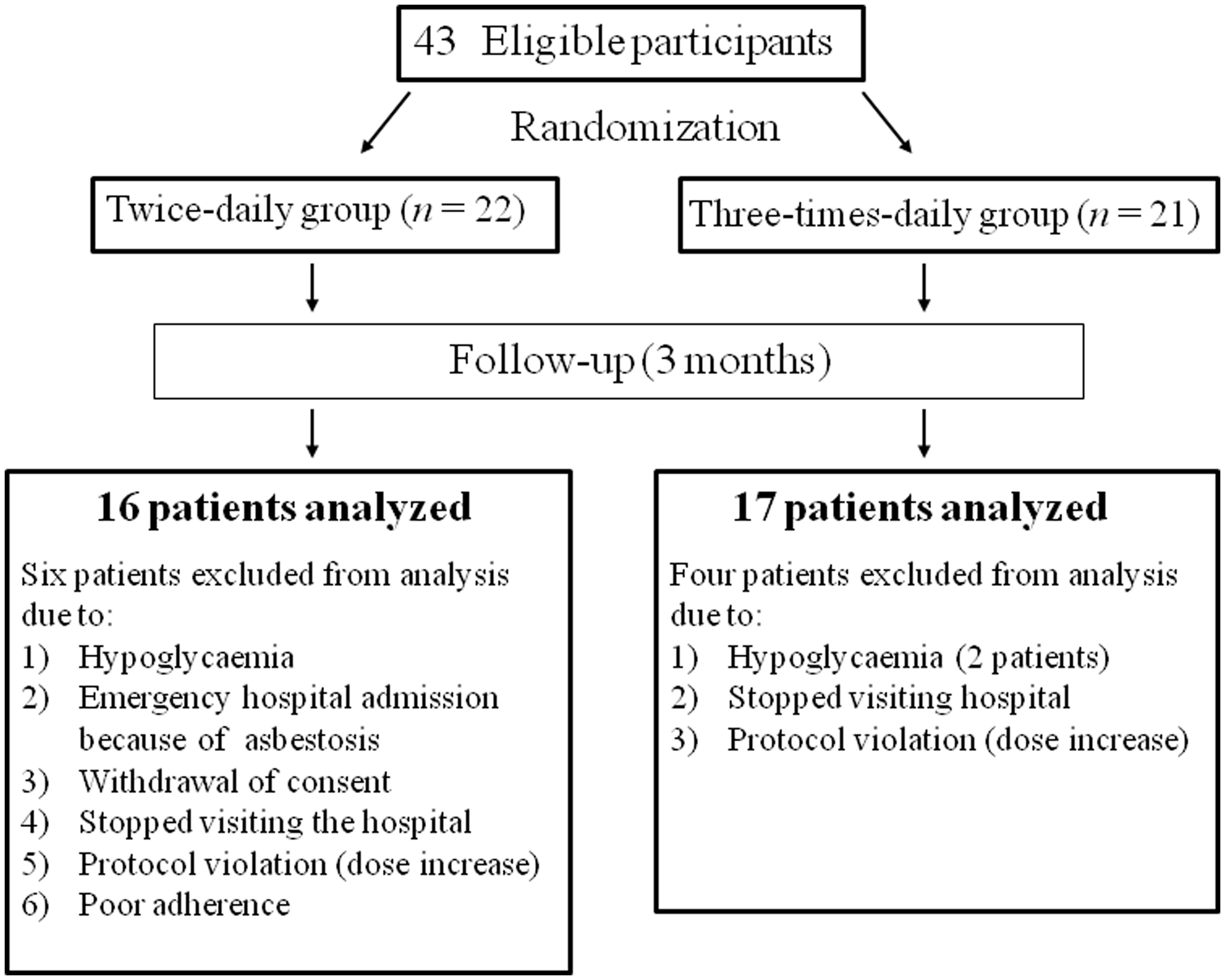
The following patients were excluded from the final analyses: group A (n = 6), change in treatment from repaglinide to a DPP-4 inhibitor due to hypoglycaemia (n = 1), emergency hospital admission due to asbestosis (n = 1), withdrawal of consent (n = 1), failure to visit the hospital (n = 1), increase in dosage causing a protocol violation (n = 1) and poor adherence (<50% at >2 months following the start of treatment) (n = 1); group B (n = 4), stopping repaglinide to avoid hypoglycaemia (physician’s judgement; n = 1), reducing metformin dosage to avoid hypoglycaemia (physician’s judgement; n = 1, failure to visit the hospital (n = 1) and an increase in dosage causing a protocol violation (n = 1; Figure 1).
Baseline characteristics of Japanese adults with type 2 diabetes mellitus assigned to receive: 0.25 mg repaglinide, oral, twice-daily (group A); or 0.25 mg repaglinide, oral, three times daily (group B).

Data presented as n patients or mean ± SD.
Values calculated for all patients entered at the start of the study.
No statistically significant between-group differences were observed (P ≥ 0.05; unpaired Student’s t-test for between-group differences in age, body mass index and duration of diabetes; χ2-test for between-group differences in sex).
Drug-adherence ratios in Japanese adults with type 2 diabetes mellitus, assigned to receive: 0.25 mg repaglinide, oral, twice-daily (group A), n = 16; or 0.25 mg repaglinide, oral, three times daily, n = 17 (group B) and who completed the trial.
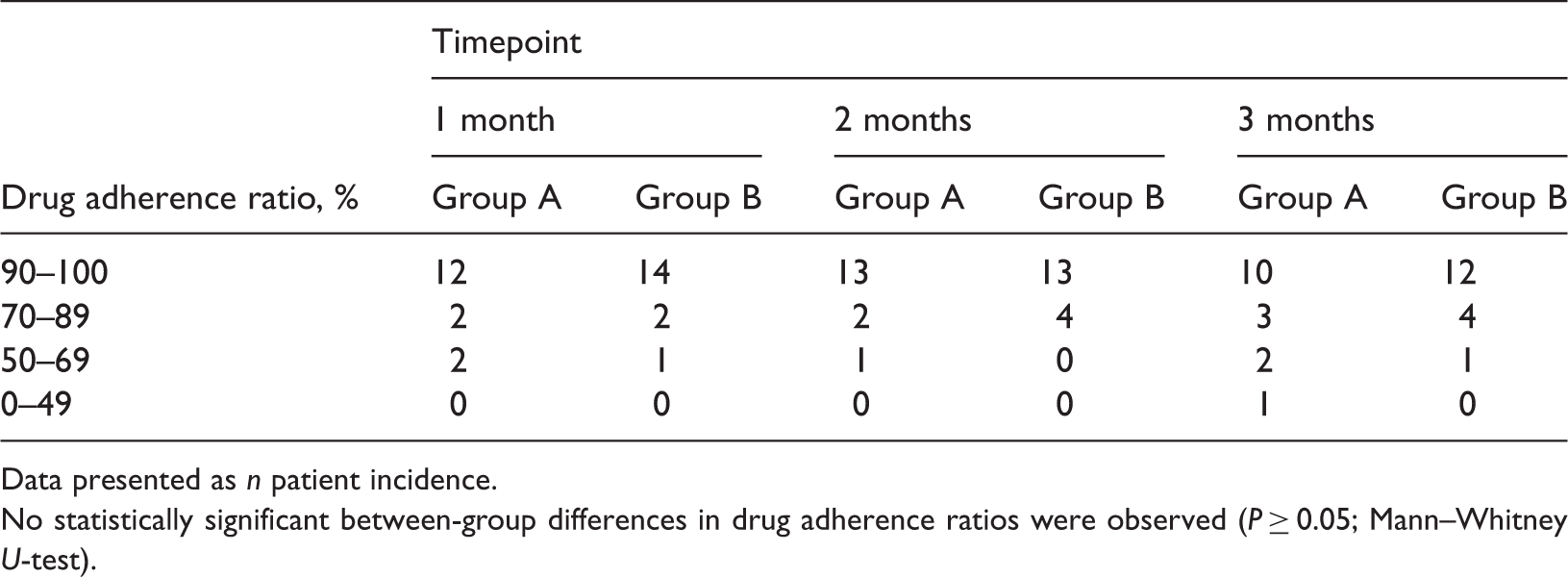
Data presented as n patient incidence.
No statistically significant between-group differences in drug adherence ratios were observed (P ≥ 0.05; Mann–Whitney U-test).
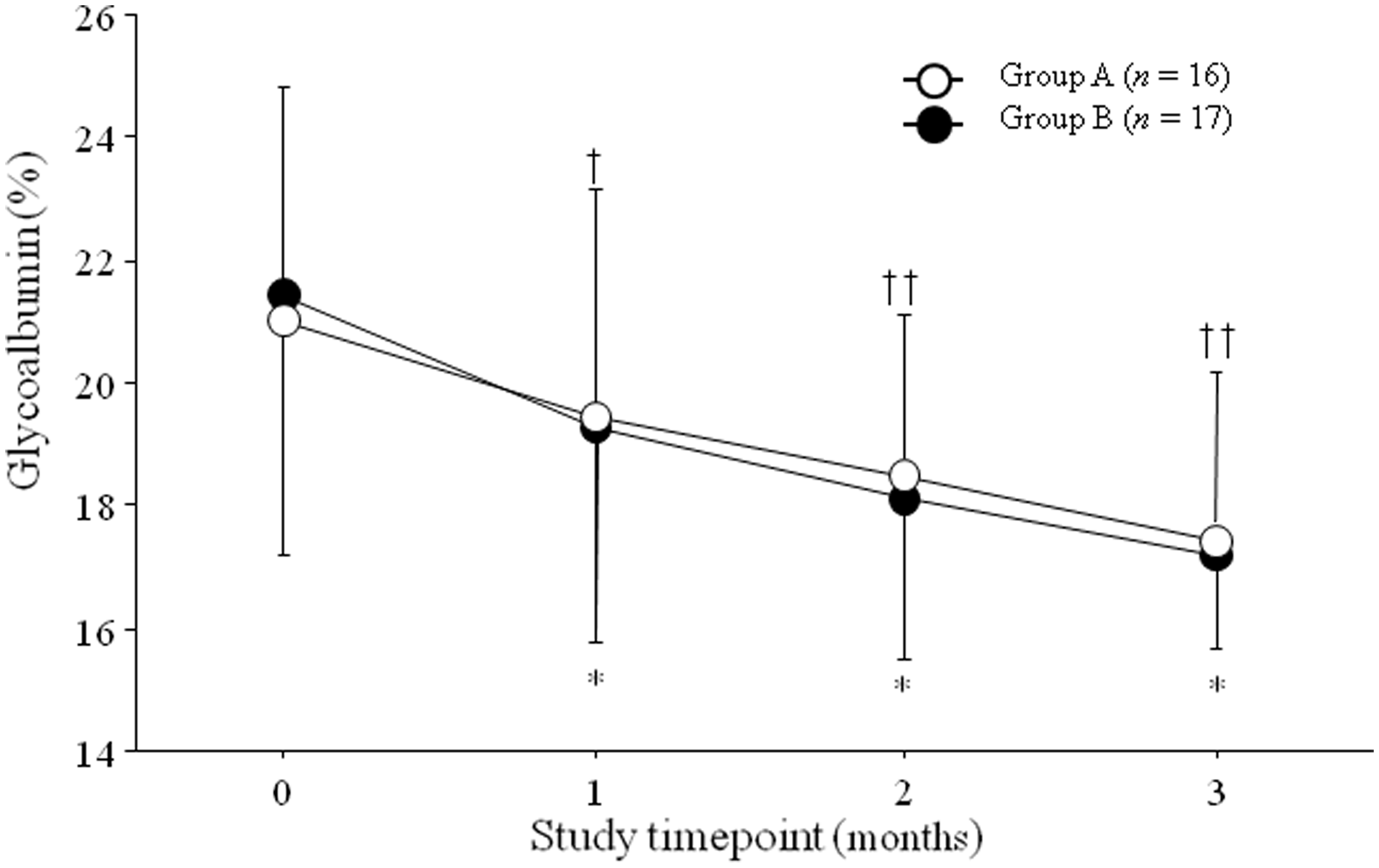
In groups A and B, mean HbA1c and GA levels had decreased significantly at 1, 2, and 3 months compared with baseline levels. No statistically significant differences in the HbA1c or GA levels were observed between the two groups at any timepoint (Figure 2 and Figure 3, HbA1c and GA, respectively).
Mean glycosylated haemoglobin values in Japanese adults with type 2 diabetes mellitus assigned to receive 0.25 mg repaglinide, oral, twice-daily (group A), n = 16; or 0.25 mg repaglinide, oral, three times daily (group B), n = 17. Data are presented as mean ± SD for both groups at baseline and at 1, 2, and 3 months following the start of treatment. No statistically significant between-group differences were observed at any timepoint (P ≥ 0.05; linear mixed model). †P < 0.01, ††P < 0.05 versus baseline value in group A; *P < 0.05, **P < 0.001 versus baseline value in group B; linear mixed model. Mean glycoalbumin values in Japanese adults with type 2 diabetes mellitus assigned to receive: 0.25 mg repaglinide, oral, twice-daily (group A), n = 16; or 0.25 mg repaglinide, oral, three times daily, n = 17 (group B). Data presented as mean ± SD for both groups at baseline and at 1, 2, and 3 months following the start of treatment. No statistically significant between-group differences were observed at any timepoint (P ≥ 0.05; linear mixed model). †P < 0.01, ††P < 0.05 versus baseline value in group A; *P < 0.001 versus baseline value in group B; linear mixed model.
In group A, the mean 1,5-AG level appeared to increase slightly by 3 months compared with baseline values, but the difference was not statistically significant (P = 0.0825). In group B, the mean 1,5-AG level had increased significantly at 3 months (P < 0.05). No significant differences in the 1,5-AG levels were observed between the two groups at any timepoint (Figure 4).
Mean 1,5-anhydroglucitol values in Japanese adults with type 2 diabetes mellitus assigned to receive: 0.25 mg repaglinide, oral, twice-daily (group A), n = 16; or 0.25 mg repaglinide, oral, three times daily (group B), n = 17. Data presented as mean ± SD for both groups at baseline and at 1, 2, and 3 months following the start of treatment. No statistically significant between-group differences were observed at any timepoint (P ≥ 0.05; linear mixed model). *P < 0.05 versus baseline value in group B; linear mixed model.
Three incidences of hypoglycaemia and subsequent use of antidiabetic drugs other than repaglinide, resulted in patients being excluded from the study. During the present study, no severe hypoglycaemic episodes occurred in either group. No other adverse events were observed in either group. No statistically significant differences in BMI were observed between the two groups at any timepoint during the 3-month period compared with baseline values (Figure 5).
Mean body mass index values in Japanese adults with type 2 diabetes mellitus assigned to receive: 0.25 mg repaglinide, oral, twice-daily (group A), n = 16; or 0.25 mg repaglinide, oral, three times daily (group B), n = 17. Data presented as mean ± SD for both groups at baseline and at 1, 2, and 3 months following the start of treatment. No statistically significant between-group differences were observed at any timepoint and there was no change in mean values during the 3-month period (P ≥ 0.05; linear mixed model).
Discussion
The present study investigated Japanese adults with type 2 diabetes mellitus, treated with 0.25 mg oral repaglinide either two or three times daily. The most important finding in the present study was that HbA1c, GA, and 1,5-AG levels did not differ significantly between the two groups at 1, 2, or 3 months following initiation of treatment with repaglinide. Glinide therapy inhibits postprandial hyperglycaemia by increasing insulin secretion following meals. 17 Thus, strict intake immediately before meals three times daily is considered to be necessary to obtain a sufficient improvement in blood glucose levels. Guidance for patients regarding the mechanism of action and the importance of regular drug intake is considered to be important; however, good compliance can still be difficult to obtain, particularly among the elderly and patients with busy social lives. Medication nonadherence is prevalent among patients with diabetes and is associated with adverse clinical outcomes. 9 The present study investigated the improvement in blood glucose control in patients with type 2 diabetes who were treated with repaglinide twice or three times daily for 3 months. There was no difference in degrees of improvement in HbA1c, GA, and 1,5-AG levels between the two groups at 1, 2, and 3 months. These results concur with published data obtained using a fixed-dose combination of repaglinide/metformin, taken two or three times daily.16,18
Repaglinide has a longer availability than other glinides, 16 therefore, one of the theories behind the present study was that administration of repaglinide twice daily might not be inferior to administration of repaglinide three times daily. One study, involving various community-pharmacy-supplied drugs, reported significantly improved mean adherence of 79.1% ± 19% for once-daily dosing regimens, compared with 65.6% ± 30% for twice-daily regimens, and 38.1% ± 36% for three-times-daily regimens. 19 The results of the present study, showing no significant between-group differences in glycaemic control, suggest that starting treatment with a twice-daily regimen, rather than a three-times-daily regimen, may be useful for patients with poor compliance.
In the present study, HbA1c levels decreased by ∼0.7% following treatment with repaglinide (0.25 mg two or three times daily) for three months. To the best of the authors’ knowledge, the dosage effect of 0.25 mg of repaglinide per meal on glycaemic control has not been previously reported. In the USA, the initial starting dosage of repaglinide for patients with diabetes who have not been previously treated, or whose HbA1c level is < 8%, is 0.5 mg/meal, while the initial starting dosage for patients whose HbA1c level is > 8% is 1 or 2 mg/meal. The maximal daily dosage is 16 mg/day. 7 In the present study, the efficacy of the smallest dosage of repaglinide (0.25 mg, twice daily) was comparable with that used for European and North American patients with type 2 diabetes. Several reasons for this difference in dosage can be considered. First, patients’ BMIs in the present study were lower than those of European and North American patients, and the insulin resistance of the Japanese patients was assumed to be lower than that of the European and North American patients. Secondly, Japanese patients have a lower capacity for insulin secretion than European and North American patients.20,21 The main aetiology of Japanese patients with type 2 diabetes mellitus is thought to be low insulin secretion, rather than high insulin resistance.20,21 Sitagliptin (a DPP-4 inhibitor) has been reported to be more effective than pioglitazone (a synthetic ligand for peroxisome proliferator-activated receptors) in the treatment of Japanese patients with type 2 diabetes mellitus. 22 Even the smallest dosage of repaglinide, therefore, is considered to be effective for Japanese patients, whose insulin secretion is low. Administration of 0.5 mg repaglinide for 4 months has been reported to be efficacious in Japanese patients with type 2 diabetes mellitus. 23 In a study performed mainly in Caucasians, treatment with repaglinide (0.5–1.0 mg/meal) for 4 months significantly improved glycaemic control compared with baseline values and placebo, reducing the mean HbA1c level by 1.1%. 24 Following the present study, the authors plan to evaluate the efficacy and safety of repaglinide administered two or three times daily at doses > 0.25 mg. In the present study, repaglinide therapy was as effective as results reported for glimepiride or glibenclamide therapy,25–27 therefore, we also hope to evaluate the effectiveness of a two- or three-times-daily repaglinide regimen after switching from sulphonylurea treatment.
In the present study, patients were instructed to take 0.25 mg repaglinide two- or three-times daily, and no significant between-group difference in drug adherence was observed. A questionnaire to survey the total amount of medication taken in this study was not conducted. An assumption was made that administration of repaglinide twice daily could improve drug adherence in daily clinical practice because the number of administrations was decreased. Based on the results of the present study, starting a twice-daily treatment, rather than a three-times-daily treatment, may be beneficial for patients with poor compliance.
The present study had several limitations. The number of patients included was relatively small and the term of the study was short, therefore, large-scale and long-term studies may elucidate a more representative effect on glycaemic control of repaglinide two or three times daily on the population of Japanese patients with diabetes.
In conclusion, twice-daily administration of a minimal dose of repaglinide (0.25 mg) had similar efficacy and safety profiles to three-times-daily administration, in Japanese patients with type 2 diabetes mellitus. Thus, administration of repaglinide twice daily may be useful as a substitute regimen in patients who are unlikely to adhere to a three-times-daily regimen.
Footnotes
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Funding
This work was supported in part by Grants-in-Aid for Scientific Research (B) 19390251, (B) 21390282, and (B) 24390235 from the Ministry of Education, Culture, Sports, Science and Technology (MEXT) of Japan, and a Medical Award from the Japan Medical Association.
Acknowledgements
The authors thank the following nurses and medical clerks: M. Toyoda, I. Mutou, M. Funaoka,Y. Tokunaga, K. Murata, Y. Kotachi, K. Kanda, Y. Hamamoto, and M. Suzuki.