
Abstract

A 27-year-old gentleman with history of substance abuse was sent to the emergency department (ED) after he was found unresponsive outside his apartment by bystanders. Paramedics administered naloxone in the field without improvement and they reported that there was a bag of white powdered substance in his pocket. On arrival to the ED he had a Glasgow Coma Scale of 3/15. His rectal temperature was 28.5°C (83.4°F), blood pressure was 103/75 mm Hg, pulse was 88/min and respiratory rate was 14/min. Laboratory workup was significant for an arterial pH of 7.07 (normal 7.35–7.45), PCO2 of 63.2 mm Hg (normal 35–45 mm Hg), PO2 of 56.2 mm Hg, HCO3 of 18.3 mmol/l (normal 22–28 mmol/l) on 100% fraction of inspired oxygen, a serum lactic acid of 9.1 mmol/l (normal 0.5–1.9 mmol/l), white blood cell count of 23,200 cmm (normal 4800–10,800 cmm), blood urea nitrogen 26 mg/dl (normal 8–20 mg/dl), creatinine 2.43 mg/dl (normal 0.7–1.2 mg/dl), sodium 142 meq/l (normal 135–145 meq/l), potassium 4.9 meq/l (normal 3.3–5.3 meq/l), calcium 9.4 mg/dl (normal 8.6–10.3 mg/dl), magnesium 3 mg/dl (normal 1.8–2.5 mg/dl) and troponin <0.02 ng/ml (normal 0.02–0.03 ng/ml). Urine drug screen was positive for benzodiazepine, opiate, amphetamine and tetrahydrocannabinoid. Chest X-ray showed left lower lobe pneumonia and computed tomography scan of the brain showed no intracranial bleed. Upon arrival to the ED, the trachea was intubated and the patient was mechanically ventilated. Electrocardiogram (ECG) showed atrial fibrillation with rapid ventricular response (rate 107/min), widening of the QRS duration to 164 ms, and Osborn waves with highest amplitude recorded in precordial leads V4–V6 (8 mm amplitude) without any shivering artifacts (Figure 1). For comparison, Figure 2 is an ECG performed a year earlier, after the patient presented to the ED for palpitation. The patient made a successful recovery. Verbal informed consent was obtained from the patient for publication of this case.

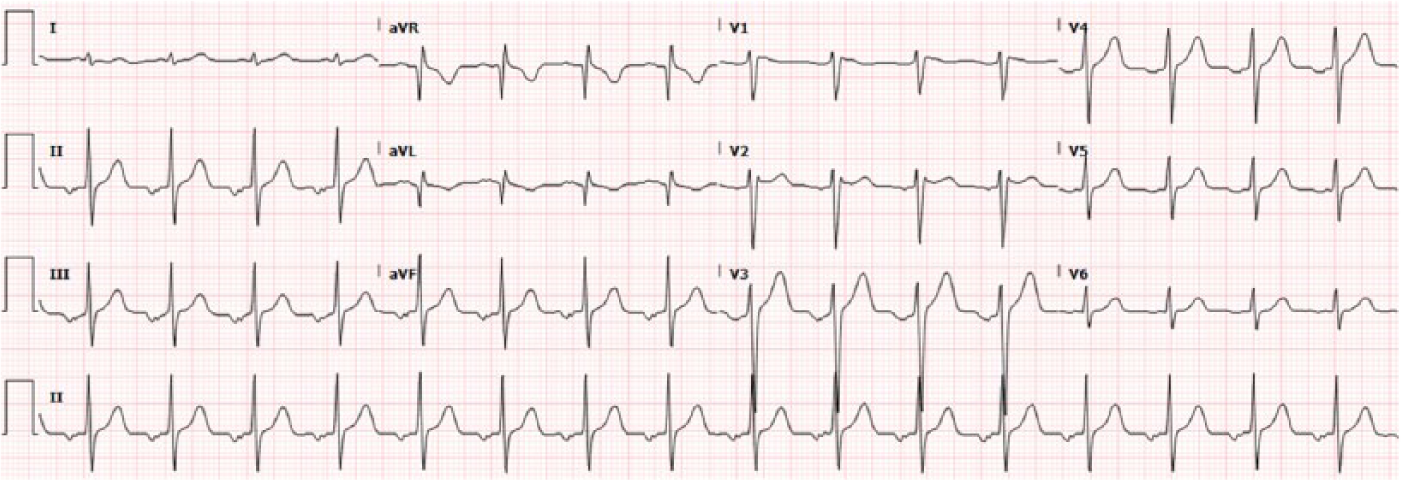
Electrocardiogram (ECG) of hypothermic patient on arrival to emergency department (ED) showing atrial fibrillation and high-amplitude Osborn waves (black arrows). The highest amplitude of Osborn waves was 8 mm in lateral leads. Note the absence of shivering artifacts despite the degree of hypothermia (temperature 28.5°C).
Baseline electrocardiogram (ECG) 1 year earlier showing low atrial rhythm.
Primary hypothermia also known as ‘accidental hypothermia’ is due to environmental exposure, and secondary hypothermia results from other medical illnesses unrelated to cold exposure. The Center for Disease Control and Prevention reported a total of 16,911 deaths in the USA due to excessive cold exposure with an average of 1301 per year from 1999 to 2011 and approximately 67% of these hypothermia-related deaths among males [Centers for Disease Control and Prevention, 2013]. Hypothermia is divided into degrees of severity according to the core body temperature as follows: mild (temperature 32–35°C), moderate (28–32°C) and severe (<28°C). Another classification of hypothermia is the Swiss staging system which grades hypothermia based on the presenting symptoms and this is preferred when it is not possible to determine an accurate core temperature. This is defined as stage 1 (awake and shivering), stage 2 (drowsy and nonshivering) and stage 3 (unconscious and nonshivering) [Brown et al. 2012]. Our case is graded as stage 3 hypothermia (unconscious and nonshivering).
Shivering artifacts are usually evident in the early stages of hypothermia and disappear as hypothermia becomes severe, and its presence has been considered as a good prognostic sign. Shivering artifacts were found to occur in 56% of hypothermic patients [Graham et al. 2001]. Prior studies showed that a higher proportion of survivors had shivering artifacts in their ECG (66% versus 38% of survivors and nonsurvivors, respectively, p = 0.047) suggesting that the inability to mount a shivering response is associated with poor outcome [Graham et al. 2001]. Therefore, one should be concerned when faced with an ECG of our case due to the presence of high-amplitude Osborn waves without shivering artifacts, in an unconscious patient. Other causes for absence of shivering artifacts is a hypothermic patient receiving moderate to deep sedation (if he is on mechanical ventilation for example): the sedation in this case will abolish the central nervous system (CNS) response to hypothermia and one would not see any artifacts. Also, shivering artifacts will not be seen in the head trauma victim who develops brainstem death with subsequent hypothermia due to impaired thermoregulatory ability from hypothalamic dysfunction [Omar et al. 2011]. We have previously reported cases of brain-death-induced hypothermia that were not on any sedation and had Osborn waves without shivering artifacts in the surface ECG [Omar et al. 2011; Omar and Abdelmalak, 2011].
The cause of hypothermia in our case is probably a combination of polysubstance abuse as well as accidental hypothermia. Despite the degree of hypothermia (28.5°C), there were no evident shivering artifacts and this is likely related to the severity of hypothermia, moreover, 20 min prior to the performance of ECG, the patient had received 80 mg of etomidate and 100 mg of the nondepolarizing neuromuscular blocker rocuronium in preparation for intubation. Looking at the ECG (figure 1) should raise suspicion for moderate to severe hypothermia due to the presence of high-amplitude Osborn waves, Osborn waves being evident in most EKG leads and not just the inferolateral leads and the prolongation of the QRS interval [Omar, 2016; Omar et al. 2016]. We have previously found that amplitude of the Osborn wave had a moderate significant inverse correlation (r = −0.410, p < 0.001) in predicting core body temperature in an analysis of all published cases with hypothermic Osborn waves [Omar and Camporesi, 2015]. These ECG signs are important especially during initial assessment of a patient in the field where the diagnosis of hypothermia can be missed by paramedics with the commonly used oral or tympanic thermometers since standard oral thermometers record temperature only as low as 35°C accurately. In addition, paramedics also rarely use thermometers in evaluating patients in the prehospital setting and therefore awareness of ECG features of hypothermia is important. Detecting hypothermia in the field will allow for early management and gradual rewarming. As evident, cardiologists are less likely to encounter the Osborn waves, which are usually diagnosed by other caregivers who should be familiar with ECG signs of hypothermia [Omar et al. 2012].
Another implication for Osborn waves is its arrhythmogenic potential [Omar, 2013]. However, unlike ischemic conditions [Omar, 2014], in hypothermic states, the correlation between the Osborn wave and ventricular fibrillation (VF) has not been well established. The initial report by John Osborn demonstrated that the Osborn wave is a bad prognostic sign in hypothermic dogs that triggered VF [Osborn, 1953]. A few years later, Fleming and Muir confirmed this arrhythmogenic potential in hypothermic patients [Fleming and Muir, 1957]. In their case series comprising 29 patients exposed to hypothermia for cardiac surgery, 21 patients developed VF [Fleming and Muir, 1957]. Nonetheless, other reports could not establish this same association [Emslie-Smith et al. 1959]. Previous reports have shown that the incidence VF or ventricular tachycardia is unexpectedly low in hypothermic patients with Osborn waves ranging from 0% to 2% [Rankin and Rae, 1984; Delaney et al. 2006; Vassal et al. 2001]. Whether the Osborn wave is a precursor for malignant ventricular arrhythmia needs further research.
Hypothermia affects all body organs but consequences on the cardiovascular system are most serious. There are several effects of hypothermia on the endocrine system. The endocrine organs react to immediate hypothermia by increasing metabolism and thermogenesis with the release of cortisol, thyroid hormones, catecholamines and glucagon. This results in an increase in blood glucose and free fatty acids and inhibition of insulin production and peripheral insulin responsiveness causing initial hyperglycemia [Curry and Curry, 1970] which was evident in our case who had an admission random blood sugar of 243 g/dl. However, with prolonged and severe hypothermia (<28°C) the endocrine organs stop working. Shivering consumes glucose, which, in addition to impaired gluconeogenesis with prolonged hypothermia, causes hypoglycemia [Mallet, 2002]. Since blood glucose level is not solely dependent on insulin production and gluconeogenesis, but also on the metabolic rate of the patient, the extent of shivering is an important determinant of how fast the glucose will be consumed. If hypothermia develops rapidly, it will lead to sympatho-adrenal activation which will raise the plasma norepinephrine level, but with prolonged hypothermia, catecholamines, cortisol and thyroid hormones often remain unchanged.
Footnotes
Acknowledgements
A verbal informed consent has been acquired from the patient for publication of this report.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The authors declare that there is no conflict of interest.