
Abstract
Thyroid storm is a rare life-threatening emergency due to thyrotoxicosis. A 30-year-old female presented with restlessness, tachycardia and vomiting but with normothermia which is an unusual presentation. There is the need for clinicians to be aware of atypical clinical features that can make the diagnosis of thyroid storm difficult.
Introduction
Thyroid storm, also known as thyroid or thyrotoxic crisis, is a rare life-threatening hypermetabolic emergency due to thyrotoxicosis [Tietgens and Leinung, 1995]. It usually occurs in previously undiagnosed patients who have major stress or in poorly treated hyperthyroid patients. The precipitants can be infection, withdrawal of antithyroid drugs, radioiodine therapy, medical illness, trauma, surgical procedure, and severe emotional stress [Sarlis and Gourgiotis, 2003]. It is mostly seen in patients with Graves’ disease and can be the first presentation. It occurs in about 1–2% of hyperthyroid patients with a high mortality rate of between 20% and 75% despite treatment [Bhattacharyya and Wiles, 1997; Burch and Wartofsky, 1993].
Case report
A 30-year-old female presented to the accident and emergency department with a day-long history of vomiting and restlessness. She had about five episodes of vomiting without diarrhea or constipation. There was associated palpitation. She was diagnosed to have Graves’ disease 7 months prior to presentation and was placed on carbimazole and propranolol. She was however noncompliant with medication and follow up. She stopped taking her antithyroid drugs 3 months prior to presentation. There was no family history of thyroid diseases.
On examination, she was found to be restless, afebrile with bilateral fine tremors. The pulse rate was 132 bpm and the blood pressure was 130/80 mmHg. There was lid lag, exophthalmos, and goiter with a bruit. The neurological examination was essentially normal except for the restlessness. Her thyroid function test revealed suppressed thyroid stimulating hormone (TSH) <0.01 mIU/ml (0.39–6.16), elevated Triiodothyronine (T3) 5.6 ng/ml (0.52–1.85) and elevated Thyroxine (T4) 26.06 μg/dl (4.8–11.6). Based on Burch and Wartofsky’s scoring system she had a total score of 50 which was highly suggestive of thyroid storm. A diagnosis of thyroid storm precipitated by noncompliance with medications was made. She was placed on carbimazole, propranolol and intravenous hydrocortisone with remarkable improvement within 2 days of medications. She was discharged 10 days after presentation with a pulse rate of 86 bpm, blood pressure of 120/80 mmHg and a temperature of 36.0oC. She was also counseled on the need for compliance to drugs and clinic follow up.
Discussion
Thyrotoxic storm is a rare medical emergency caused by an exacerbation of the hyperthyroid state that can be fatal unless recognized and treated early. The clinical presentations are due to a hypermetabolic state, as well as to the increase in sympathetic nervous system activity that occurs [Wilson and Hobbs, 1993; Landsberg, 1977].
Thyroid storm is usually characterized by fever, tachycardia/arrhythmias, gastrointestinal symptoms and central nervous system symptoms [Pearce, 2006]. This case presented with restlessness, tachycardia and vomiting, but with normothermia which is an unusual presentation. Unusual presentations, such as normothermic crisis, hepatic failure or apathetic storm are very rare [Boelaert et al. 2010; Nordyke et al. 1988; Ho et al. 1998]. The exact reason this case was normothermic is not known, however normothermic crisis has been reported previously, especially in the elderly. Jiang and colleagues have reported a normothermic, normotensive presentation of thyroid storm accompanied by multiple organ dysfunction syndrome in a young patient [Jiang et al. 2000]. Therefore, atypical (normothermic) presentations should not preclude the diagnosis of thyroid storm even in younger patients.
The diagnosis of thyrotoxic storm can be made on clinical findings alone, since it is difficult in most instances to obtain rapid laboratory confirmation. Delay in commencement of therapy for a suspected case of thyroid storm can lead to a poor outcome of management [Carroll and Matfin, 2010]. In addition, biochemical markers of thyroid function may not be different from hyperthyroid patients without thyroid storm [Landsberg, 1977]. The clinical score by Burch and Wartofsky (Table 1) can be used to make a diagnosis of thyroid storm [Burch and Wartofsky, 1993].
Burch and Wartofky scoring system.
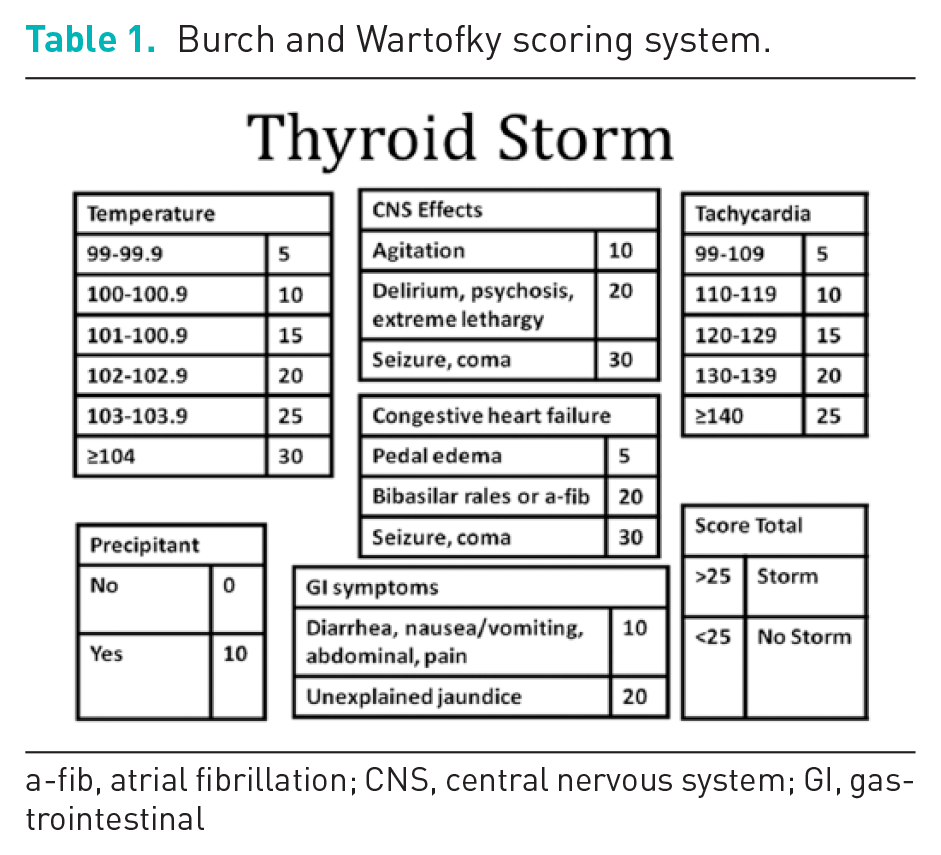

a-fib, atrial fibrillation; CNS, central nervous system; GI, gastrointestinal
A score of 45 or greater is highly suggestive of thyroid storm, a score of 25–44 is suggestive of an impending crisis and less than 25 is unlikely to be thyroid storm.
Conclusion
Thyroid storm is a rare life-threatening hypermetabolic emergency due to thyrotoxicosis that can occur due to noncompliance with medications. Atypical presentations, such as normothermic crisis, hepatic failure or apathetic storm can occur. There is, therefore, the need for clinicians to be aware of these varied atypical clinical features that can make the diagnosis of thyroid storm difficult. There is the need to counsel all thyrotoxic patients on the need for compliance to drugs and clinic follow up.
Footnotes
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Conflict of interest statement
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.