
Abstract
Thyroid storm is a rare and serious endocrine crisis during the perinatal period and typically occurs in patients with Graves’ disease. We present the case of a postpartum woman without prior history of thyroid disease who presented with vomiting, fever, irregular abdominal pain, and a diagnosis of intrauterine death. Despite comprehensive treatment, she showed persistent tachycardia, fever, and multi-organ failure. Diagnostic assessment revealed elevated thyroid hormone levels, and she was diagnosed with thyroid storm based on the scoring system of Burch–Wartofsky and the Japanese Thyroid Association diagnostic criteria. Treatment included plasmapheresis, β-blockers, iodine solutions, antithyroid drugs, and corticosteroids. Following successful mitigation of thyroid storm, she developed hypothyroidism and was treated with levothyroxine. For patients with no history of thyroid disease or negative thyroid autoantibodies, especially postpartum women, presenting unexplained symptoms such as tachycardia, fever, diarrhea, sweating, and altered consciousness, the possibility of thyroid storm should be considered.
Introduction
Thyroid storm is an acute and life-threatening complication of thyrotoxicosis, characterized by manifestations such as high fever, tachycardia, diarrhea and vomiting, jaundice, or multiple organ failure including heart failure, respiratory failure, and renal insufficiency. 1 As an endocrine emergency, thyroid storm is associated with high mortality, estimated to be 10%–30% in previous reports. 2 An abrupt release of large amounts of thyroid hormones into circulation is believed to be the direct cause. Thyroid storm often occurs in patients with underlying hyperthyroidism, either unrecognized or longstanding Graves’ disease, and is often precipitated by factors such as thyroid or radioiodine therapy, infections, trauma, acute illness, delivery, or the introduction of a large amount of iodine into body (including iodinated contrast agent or drugs). 3 Here, we report the case of a 28-year-old woman without previous thyroid disease who experienced a thyroid storm during the perinatal period following infection and obstetric complications.
This case was approved by the Ethics Committee of Suzhou Hospital Affiliated to Nanjing Medical University. The reporting of this case conforms to the Case Report (CARE) guidelines. 4 The patient provided written consent for publication of this case report.
Case presentation
A gravida 3, para 1 woman in her late 20s at 36 weeks of gestation presented to the emergency room of Suzhou Hospital Affiliated to Nanjing Medical University on May 2024 with vomiting, fever, irregular abdominal pain, and a diagnosis of intrauterine death, confirmed the previous day at another hospital. Her obstetric history included an uneventful vaginal delivery of a healthy infant 8 years prior and an induced abortion 4 years earlier. She had no history of thyroid disease and her prenatal exams were unremarkable except for anemia.
Diagnostic assessment
At presentation, she had a high fever of 40°C, sinus tachycardia (134 bpm), and blood pressure of 102/69 mmHg. Physical examination showed no other abnormalities. Laboratory results showed increased leukocytes (16.26 × 109/L, reference range: 3.5–9.5 × 109/L), increased neutrophils (15.79 ×109/L, reference range: 1.8–6.3 × 109/L), and decreased lymphocytes (0.34 × 109/L, reference range: 1.2–3.2 × 109/L); abnormal liver function (alanine aminotransferase 55 U/L, reference range: 0–35 U/L; aspartate aminotransferase 267 U/L, reference range: 14–36 U/L; total bilirubin 43.23 μmol/L, reference range: 3–19 μmol/L; indirect bilirubin 30.85 μmol/L, reference range: 0–19 μmol/L; alkaline phosphatase 349 U/L, reference range: 38–126 U/L); increased creatine level (168 μmol/L, reference range: 46–92 μmol/L), and a high level of N-terminal pro-B-type natriuretic peptide (6640 pg/mL, reference range: 0–300 pg/ml). The level of C-reactive protein (CRP) was increased at 38.56 mg/L (reference range: 0–10 mg/L). Following admission, she delivered a stillborn male infant with notable foul odor from the uterus and concurrently experienced postpartum hemorrhage.
She received comprehensive treatment, including cooling therapy, antibiotics (meropenem 1 g every 8 hours; teicoplanin 600 mg once a day, with dosage adjustments based on serum concentration), blood transfusion, fluid resuscitation, and pressor treatment. Despite symptomatic treatment, her vital signs remained unstable, necessitating transfer to the intensive care unit (ICU) for further treatment. Her Acute Physiology and Chronic Health Evaluation II (APACHE II) score was 19.
On the fourth day after delivery, she continued to exhibit high fever with persistent sinus tachycardia (shown in Figure 1). Laboratory results showed increased leukocytes (36.83 × 109/L) and CRP (116.16 mg/L). Blood routine revealed elevated inflammatory indicators, while blood-based metagenomic next-generation sequencing analysis revealed the presence of Streptococcus pyogenes, which was sensitive to the currently antibiotic regimen. An etiological examination of genital tract secretions identified the presence of Candida glabrata, which is generally regarded as a colonizing organism. Thyroid function measurement demonstrated hyperthyroidism (shown in Figure 1, thyroid-stimulating hormone (TSH) 0.1361 μIU/mL, reference range: 0.35–4.94 μIU/mL; free thyroid hormone (FT4) > 64.35 pmol/L, reference range: 9.01–19.05 pmol/L; free triiodothyronine (FT3) 21.26 pmol/L, reference range: 2.43–6.01 pmol/L). Thyroid autoantibody measurement showed thyroglobulin antibody 2.29 IU/mL (reference range: 0–34 IU/mL), thyroid peroxidase antibody 14.94 IU/mL (reference range: 0–12 IU/mL), thyroid-stimulating antibody 0.1 IU/mL (reference range: 0–0.55 IU/L), and thyroid receptor antibody <0.8 IU/L (reference range: 0–1.75 IU/L). Computed tomography and thyroid ultrasound revealed a slightly enlarged gland (with patchy low echoes and diffuse changes; left lobe: 25 × 50 × 26 mm, right lobe: 20 × 55 × 21 mm, isthmus thickness: 5.2 mm). According to the Burch–Wartofsky Point Scale (BWPS), the patient scored 75 points (based on manifestations including body temperature of 40°C, agitation status, recent diarrhea, heart rate >140 bpm, pedal edema, and jaundice). According to the Japan Thyroid Association (JTA) diagnostic criteria, the patient had thyrotoxicosis, fever, tachycardia, diarrhea, jaundice, and was classified as “definite” thyroid storm (TS1). By combining BWPS and JTA diagnostic criteria, the patient was diagnosed with thyroid storm. The timeline for diagnosis and treatment is summarized in Figures 1 and 2.

An overview of the treatment process, encompassing changes in body temperature, thyroid function, and adjustments to medication throughout the entire course of therapy. FT3: free triiodothyronine; FT4: free thyroid hormone; MMI: methimazole; PTU: propylthiouracil; TSH: thyroid-stimulating hormone.
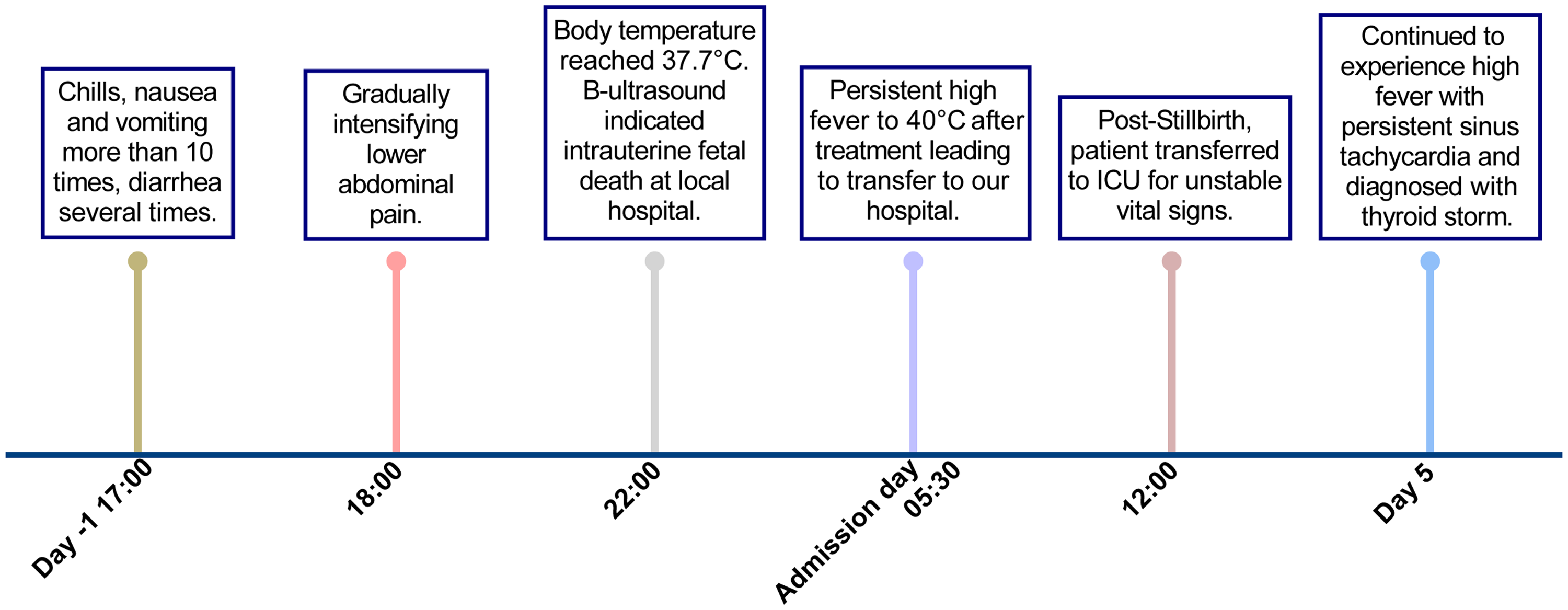
The timeline for diagnosis. ICU: intensive care unit.
Treatments and prognosis
Due to sepsis, severe multi-organ failure, and unstable vital signs, she underwent plasmapheresis 3 times after the diagnosis of thyroid storm was confirmed. In addition, propranolol (20 mg every 8 hours), iodine solutions (0.2 mL three times daily), and hydrocortisone (100 mg every 8 hours) were administered. After liver function improved, propylthiouracil (PTU) (100 mg every 8 hours) was initiated. Throughout PTU treatment, liver function remained normal. After 7 days of PTU, her thyroid function improved (shown in Figure 1; TSH 0.0074 μIU/mL, FT4 62.57 pmol/L, FT3 3.06 pmol/L). Thus, hydrocortisone was decreased to 50 mg every 12 hours, and PTU was replaced with methimazole (MMI) for 10 mg once daily. Repeated assessment of inflammatory markers revealed normalization of CRP (1.75 mg/L), although the white blood cell count remained mildly elevated (16.09 × 109/L). Meropenem and teicoplanin were discontinued, and antibiotic therapy was transitioned to levofloxacin (0.5 g once daily) for 4 days. After another 7 days of MMI, her thyroid hormone levels dropped rapidly (shown in Figure 1; TSH 0.0056 μIU/mL, FT4 25.85 pmol/L, FT3 <2.30 pmol/L), and MMI was discontinued. Approximately 10 days after discontinuing MMI, her FT4 level continued to decline. With the context of no history of thyroid disease and low titers of thyroid antibody, levothyroxine (25 μg once daily) was prescribed.
After the patient’s temperature, heart rate, and liver and kidney function returned to normal, she was discharged with the treatment plan of levothyroxine (50 μg once daily) and metoprolol (47.5 mg in the morning, 23.75 mg in the evening). Thyroid function was measured 1 and 4 months after discharge (1-month: TSH 0.0635 μIU/mL, FT4 9.1 pmol/L, FT3 4.02 pmol/L; 4 months: TSH 5.86 μIU/mL, FT4 12.97 pmol/L, FT3 4.37 pmol/L). She was administered levothyroxine (50 μg once daily) based on the thyroid function diagnosis of hypothyroidism.
Discussion
The sudden release of thyroid hormone causes thyroid storm, a life-threatening endocrine emergency with rapid progression and high mortality in clinical practice. 1 Most cases develop from unrecognized or uncontrolled Graves’ disease, which is the most common cause of hyperthyroidism.5,6 The definite etiology and triggers of thyroid storm are not always apparent. Various medical interventions, including thyroidectomy, non-thyroid surgery, radioiodine therapy, exposure to excessive iodine agents or drugs, or the ingestion of an excessive amount of thyroid hormone, can trigger thyroid storm. 3
Early recognition, timely diagnosis, and intensive treatment are crucial to improving the survival rate and prognosis of patients with thyroid storm. However, the complexity and nonspecific symptoms of thyroid storm can complicate diagnosis. 6 In 1993, the BWPS was proposed for diagnosing thyroid storm. 7 By assessing the severity of multi-organ involvement, including body temperature, central nervous system symptoms, tachycardia or atrial fibrillation, congestive heart failure, gastrointestinal and liver dysfunction, as well as precipitating factors, BWPS is a scoring system developed based on clinical experience. It has been suggested that BWPS might be too sensitive to result in a false positive diagnosis. In 2012, the JTA introduced new diagnostic criteria for thyroid storm based on 99 published cases and case reports. 8 These criteria require thyrotoxicosis as a prerequisite, along with central nervous system symptoms, fever, tachycardia, congestive heart failure, or gastrointestinal/hepatic dysfunction. 8 Currently, both scoring systems are widely used in the diagnosis of thyroid storm in clinical practice.
In our case, the patient was admitted due to vomiting and high fever without prior thyroid history. Despite comprehensive treatment such as cooling therapy and antibiotic therapy, the patient exhibited persistent tachycardia, fever, and multi-organ failure including congestive heart failure and liver and renal dysfunction. Thyroid function measurement showed that FT3 and FT4 were extremely high. According to the BWPS system, her score was 75, leading to a diagnosis of thyroid storm. According to JTA diagnostic criteria, she was classified as TS1.
Several aspects are important in the treatment of thyroid storm, with the paramount objective being to swiftly mitigate circulating thyroid hormone levels, alleviate symptoms, and prevent the onset of complications. 9 In addition to supportive care, this patient received plasmapheresis, β-blockers (propranolol), inorganic iodides, antithyroid drugs (ATDs, namely PTU and MMI), and corticosteroids (hydrocortisone). Plasmapheresis, an efficacious emergency intervention, rapidly removes thyroid hormones by extracorporeal elimination of plasma protein-bound T3/T4, thereby buying critical time for subsequent therapeutic interventions. 10 Several guidelines propose considering plasmapheresis in severe patients or those who are refractory to ATD treatment. 11 β-blockers, notably propranolol, effectively manage symptoms such as tachycardia, and at elevated doses, additionally hinder the peripheral conversion of T4 to T3 by inhibiting type 1 deiodinase, further mitigating the hormonal surge. 6 Iodine solutions can stabilize the condition by inhibiting the further release of thyroid hormones. 12 Glucocorticoids help reduce the inflammatory response of thyroid tissue and maintain adrenal cortex function. 6 Notably, impaired liver function initially prevented immediate use of ATDs (such as PTU), which were initiated as liver function gradually recovered. In this case, PTU was chosen as the first-line antithyroid drug due to its rapid onset of action and the ability to inhibit both thyroid hormone synthesis and the peripheral conversion of T4 to T3, which is particularly important in treating thyroid storm.6,13
Upon successful mitigation of the thyroid storm, the patient subsequently manifested signs of hypothyroidism, a prevalent sequela after thyroid storm management, particularly in instances of acute hyperthyroidism exacerbation. In this case, the patient was treated with levothyroxine starting at 25 μg once daily and gradually adjusted to 50 μg once daily based on thyroid function monitoring. Thyroid hormone was in the normal range after discharge.
It should also be noted that she had no previous history of thyroid disease and developed severe septic shock at the beginning of the disease. Thyroid storm typically happens in patients with Graves’ disease. It is very rare for thyroid storm to occur in destructive thyroiditis, toxic multinodular goiter, TSH-secreting pituitary adenoma, human chorionic gonadotropin-secreting hydatidiform mole, or metastatic thyroid cancer.13–15 Symptoms such as sustained tachycardia and vomiting in our case were difficult to attribute to a diagnosis of thyroid storm at first. In a series case report, thyroid storm in patients with no prior history of thyroid disease may begin with septic shock in the ICU, and sepsis can simulate thyroid storm. 16 Therefore, thyroid storm should be considered and thyroid function should be measured when symptoms such as tachycardia, fever, diarrhea, and abnormal consciousness cannot be explained by infection alone.
In addition, this unusual case developed after labor induction. Risk factors for thyroid storm during pregnancy or postpartum mainly include untreated or uncontrolled hyperthyroidism, infection, diabetic ketoacidosis, severe mental stimulation, pregnancy and delivery, trauma, and cardiovascular and cerebrovascular diseases. 13 Infection and labor induction may have been the precipitators of thyroid storm in this case. Systemic inflammatory response to infection may stimulate the massive release of thyroid hormones, possibly mediated by elevated inflammatory mediators like interleukin-6 and tumor necrosis factor α, which can act directly on the thyroid gland to promote thyroid hormone secretion. 14 The stress response caused by infection can lead to increased levels of catecholamines, which can further burden the heart and lead to symptoms such as tachycardia. 15 Infection may activate the immune system, increasing the autoimmune response of the thyroid, thus exacerbating the hyperthyroidism. 17 However, thyroid peroxidase antibody titers remained at low levels in this case, and thyroid receptor antibody titers remained negative during treatment and follow-up. Unfortunately, the patient has been lost to follow-up, and no subsequent antibody changes have been observed. During pregnancy, elevated estrogen levels prompt an augmentation in the synthesis of thyroid-binding globulin, leading to an increase of total serum thyroid hormone concentrations, while free thyroid hormone levels remain relatively stable. However, acute infection and stress disrupt this equilibrium, resulting in abnormal elevations of free thyroid hormones. 18
This case highlights that thyroid storm can occur during the perinatal period, even in individuals without a prior history of thyroid disease. When patients exhibit symptoms such as tachycardia, high fever, diarrhea, sweating, and altered consciousness, and these symptoms cannot be adequately attributed to a solitary condition such as infection, the potential for a thyroid storm should be seriously considered. In postpartum women, even with no history of thyroid disease or negative thyroid autoantibodies, special attention also should be given to the potential occurrence of a thyroid storm. Prompt identification, coupled with vigorous multidisciplinary management strategies and carefully monitoring, is paramount in stabilizing patients and averting potentially life-threatening complications.
Footnotes
Acknowledgements
We thank the patient in this case and the intensive care unit medical staff for their invaluable assistance in the treatment of this case.
Authors’ contributions
Data availability
The clinical data of the patient are available from the corresponding author upon request.
Declaration of conflicting interests
All authors declare that there are no conflicts of interest and have nothing to declare.
Funding
This research received no funding.