
Abstract
Osteoporosis affects a substantial proportion of patients with chronic liver disease. Pathologic fracture in osteoporosis significantly affects quality of life and life expectancy. By some estimates, 40% of patients with chronic liver disease may experience osteoporotic fracture. In this study we review the pathogenesis, diagnosis and treatment of specific liver disease entities and their relation to osteoporosis.
Introduction
Hepatic osteodystrophy refers to osteoporosis and osteomalacia associated with chronic liver disease. Osteoporosis is a disorder of low bone mass, microarchitectural malformation and structural weakness while osteomalacia is a disorder of decreased osteoid mineralization at sites of bone formation. Liver is involved in a number of metabolic mechanisms. Therefore, it is not surprising that liver disease is one of the secondary causes of osteoporosis and approximately 30% of patients with chronic liver disease suffer from osteoporosis. However, aetiology of bone loss is multifactorial and not entirely understood. Patients with cholestatic liver disease are particularly susceptible to osteoporosis due to the interference of cholestasis with vitamin D metabolism. Clinical conditions for which early diagnosis of osteoporosis are indicated are given in Table 1 [Guañabens and Parés, 2011; Collier et al. 2002].
Indications for bone mineral density measurement [Guañabens and Parés, 2011; Collier et al. 2002].
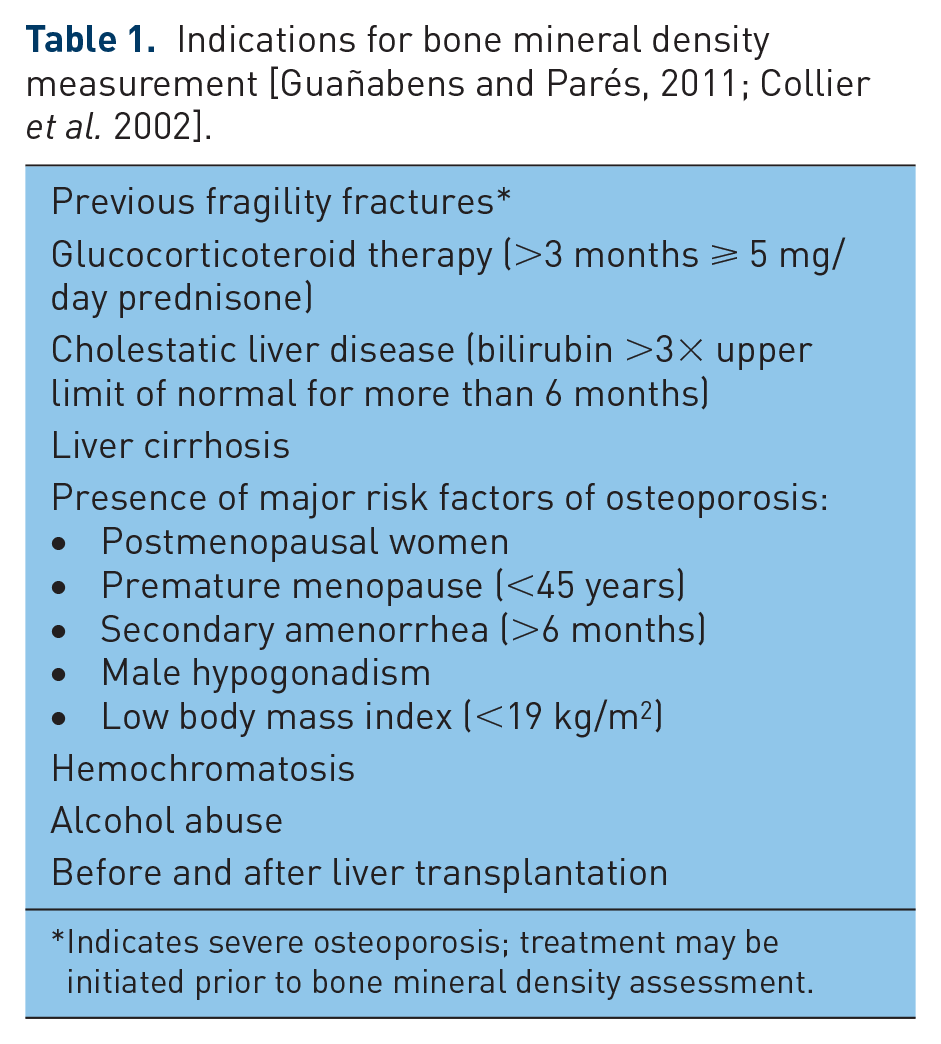
Indicates severe osteoporosis; treatment may be initiated prior to bone mineral density assessment.
Pathogenesis
The pathogenesis of osteoporosis in chronic liver disease is complex and related to both increased bone resorption [Crosbie et al. 1999] and reduced bone formation [Collier et al. 2002; Gallego-Rojo et al. 1998]. Unstable bone remodelling is caused by a number of mechanisms, some of which remain unknown. In many cases, the mechanisms of impaired bone metabolism are largely caused by the unique characteristics of the specific liver disease being considered. However, there remain a number of common factors related to chronic liver disease in general that affect bone metabolism. These include vitamin D and calcium metabolism alterations, vitamin K deficiency, and hormonal dysregulation, the release of cytokines and deficiency of insulin-like growth factor 1 (IGF-1).
Vitamin D3 is hydroxylated in the liver to 25-hydroxy vitamin D (25-OH-vitamin D) and then in the kidneys to 1,25-hydroxyvitamin D. Decreased 25-OH-vitamin D production is associated with altered liver function and it results in impaired osteoclast-mediated bone resorption, osteoblast-mediated mineralization and decreased calcium resorption in the gastrointestinal tract [Van Leeuwen et al. 2001]. Additionally, disturbed secretion of bile leads to decreased fat absorption and abnormal uptake of vitamin D as a result. To summarize, disturbed metabolism of calcium and vitamin D results from impaired 25-hydroxylation, intestinal malabsorption and decreased skin synthesis in patients with jaundice [Van Leeuwen et al. 2001].
IGF-1 mediates a number of biological effects of growth hormone (GH) and is also involved in the negative feedback mechanism of GH secretion from the pituitary gland [Burra et al. 2010]. IGF-1 is produced in the majority of hepatocytes and feedback is inhibited by GH. In patients with chronic liver disease with advanced cirrhosis, GH secretion is increased twofold. Increased pulse frequency and a longer half life of GH both contribute to the greater availability [Cuneo et al. 1995]. Reduced production of IGF-1 from the cirrhotic liver leads to inhibition of the GH axis negative feedback mechanism, thereby reducing GH levels in healthy individuals.
Interleukin-1 (IL-1), IL-6 and tumour necrosis factor α (TNFα) enhance the activity of osteoclasts. Increased concentrations of these cytokines are found in cases of cirrhosis, hepatitis and alcoholic liver disease [Luxon, 2011]. IL-6 is produced by osteoblasts which directly and indirectly activates osteoclasts. IL-6 indirectly activates osteoclasts by stimulating osteoblast production of receptor activator of nuclear factor κB ligand (RANKL). RANKL and osteoprotegerin are among the best known cytokines involved in the regulation of bone homeostasis. Receptor activator of nuclear factor κB (RANK) leads to activation of osteoclasts, thereby increasing bone resorption. Osteoprotegerin inhibits binding of RANKL with RANK, thereby preventing loss of bone mass. In the early stages of liver disease increased levels of RANKL and normal osteoprotegerin concentration result in increased bone resorption. However, as liver disease progresses, the concentration of RANKL remains within the normal range while the concentration of osteoprotegerin increases. This phenomenon may be secondary to impaired osteoblast function, which leads to decreased production of RANKL and thus reduced bone resorption. Decreased osteoblast activity also leads to impaired bone formation, which is reflected in the reduction in the concentration of osteoblast-specific protein, osteocalcin [Nakchbandi, 2014].
Adipose tissue derived cytokines, called adipokines, also play an important role in the pathogenesis of osteoporosis. In the context of bone metabolism disorders, the best known adipokine is leptin. Adipokines inhibit osteoclastogenesis by decreasing the synthesis of RANKL and increasing osteoprotegerin levels. Moreover, leptin stimulates the synthesis of proinflammatory cytokines, particularly IL-1 and TNFα [Szalay et al. 2005].
In light of the reduced levels of vitamin D seen in chronic liver disease, it should be noted that there is a relatively low incidence of significant parathyroid hormone (PTH) disturbances associated with decreased vitamin D concentrations [Miroliaee et al. 2010]. This paradox in the vitamin D–PTH regulation pathway may be related to genetic polymorphism of the vitamin D receptor (VDR), which may result in the suppression of PTH secretion. The exact pathophysiological mechanism is not yet fully understood [Miroliaee et al. 2010].
Other causes of impaired bone turnover in liver disease are presented in Table 2.
Factors impairing bone turnover in chronic liver disease [Collier et al. 2002; Crosbie et al. 1999; Luxon, 2011; Szalay et al. 2005; Goral et al. 2010; López-Larramona et al. 2011, 2015].

BMI, body mass index; IGF-1, insulin-like growth factor 1; RANKL/OPG, receptor activator of nuclear factor κB ligand/osteoprotegerin; IL-6, interleukin 6.
Osteoporosis in specific liver disease entities
Cirrhosis doubles the risk of pathological fractures, regardless of the aetiology of cirrhosis. The total incidence of osteoporosis in patients with cirrhosis varies from 12% to 55%, with the incidence of fracture between 5% and 20% [Luxon, 2011; López-Larramona et al. 2011]. Such a large discrepancy is primarily due to differences in the age and stage of the disease between treatment groups [Luxon, 2011].
Cholestatic liver diseases
Primary biliary cirrhosis (PBC) increases the incidence of osteoporosis up to four times and increases the probability of osteoporotic fracture twofold. The prevalence of osteoporosis in patients with PBC reaches 20–44% [Raszeja-Wyszomirska and Miazgowski, 2014]. Only 20% of patients with advanced stage PBC and primary sclerosing cholangitis (PSC) retain bone mineral densities (BMDs) in the normal range [Guichelaar et al. 2006]. Both the duration and severity of PBC reflect the extent of the dysfunction of bone metabolism [Crosbie et al. 1999].
Cirrhosis and steroid therapy contribute to a reduction of BMD in patients with PSC associated with inflammatory bowel disease (IBD). IBD may coexist in over 90% of patients with PSC [Saich and Chapman, 2008]. In addition, PBC is more common in postmenopausal women who are already at increased risk of metabolic bone disease.
The role of adipokines in bone metabolism has been confirmed in a number of studies. However, the significance of changes in plasma levels of specific adipokines in the pathogenesis of osteoporosis in patients with PBC and PSC has not yet been established. The result of studies evaluating the plasma concentrations of leptin in these patient populations has proved to be largely contradictory [Szalay et al. 2005; Ben-Ari et al. 2002; García-Suárez et al. 2004; Breidert et al. 2004]. In patients with PBC there exists a negative correlation between adiponectin and BMD [Floreani et al. 2008]. It remains to be established whether increased concentrations of adipokines is part of the pathogenesis of PBC, or is rather a complication of the disease.
Vitamin D deficiency and genetic polymorphisms of VDRs appear to be key features of PBC. VDR gene polymorphisms are associated with an increased risk of certain cancers, for instance cancer of the skin and mammary glands. Recent studies also point to the role of these VDR polymorphisms in the development of PBC. B gene allele of Bsm1 and t gene allele of Taq1 are observed significantly more often in patients with PBC. These genotypes were also significantly associated with a higher risk of advanced fibrosis at the time of diagnosis of PBC [Kempińska-Podhorecka et al. 2012]. The results of studies conducted on the role of VDR gene polymorphism in the development of osteoporosis in patients without liver disease are discrepant. Some polymorphisms (BsmI, ApaI, TaqI, 283G/A) have been shown to be associated with lower BMD or higher risk of low-energy fractures [Boroń et al. 2015; Horst-Sikorska et al. 2013]. It may be hypothesized that specific VDR genotypes enhance the risk of osteoporosis development irrespectively of liver disease (e.g. via alterations in vitamin D endocrine system), but they may also increase incidence and severity of PBC, which may later relate to the development of osteoporosis in these patients [Springer et al. 2000]. The exact mechanism of action of VDR gene polymorphisms in osteoporosis in PBC requires further investigation.
Cholestasis is considered by many scholars to be one of the major risk factors for osteoporosis [Guañabens et al. 2005]. Recent studies indicate, however, that the use of ursodeoxycholic acid, which has been shown to improve cholestasis, does not result in an increase in BMD [European Association for the Study of the Liver, 2009]. Lack of correlation between improvement of cholestasis and BMD suggests that advanced cirrhosis may be responsible for changes in bone metabolism rather than the cholestasis of PBC. Influence of auto antibodies on bone metabolism cannot be excluded due to the role of immune system cells in osteoporosis development which has been previously investigated [Demirdal et al. 2010; Faienza et al. 2013]. Environmental factors that contribute to the development of osteoporosis, such as smoking, low body weight, and age and sex, also appear to outweigh the risks associated with cholestasis [European Association for the Study of the Liver, 2009]. Additional risk factors for osteoporosis, which are indications for bone densitometry in patients with PSC and PBC include liver transplantation, increased indicators of cholestasis, progressive malnutrition and a history of corticosteroid use [Raszeja-Wyszomirska and Miazgowski, 2014]. Distal renal tubular acidosis, which is a renal complication of PBC, has also been considered as one of risk factors of osteoporosis in PBC, but the data in this field are inconsistent [Farias et al. 2005].
Hemochromatosis
Hemochromatosis predisposes patients to osteoporosis, especially when complicated by hypogonadism [López-Larramona et al. 2011]. The prevalence of osteoporosis in patients with primary hemochromatosis has not been associated with any specific genetic aetiologies of the disease. Valenti and colleagues showed that 25% of patients with hemochromatosis have osteoporosis and that 41% have osteopenia [Valenti et al. 2009]. In addition, a small subgroup of 36 patients with hemochromatosis and without evidence of hypogonadism, cirrhosis of the liver or menopause had developed osteoporosis (8%) or osteopenia (61%). Singalia and colleagues showed similar results [Sinigaglia et al. 1997]. Increased iron concentrations seem to convey an equally high predictive value for osteoporosis as they do for cirrhosis of the liver, and the greater the iron load the greater the risk of metabolic bone disease [Valenti et al. 2009]. Increased BMD has been observed in up to 66% of patients treated by phlebotomy. However, the confounding role of improved gonadal function remains to be elucidated [Valenti et al. 2009].
Nonalcoholic fatty liver disease and nonalcoholic steatohepatitis
Metabolic syndrome (MS) has been associated with the development of osteoporosis [Yilmaz, 2012]. Nonalcoholic fatty liver disease (NAFLD) may result as a complication of MS. NAFLD may lead to nonalcoholic steatohepatitis (NASH) and eventually cirrhosis. In addition, NAFLD has been recognized as a potential risk factor for reduced BMD. Moon and colleagues observed reduced BMD of the lumbar spine in postmenopausal patients with NAFLD, regardless of the presence of MS, and after taking into account other risk factors for low BMD (body mass index, age, and smoking) [Moon et al. 2012]. Decreased BMD in NAFLD appears to be independent of sex, which is consistent with the results of a retrospective study involving more than 7000 men, in which the presence of NAFLD was associated with a 2.5-fold increased risk of osteoporotic fractures [Li et al. 2012]. Purnak and colleagues did not observe a relationship between simple steatosis and BMD [Purnak et al. 2012]. However, in patients with elevated alanine transaminase levels and C-reactive protein suggestive of NASH, BMD was significantly reduced [Purnak et al. 2012].
The phenomenon of reduced BMD in steatotic liver disease is also observed in children [Pardee et al. 2012]. Of 36 children diagnosed with NAFLD in liver biopsy as many as 45% had lower BMD than healthy children matched for sex, age and body weight. In addition, children with NASH had lower BMD’s than patients with simple steatosis [Pardee et al. 2012; Armstrong et al. 2014].
The mechanism of decreased bone mineralization in NAFLD is not fully understood. However, an important role is attributed to cytokines secreted by chronic subclinical inflammation associated with obesity [Yilmaz, 2012]. Increased concentrations of TNFα have been repeatedly observed in NAFLD. This factor is involved in the stimulation of osteoclastogenesis (including induction and secretion of IL-6 and colony-stimulating factor macrophages) and the inhibition of osteoblast progenitor cells [Yilmaz, 2012]. TNFα has also been shown to reduce the production of alkaline phosphatase, vitamin D receptors and PTH receptors, and other factors involved in bone formation. The level of bone metabolism disruption is indicated by the level of markers osteopontin, osteoprotegerin, osteocalcin and fetuin A [Yilmaz, 2012]. While the mechanism has not been fully elucidated, it is known that NAFLD is associated with biochemical markers of metabolic bone disorders, and vice versa.
Viral hepatitis
In patients with cirrhosis as a consequence of viral hepatitis, the prevalence of osteoporosis is similar to patients with cirrhosis due to other causes of liver disease and comprises 20–53% of all patients [Luxon, 2011]. Hepatitis B and C have been shown to increase the concentration of proinflammatory cytokines and promote reductions in bone mass. According to Schiefke and colleagues, bone density measurements in patients with hepatitis B and C were significantly reduced in the absence of changes typical for cirrhosis [Schiefke et al. 2005]. As liver fibrosis progresses so too deepens the BMD deficit. Viral hepatitis is unique among other aetiologies of liver disease in that increased concentrations of serum PTH have been observed [Schiefke et al. 2005].
Alcoholic liver disease
Alcohol abuse and chronic liver disease cause endocrine and metabolic disorders favouring a reduction in BMD. Factors affecting increased bone resorption include eating disorders and the direct effect of ethanol on bone resorption. Alcohol enhances the activity of osteoclasts via induction of IL-6, TNFα and IL-1β activation of RANKL. In both experimental and clinically confirmed studies, a dose-dependent effect of alcohol on osteoblasts has been observed, which results in the inhibition of bone formation, resulting in a decrease in bone turnover [López-Larramona et al. 2013].
Liver transplantation
Disorders of bone homeostasis in patients who undergo liver transplantation are influenced both by liver disease and immunosuppressive therapy [Bjøro et al. 2003]. BMD falls substantially within 3–6 months of transplantation and increases to pretransplantation within 2 years [Monegal et al. 2001]. The rate of return to the initial BMD depends on immunosuppression [Luxon, 2011]. Post-transplantation bone biopsies show that tacrolimus-based immunosuppression leads to faster normalization of bone metabolism than the use of cyclosporine. It is probable that immunosuppression protocols with lower steroid doses also improve bone metabolism [Luxon, 2011].
Diagnosis and treatment
Patients with chronic liver disease are classified as medium or high risk according to the risk factors associated with developing osteoporosis. Given the risk of osteoporosis-related liver injury, all patients with confirmed liver disease should be screened. Modifiable risk factors should be corrected in an effort to maintain or limit the extent of BMD loss. According to the American Association for the Study of Liver Disease, patients with autoimmune hepatitis on long-term corticosteroid treatment should be monitored for bone disease at baseline and then annually [Manns et al. 2010].
We recommend determining serum 25-OH-vitamin D levels and supplementation if a deficiency is detected [Płudowski et al. 2013]. According to Endocrine Society clinical practice guidelines, 25-OH-vitamin D requirements in chronically ill patients are greater than in healthy individuals and blood levels of 25-OH-vitamin D above 30ng/ml should be achieved, as this may provide additional health benefits [Holick et al. 2011]. In patients with cirrhosis, previously diagnosed with osteoporosis during treatment with glucocorticoid steroids, supplementation with calcium and vitamin D is justified without performing laboratory tests. Other modifiable risk factors include smoking, alcohol abuse and malnutrition. Significantly, it is important to maintain ambulation and physical exercise whenever possible.
Densitometry tests should be ordered for patients with chronic liver disease to estimate the absolute risk of fracture. Dual energy X-ray absorptiometry bone densitometry can also be used to obtain data about bone quality by the means of trabecular bone score and hip structural analysis assessment. Using the FRAX calculator [Głuszko et al. 2014], one can determine when to begin appropriate pharmacological therapy. Note, however, that the assessment of BMD in patients with cirrhosis, both when measured at the lumbar spine as well as within the proximal femur, is difficult due to decreased densitometric accuracy in patients with ascites [Guañabens et al. 2012]. Multisite bone ultrasound methods are new, alternative tools, which could be successfully used in these patients as a diagnostic option in the future [Karjalainen et al. 2016]. The gold standard for diagnosis of osteomalacia is bone biopsy, but this method is not recommended for patients with liver disease due to its invasiveness. Osteoporosis is a relatively common complication of cholestatic liver disease and for this reason has been relatively well studied. The European Association for the Study of the Liver issued recommendations in 2009, according to which all patients with cholestatic liver disease should be screened with densitometry soon after diagnosis [European Association for the Study of the Liver, 2009]. Furthermore, annual checkups should be provided, especially in patients with environmental risk factors [European Association for the Study of the Liver, 2009]. In patients with PBC and PSC, the European Association for the Study of the Liver recommends considering supplementation with calcium (1000–1200 mg/day) and vitamin D (400–800 IU / day), noting that its effectiveness has not been proven. Alendronate or other bisphosphonates are recommended with T scores less than −2.5 or less than −1.5 or in cases where osteoporotic fracture has occurred [European Association for the Study of the Liver, 2009]. Particular attention should be paid to the potential side effects of bisphosphonates, including ulceration of the gastrointestinal tract. In patients with oesophageal varices in whom treatment with bisphosphonates appears to be necessary, intravenous dosing should be considered. In patients with autoimmune hepatitis with pre-existing osteoporosis, combination therapy with prednisolone and azathioprine should be preferred to monotherapy with prednisolone [European Association for the Study of the Liver, 2015]. Patients undergoing treatment at dose equivalent glucocorticoids (GC) at least 5 mg/day of prednisone for 3 months or more should be considered for treatment with bisphosphonates. Preventive administration of oral bisphosphonate therapy prior to the scheduled GC should also be considered [Głuszko et al. 2014].
Hormone replacement therapy (HRT), although initially considered a second-line therapy, is contraindicated in severe liver disease. Contradictory studies as to the effectiveness of HRT make the therapy unsuitable for the treatment of osteoporosis in liver disease [Luxon, 2011].
Treatment of viral liver disease associated osteoporosis appears to be a causal treatment geared to achieve sustained suppression of hepatitis B virus replication or hepatitis C virus sustained viral response [Arase et al. 2010]. It has been shown that the incidence of osteoporotic fractures in patients with hepatitis C is significantly reduced after successful interferon therapy. In postmenopausal women treated with interferon, the risk of osteoporotic fractures was reduced by 66% [Arase et al. 2010].
A causal treatment of liver diseases is a fundamental element of prevention and therapy of osteoporosis in these patients. However, detailed management of a particular liver disorder exceeds the aim of this review.
Summary
The liver is an organ involved in a number of metabolic and hormonal processes whose dysregulation may lead to the development of bone homeostasis disorders and ultimately to osteopenia and osteoporosis. Complications of chronic liver disease should therefore include pathologic osteoporotic fractures, which significantly reduce quality of life. Despite this, disorders of bone metabolism in patients with liver disease are often overlooked in clinical practice, as demonstrated by the frequent omission of supplemental calcium and vitamin D in chronic liver disease. For the prevention of osteoporosis in liver disease, one should address and treat the specific disease modality, eliminate modifiable risk factors and maintain proper diet and supplementation of vitamin D.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.