
Abstract
Metabolic (dysfunction)-associated fatty liver disease (MAFLD) is the most common chronic liver disease worldwide – with an estimated global prevalence of 37%. Different from nonalcoholic fatty liver disease (NAFLD), which is an exclusion diagnosis, MAFLD is defined by a set of positive criteria. This recent change in terminology is challenging because MAFLD and NAFLD denote two similar, albeit not identical, clinical populations. When the diagnostic criteria for MAFLD are applied, liver histology appears more severe and clinical outcomes are less favorable. However, the clinical management of MAFLD and NAFLD remains similar. While liver biopsy is still the reference standard for achieving a final diagnosis, noninvasive imaging- or biomarker-based diagnostic modalities are currently gaining momentum. However, liver biopsy should be recommended when diagnostic challenges exist. In this review, we compared the epidemiology, natural history, and diagnosis of MAFLD with respect to the traditional NAFLD definition.
Keywords
Introduction
Nonalcoholic fatty liver disease (NAFLD) – which is defined as deposition of fat in at least 5% of hepatocytes – encompasses a disease spectrum ranging from nonalcoholic fatty liver (NAFL) to cirrhosis. NAFLD is a diagnosis of exclusion that requires the absence of secondary causes of hepatic steatosis (e.g. alcohol consumption, use of steatogenic drugs, drug abuse, and autoimmune liver disease). 1 After the introduction of the acronym NAFLD by Ludwig in 1980, 2 there has been a continuing debate as to whether this terminology obscures – rather than illuminates – the real etiology of the disease. In recent years, it has been contended that the term NAFLD suffers from major shortcomings – including (1) an overestimation of the lack of alcohol consumption in the pathogenesis of the disease and (2) the neglected role of metabolic factors in disease etiology.3,4 This has prompted significant efforts for rebranding the disease in a more meaningful manner. In 2020, Eslam et al. 5 reached a consensus that recommended ‘metabolic (dysfunction) associated fatty liver disease’ (MAFLD) as a more appropriate name to describe fatty liver disease associated with metabolic dysfunction, ultimately suggesting that the term NAFLD does not reflect current knowledge. Remarkably, the authors proposed a set of positive diagnostic criteria for MAFLD that included the presence of diabetes mellitus, overweight/obesity, and indices of metabolic dysfunction. 5 More recently, age- and sex-adjusted criteria based on standard deviation curves have been proposed for diagnosing MAFLD in pediatric age. 6
The proposal of rebranding NAFLD as MAFLD has sparked a fierce scientific debate as to the most appropriate acronym. The new terminology has been combated by some hepatologists who contended that a lack of information regarding disease etiology was anticipated to have negative effects on drug development. 7 While the acronym NAFLD has not been abandoned yet, an increasing number of recent clinical studies have applied the positive definition of MAFLD and, in some cases, compared the findings with those obtained with the traditional exclusion diagnosis of NAFLD. A consistent finding is that, despite a large overlap, MAFLD and NAFLD do not define the same condition and should not be regarded as synonym.8,9 In this regard, a recent meta-analysis has shown that only 4% of the population under scrutiny was either MAFLD or NAFLD. 10 Starting from these premises, we designed the current review to compare the epidemiology, natural history, and diagnosis of MAFLD versus the traditional NAFLD definition. With this aim, we specifically focused on studies that systematically applied and compared the MAFLD and NAFLD definitions within the same study populations.
Epidemiology
General prevalence and characteristics of MAFLD versus NAFLD
According to 2015 data, 11 the estimated global prevalence of NAFLD was approximately 25%. However, 95% of the study population included in this meta-analysis was from North America, and the diagnosis of hepatic steatosis relied on imaging modalities. On identifying NAFLD based on blood tests, the estimated prevalence appeared significantly lower. 11 A more recent meta-analysis by Chan et al. 12 carried out in more than 3 million people reported that the prevalence of MAFLD was 39%. When interpreting these findings, it should be noted that nearly 90% of the participants were of Asian descent. In addition, the diagnostic modality for detecting hepatic steatosis was found to affect the final prevalence rates [fatty liver index (FLI) = 28%; imaging methods = 37%]. 12 While both meta-analyses reported high prevalence rates of either NAFLD 11 or MAFLD, 12 a direct comparison appears problematic in light of different study populations, diagnostic techniques, and time periods (Table 1).
Comparison of MAFLD and NAFLD.
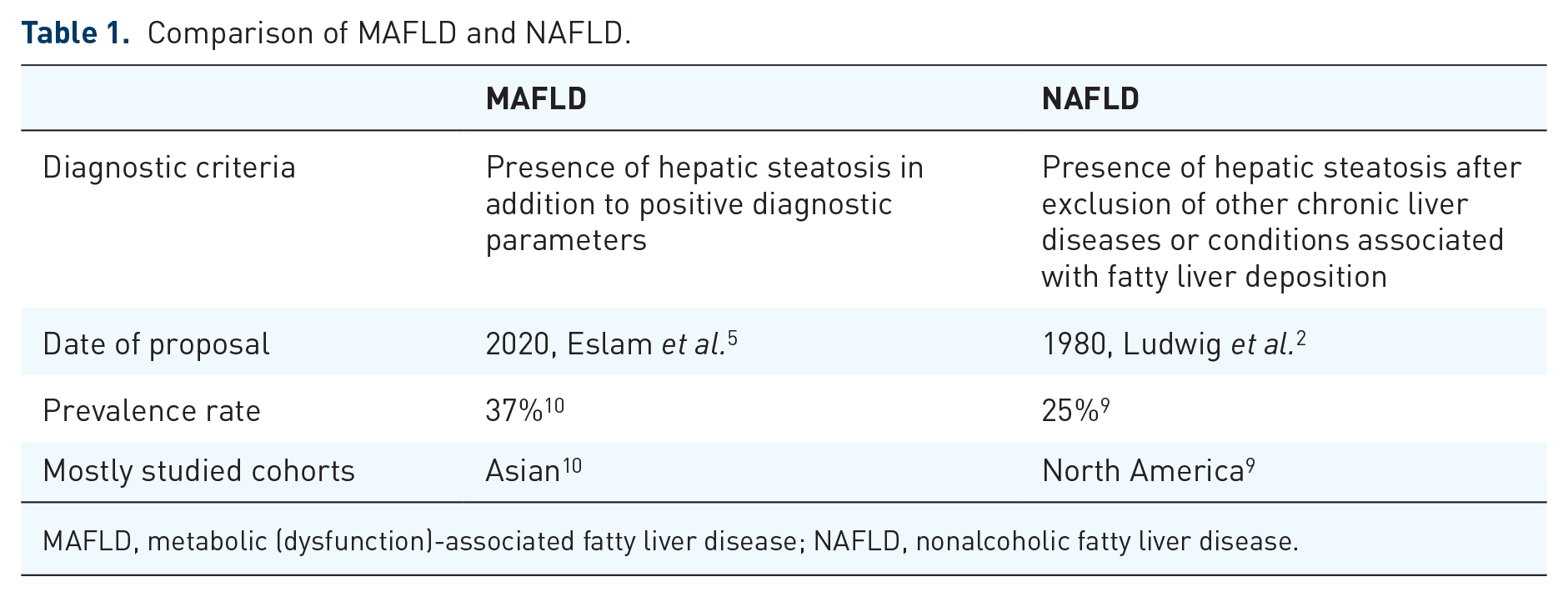
MAFLD, metabolic (dysfunction)-associated fatty liver disease; NAFLD, nonalcoholic fatty liver disease.
On analyzing the prevalence of MAFLD in overweight and obese individuals, Liu et al. 13 mainly focused on Asian individuals. They found that 50.7% of the overweight and obese study population (n = 2,667,052) met the diagnostic criteria for MAFLD. The pooled prevalence rates of type 2 diabetes mellitus (T2DM) and metabolic syndrome were 19.7% and 57.5%, respectively. 13
Lin et al. 14 compared the characteristics of MAFLD and NAFLD by analyzing data from Third National Health and Nutrition Examination Survey (NHANES-III) collected between 1988 and 1994. In all participants, hepatic steatosis was diagnosed by abdominal ultrasound, whereas fibrosis was staged with blood-based noninvasive tests – including the Fibrosis-4 Index (FIB-4), the NAFLD Fibrosis Score (NFS), and the body mass index, aspartate transaminase-to-alanine transaminase ratio, and diabetes (BARD) score. The authors found that MAFLD outperformed NAFLD in terms of risk stratification with respect to disease progression. 14 Interestingly, patients who met the criteria for MAFLD were older (48.79 ± 15.06 versus 46.81 ± 15.77 years, respectively, p < 0.001) and more commonly men [1959 (50.42%) versus 2014 (46.33%), respectively, p < 0.001] than those with NAFLD. In addition, the metabolic profile of patients with MAFLD was more severe with respect to body mass index (BMI) (31.14 ± 6.05 versus 29.49 ± 6.69 kg/m2, respectively, p < 0.001) and a higher prevalence of both T2DM [1171 (30.14%) versus 1092 (25.12%), respectively, p < 0.001] and hypertension [1405 (36.16%) versus 1343 (30.89%), respectively, p < 0.001]. 14 As for patient-related outcomes, nationwide data from the Fifth Korean National Health and Nutrition Examination Survey revealed that a diagnosis of MAFLD was associated with a two-fold increase in the extent of health-related quality of life impairment. 15 There is also evidence that MAFLD, but not NAFLD, may have an adverse impact on quality of life. 16
In another study that relied on NHANES-III data, 17 MAFLD was associated with a 17% increased risk of all-cause mortality [hazard ratio (HR): 1.17; 95% confidence interval (CI): 1.04−1.32], whereas NAFLD was not (HR: 1.05; 95% CI: 0.95–1.17). Interestingly, MAFLD – but not NAFLD – was an independent risk factor for overall mortality even after adjusting for metabolic risk factors. 17 This has been recently confirmed by Nguyen et al. 18 who found that the highest cumulative incidence of all-cause mortality (26.2%) occurred in patients who met the diagnostic criteria for MAFLD but not those of NAFLD. They were followed by patients who met the criteria for both NAFLD and MAFLD (21.1%) and those who met the diagnostic criteria for NAFLD but not those of MAFLD (10.6%; p < 0.001). Notably, patients who met the diagnostic criteria for MAFLD but not those of NAFLD had the highest FIB-4 values, which reflected a high risk of advanced fibrosis (8%), compared with the other two groups (1.3% and 1.9%, respectively). 18
The recent change in nomenclature has been endorsed by several different stakeholders. 19 Of note, the positive definition of MAFLD has reduced patient confusion on disease etiology, ultimately facilitating both awareness and patient-physician communication. 3 In addition, the new terminology has emerged as an important tool for reducing stigmatization caused by the association of NAFLD with alcohol consumption. 20 Using a 25-item survey, Fouad et al. 21 found that more than 90% of the participating physicians were unaware of NAFLD and tended to underestimate disease severity. However, 73% of the responders reported an increased awareness following the change in the acronym. 21 Similar findings were noted for other health care professionals, including nurses. 22
Current world data
Current knowledge concerning the prevalence of MAFLD is mainly informed by Asian studies. On examining 1016 Chinese patients using magnetic resonance imaging proton density fat fraction (MRI-PDFF), Wong et al. 23 reported that the prevalence rates of MAFLD and NAFLD were 25.9% and 25.7%, respectively. Interestingly, 89.2% of their study patients met the criteria for both conditions, 5.8% met the criteria for MAFLD but not those of NAFLD, and 5.1% met the criteria for NAFLD but not those of MAFLD. 23 Similar findings were reported in a cross-sectional study carried out in an urban population in southwest China. 24 On analyzing 139,170 subjects who underwent ultrasonography, 26.1% met the criteria for MAFLD. Interestingly, this condition was diagnosed in 11.5% of nonobese participants. The metabolic profile of nonobese individuals with MAFLD was less favorable than that of nonobese individuals who did not meet the criteria for MAFLD. 24 Huang et al. 25 reported that the prevalence of MAFLD was significantly higher (40.8%) in a Chinese cohort of government employees (n = 16,924) compared with the general population. This was attributed to dietary factors and a sedentary lifestyle. 25 In another study, Guan et al. 26 found a prevalence of MAFLD as high as 63.2% in a sample of 3553 Chinese individuals with T2DM. Only 48.2% of the study participants who met the criteria for MAFLD had a low risk of advanced fibrosis according to FIB-4 scores, suggesting that >50% of patients with MAFLD and T2DM may require a second-level work-up for assessing fibrosis stage. 26
In a nationwide study carried out in 6775 subjects in South Korea, Kim et al. 27 investigated the presence of hepatic steatosis and fibrosis by means of ultrasonography and magnetic resonance elastography, respectively. MAFLD was identified in 33.9% of the study participants, of whom 3% had advanced fibrosis. The majority of obese (79%) and diabetic (73.6%) subjects met the criteria for MAFLD. In addition, patients with a concomitant diagnosis of T2DM and MAFLD had a high rate (9.5%) of advanced fibrosis. 27
Fujii et al. 28 carried out a transient elastography study of 2254 patients who had undergone a health checkup. They reported that the prevalence rates of MAFLD and NAFLD were 35% and 27.4%, respectively, of whom 9% and 8%, respectively, had progressive liver disease. 28 In another Japanese cohort, Yamamura et al. 29 compared the prevalence of MAFLD and NAFLD in a cohort of 765 individuals with hepatic steatosis. The prevalence rates of the two conditions were 79.6% and 70.7%, respectively. Interestingly, patients with MAFLD had higher liver stiffness on transient elastography. 29
A similar prevalence of MAFLD has been reported in Iran. Taheri et al. 30 examined 4242 northeastern Iranian subjects aged between 35 and 70 years and investigated the prevalence of hepatic steatosis using the FLI. The prevalence of MAFLD was 22.8%, with the main risk factors being increased BMI, waist circumference, liver transaminases, and blood lipids. In addition, patients who slept less than 5 h per day showed a significantly higher risk of MAFLD [odds ratio (OR): 1.43; 95% CI: 1.07–1.92; p = 0.01]. 30
On analyzing a total of 909 patients, a multicenter study from Turkey reported that the prevalence of MAFLD was 45.5%. Notably, the enrolment involved patients with a history of dyspepsia but without known hepatic steatosis. The study cohort was therefore reflective of the general Turkish population. The prevalence rates of obesity, T2DM, metabolic syndrome, dyslipidemia, and hypertension in the study participants were 43.3%, 24.9%, 52.5%, 92.3%, and 31.9%, respectively. 31 In another Turkish study focusing on biopsy-proven MAFLD (n = 424), 16.5% of patients had evidence of advanced fibrosis – for which T2DM was the strongest predictor (OR: 2.495; 95% CI: 1.425–4.418). 32
Baratta et al. 33 investigated the overlap between MAFLD and NAFLD in an Italian cohort of 795 patients with NAFLD and found that the vast majority (96.5%) also met the criteria for MAFLD.
Currently, data from African countries remain limited. Van Dijk et al. 34 carried out a study using the Research on Obesity and Diabetes among African Migrants data set, which includes both individuals from the Ashanti Region in rural and urban Ghana and migrant Ghanaians living in European cities (n = 5282). The presence of hepatic steatosis was detected using FLI; unfortunately, the MAFLD diagnostic criteria were not applied. Elevated FLI values (>60) were found in 4.2%, 16.3%, and 28.9% of men as well as in 13.6%, 32.3%, and 36.6% of women living in rural Ghana, urban Ghana, and Europe, respectively (both p < 0.001). 34
In 2012, the Australian Diabetes, Obesity, and Lifestyle study included 4747 Australian adults aged between 34 and 97 years who were considered representative of the general population. 35 The authors found that 37% of the study participants met the criteria for MAFLD; among them, the BARD score ruled out advanced fibrosis in 38% of cases. The main independent risk factors for a diagnosis of MAFLD were advanced age, male sex, T2DM, lower high-density lipoprotein (HDL) cholesterol levels, a high diastolic blood pressure, and a sedentary lifestyle. 35 On analyzing an Australian regional cohort, Kemp et al. 36 reported that the prevalence rates of MAFLD and NAFLD were 47.2% and 38.7%, respectively. The observation that MAFLD was highly prevalent was attributed to a high occurrence of obesity and overweight (75.2%) in the study participants. 36
Finally, a study conducted in the general population of Mexico examined 585 volunteers who had undergone laboratory tests, liver ultrasound, transient elastography, and calculation of FIB-4 index. 37 The diagnostic criteria for MAFLD were met by 41% of the study participants. In addition, the prevalence of advanced fibrosis was as high as 40%, that is, markedly above that reported for the world’s general population. 37
Incidence
Published data concerning the incidence of MAFLD remain scarce and mainly limited to Asian countries. Wong et al. 23 examined the incidence of both MAFLD and NAFLD in a Chinese cohort consisting of 739 subjects without baseline evidence of fatty liver on MRI-PDFF. At follow-up, 13.8% of the study participants developed fatty liver – of whom 75.6% met the diagnostic criteria for MAFLD. The incidence rates of MAFLD and NAFLD were 2.8 per 100 person-years and 3.7 per 100 person-years, respectively. Compared with those who developed NAFLD, patients who met the diagnostic criteria for MAFLD at follow-up had a more severe baseline metabolic profile in terms of BMI, waist circumference, fasting blood glucose concentrations, and plasma lipid levels. 23 On examining a cohort of 30,633 Chinese subjects followed-up for a mean of 2.28 years, Yu et al. 38 reported that the incidence rates of MAFLD and NAFLD were as high as 41.58 per 1000 person-years and 37.69 per 1000 person-years, respectively. These findings were attributed to a high prevalence of the metabolic syndrome at baseline. 38 In another community-based Chinese cohort study, 6873 individuals were followed-up for approximately 5 years. 39 At follow-up, the incidence rates of NAFLD and MAFLD were 22.7% (95% CI: 21.3−24.0%) and 27.0% (95% CI: 25.5−28.4%), respectively. The predictive value of diabetes, cardiovascular disease, and chronic kidney disease for the development of MAFLD was similar. 39 On analyzing a Japanese cohort of subjects who had undergone a medical health checkup between 2004 and 2014, Hashimoto et al. 40 reported that the incidence of MAFLD after median follow-up of 4.6 (2.0–8.1) years was 31.1 per 1000 person-years. 40
Natural history
Patients with NAFLD show a stepwise increase in mortality rates according to the fibrosis stage; 41 therefore, the severity of hepatic fibrosis is currently recognized as the main prognostic determinant in this clinical entity. On analyzing 1773 adult patients with biopsy-proven NAFLD, Sanyal et al. 42 found that all-cause mortality was significantly associated with advanced fibrosis stages (0.32 deaths per 100 person-years for stage F0 to F2, 0.89 deaths per 100 person-years for stage F3, and 1.76 deaths per 100 person-years for stage F4). Interestingly, the majority of patients with advanced fibrosis and cirrhosis had evidence of concomitant nonalcoholic steatohepatitis (NASH). 42 Yang et al. 43 have recently examined the prevalence of fibrosis in a Chinese cohort of 246 patients with biopsy-proven NAFLD. They found that 74 (30.9%) of the 239 patients who met the criteria for MAFLD had significant fibrosis. 43 In a Turkish study that included 574 patients with biopsy-proven MAFLD, the overall prevalence of significant fibrosis was 39.3%. Specifically, the following distribution was observed: F1, n = 172 (30.7%); F2, n = 109 (19.5%); F3, n = 86 (15.4%), and F4, n = 25 (4.5%). 44
MAFLD is a multisystemic disease in which a wide variety of extra-hepatic manifestations – including cardiovascular disease, chronic kidney disease, and extrahepatic malignancies – can occur. In addition, epidemiological evidence for a possible comorbidity between NAFLD and an impaired cognitive function has been reported. 45 Adverse cardiovascular events represent the leading cause of death in patients with MAFLD, followed by extra-hepatic malignancies and liver-related complications. 46 The MAFLD definition seems to outperform NAFLD in terms of identifying patients at high risk of extra-hepatic manifestations. For example, the NHANES-III (1988−1994) study revealed that MAFLD identified chronic kidney disease (CKD) in 29.60% of the participants compared with 26.56% when the traditional NAFLD criteria were used. 47 On analyzing an independent cohort of 27,371 subjects, Hashimoto et al. 40 was able to replicate these findings. Specifically, the adjusted ORs for CKD in patients with MAFLD versus those with fatty liver in the absence of metabolic disturbances were 1.83 (95% CI: 1.66−2.01) and 1.02 (95% CI: 0.79−1.33), respectively. 40 There is also evidence to support the predictive ability of the MAFLD definition for the development of CKD. 48
The association between both MAFLD and NAFLD with adverse cardiovascular outcomes is well established.39,49 In a large nationwide study, Lee et al. 50 examined 9,584,399 subjects included in a health care screening data set. After the exclusion of 8,962,813 participants with a known history of cardiovascular disease at baseline, they found that both MAFLD and NAFLD were associated with an increased risk of developing cardiovascular disease at follow-up; however, the HR was significantly higher for the former definition (1.43; 95% CI: 1.41−1.45) compared with the latter (1.09; 95% CI: 1.03−1.15). 50 In line with these findings, another study that included patients with biopsy-proven MAFLD and NAFLD reported a higher occurrence of cardiovascular disease at follow-up in the former compared with the latter (36.4 versus 25.7%, respectively). 51 The authors also found that a concomitant diagnosis of viral hepatitis significantly increased cardiovascular risk in patients diagnosed with MAFLD. 51
There is also evidence indicating that the extent of lung impairment is higher in MAFLD than in NAFLD. On analyzing 2543 middle-aged individuals recruited from 25 communities across four cities in China, Miao et al. 52 found that patients with MAFLD were characterized by significantly lower forced vital capacity (88.27 ± 17.60% versus 90.82 ± 16.85%, p < 0.05) and one second forced expiratory volume (79.89 ± 17.34 versus 83.02 ± 16.66%, p < 0.05) than those with NAFLD.
Finally, colorectal malignancies are prevalent in patients with MAFLD. 53 Interestingly, their burden has been associated with the severity of both MAFLD and NAFLD. 54 In a multicenter retrospective study, Fukunaga et al. 55 found that patients with nonobese MAFLD were at an increased risk for colorectal adenoma, whereas those with nonobese NAFLD were not.
Diagnosis
Figure 1 depicts the current diagnostic algorithm for MAFLD. 5 In general, the diagnostic process relies on the detection of hepatic steatosis using noninvasive blood tests, imaging modalities, or liver histology. According to the Asian Pacific Association for the Study of the Liver, 56 screening of MAFLD with abdominal ultrasonography is recommended for patients with overweight/obesity, T2DM, and metabolic syndrome. However, the diagnosis of hepatic steatosis can be incidental. The detection and staging of liver fibrosis is also paramount for risk stratification. In the next sections, we will discuss the current diagnostic options for detecting MAFLD.

Diagnostic workflow for MAFLD.
Noninvasive blood tests
FLI is a common diagnostic algorithm for hepatic steatosis that includes BMI, waist circumference, triglycerides, and gamma-glutamyl transferase. An FLI < 30 can confidently rule out the presence of fatty liver, whereas an FLI > 60 denotes a high probability of steatosis. 57 Other less commonly used algorithms include the hepatic steatosis index, 58 SteatoTest, 59 lipid accumulation product, 60 NASH index, 61 NAFLD liver fat score, 62 triglyceride-glucose index, 63 serum keratin-18 fragments, 64 and the visceral adiposity index. 65 The utility of FLI for MAFLD screening has been recently validated in the NHANES III population where hepatic steatosis was identified by ultrasonography. 66 The results revealed a satisfactory performance of FLI (area under curve = 0.793; negative predictive value = 77%) in the detection of MAFLD. 66
As for the noninvasive screening of hepatic fibrosis, several blood-based panels have been proposed. The American Association for the Study of Liver Diseases and the European Association for the Study of the Liver recommended the use of the FIB-4 and the NFS for the screening of advanced fibrosis in patients with NAFLD.1,67 More recently, the Asian Pacific Association for the Study of the Liver maintained the same approach for MAFLD. 57 Other panels – including the alanine transaminase-to-platelet ratio index (APRI) and BARD – have been widely used for the screening of significant and advanced fibrosis.68,69 It is generally accepted that FIB-4 and NFS are superior to APRI and BARD in both MAFLD and NAFLD populations.70–73 On analyzing a cohort of 417 patients with biopsy-proven MAFLD, Wu et al. 70 reported that FIB-4 was characterized by the highest area under curve (0.736; 95% CI: 0.691−0.778) followed by NFS (0.724; 95% CI: 0.679−0.767), APRI (0.671; 95% CI: 0.623−0.715), and BARD (0.609; 95% CI: 0.560−0.656).
Although the use of FIB-4 and NFS should be preferred over other panels for the screening of advanced fibrosis, their application in patients with MAFLD is not without limitations. First, their main clinical utility lies in their ability to exclude – rather than identify – advanced fibrosis. 74 Second, age may significantly affect the diagnostic accuracy of both FIB-4 and NFS. In this regard, McPherson et al. 75 found that FIB-4 and NFS may underperform in patients aged less than 35 years; in addition, age-specific cut-offs (<2 for FIB-4 instead <1.3 and <0.12 for NFS instead <–1.455) have been proposed to reduce false-positive findings in elderly patients (>65 years). 75 Third, the performances of FIB-4 and NFS may be affected by BMI values. Using the diagnostic criteria for MAFLD, we have previously shown that FIB-4 and NFS do not perform adequately in both lean and morbidly obese patients. 44 However, no confounding effect of abnormal transaminase levels or T2DM has been reported.76–79
Several more complex panels – including the enhanced liver fibrosis test (ELF), FibroMeter, FibroTest, and ADAPT (age, presence of diabetes, procollagen C3, and platelet count) – have been recently proposed for the detection of hepatic fibrosis.80–82 Of them, ADAPT has been validated according to the MAFLD diagnostic criteria and was found to outperform FIB-4, NFS, APRI, and BARD. 83 The stepwise use of ADAPT followed by liver stiffness measurement (LSM) with transient elastography resulted in a negative predictive value close to 100%. 83 Therefore, this diagnostic algorithm holds promise to reduce the number of liver biopsies. Similarly, it has been recently reported that the combined used of FIB-4 and ELF may result in 85% reduction of referrals to tertiary care centers. 84
Imaging modalities
Owing to its noninvasive nature, widespread availability, and low costs, abdominal ultrasonography remains the most extensively used imaging modality for the identification of hepatic steatosis. 85 However, its clinical usefulness for the detection of mild-to-moderate steatosis (<30%) is limited, and more sensitive methods – including controlled attenuation parameter (CAP) obtained from transient elastography86,87 – have been developed. Notably, the determination of CAP in obese individuals is feasible but requires the use of a specific XL probe.88,89 Currently, MRI-PDFF remains the reference standard for quantification of liver fat using imaging modalities; therefore, it has been extensively used as an endpoint in clinical trials. 90
As for the imaging detection of hepatic fibrosis, the use of LSM obtained from transient elastography is gaining momentum.91,92 Currently, FibroScan is recommended as a second-level diagnostic modality93,94 for patients deemed at indeterminate or high risk of advanced fibrosis based on FIB-4 scores (i.e. values ⩾1.3).95,96 A feasible diagnostic workflow for hepatic fibrosis is presented in Figure 2. Finally, magnetic resonance elastography is a highly accurate imaging modality for the assessment of liver fibrosis. Unfortunately, its high costs and poor availability have significantly limited its routine clinical use. 97

Diagnostic workflow for hepatic fibrosis in MAFLD.
Liver biopsy
In light of the continuous nature of hepatic inflammation, the definition of MAFLD avoids the traditional dichotomous classification of NASH versus non-NASH. In this scenario, disease activity and fibrosis are considered the main prognostic drivers. 56 Although liver biopsy is still considered the reference standard for achieving a final diagnosis, its use should be carefully weighed in light of its procedural risks, invasive nature, and possible sampling errors. 98 In general, it is recommended to obtain a biopsy in all patients who undergo bariatric surgery or in presence of conflicting results on noninvasive tests. Moreover, liver biopsy is mandatory in presence of diagnostic uncertainties (e.g. dual etiology) or inclusion in clinical trials. 56
Conclusion
The recent rebranding of NAFLD to MAFLD has prompted research efforts to compare the two conditions with respect to a number of aspects. While large overlaps exist between the MAFLD and NAFLD populations, it is clear that the two terms do not denote the same clinical entity. In addition, although the diagnostic modalities remain similar, the two acronyms should not be used interchangeably. Notably, growing evidence indicates that patients with MAFLD tend to have less favorable outcomes than those with NAFLD.