
Abstract
Background:
In the context of the COVID-19 pandemic, there is growing concern about the virus’s effects on individuals with existing endocrine disorders such as primary aldosteronism (PA).
Objectives:
This study explores the potential relationship between PA and the risk of developing obstructive sleep apnea (OSA) after a COVID-19 infection.
Design:
In this retrospective cohort study, we utilized data from the TriNetX database, covering the period from January 2019 to January 2023. We identified essential hypertension (EH) patients as the control group, employing 1:1 propensity score matching.
Methods:
The endpoints included incident OSA and all-cause mortality.
Results:
Among 11,422,001 patients with PCR-positive COVID-19, we identified 3628 PA patients (mean 63.1 years, male 38.1%). After a median follow-up of 1.9 years, the rate of OSA was 28.9 per 1000 person-years in PA patients compared to EH with 16.7. We showed a significant increase in incident OSA (adjusted hazard ratio (aHR) 1.58, p < 0.001) and mortality (aHR 1.12, p = 0.04) in PA patients than EH post-COVID-19. The horizon plot revealed that patients with pre-existing PA had the highest risk of OSA at 2 months (aHR = 2.34) post-COVID-19. In subgroup analysis, PA patients with a high body mass index (⩾30 kg/m2; aHR 1.81, p = 0.001) or preserved kidney function (aHR 2.00, p < 0.001) had increased OSA incidences post-COVID-19.
Conclusion:
Our study underscores a notable rise in incident OSA among PA patients post-COVID-19, highlighting the imperative for diligent OSA screening, particularly among individuals with obesity or preserved kidney function.

Keywords
Introduction
Primary aldosteronism (PA), linked to the Renin-Angiotensin-Aldosterone System (RAAS) and marked by excessive aldosterone, raises hypertension and cardiovascular risks. 1 The COVID-19 pandemic highlights the interaction between SARS-CoV-2 and RAAS, especially in PA patients, with angiotensin-converting enzyme 2 (ACE2) playing a key role in the virus’s entry and infection pathophysiology. 2
Obstructive sleep apnea (OSA) is commonly undiagnosed despite its prevalence, characterized by the repeated collapse of the upper airway during sleep, leading to disrupted sleep patterns and variable oxygen saturation. 3 OSA extends its effects beyond mere drowsiness, potentially triggering various endocrine disorders. 4 It is notably more prevalent among those with conditions such as obesity, hypothyroidism, acromegaly, Cushing’s syndrome, diabetes, systemic infection disease, and PA. 5
Objectives
Emerging studies have identified OSA as an independent risk factor for severe COVID-19 outcomes.6–10 A small-scale study has also indicated a high incidence of OSA in COVID-19 patients with moderate-to-severe acute respiratory distress syndrome post-hospital discharge. 11 Despite this, there was a causal effect of severe COVID-19 on an increased risk of OSA. 12 Our research addresses this knowledge gap by investigating the potential link between PA and heightened susceptibility to OSA after COVID-19.
Design
This was a retrospective cohort study based on electronic health records extracted from the TriNetX US Network database. The analysis covered data from 42 million individuals in the TriNetX US Network, spanning January 2019 to January 2023, 13 using the TriNetX database to aggregate electronic medical data from 84 Healthcare Organizations.13–15 This study followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guideline for cohort studies (Supplemental File). The index date for these patients was set as the date of their positive PCR test for COVID-19. Among them, a validated algorithm was employed to identify patients with PA (10th International Classification of Diseases (ICD-10) code: E26.0), with recruitment limited to individuals aged ⩾18 years old (Supplemental Table 1). Consequently, we exclusively enrolled patients diagnosed with PA who had a documented history of mineralocorticoid receptor antagonist (MRA) usage at the index time, falling within the ATC class C03D, RXNORM:9997/298869, VA Class Code: CV704. This stringent criterion was established in alignment with our principal study objective, which sought to establish a robust and reliable sample representative of PA.13,16 In the PA group, we excluded patients with adrenal gland resection, secondary hyperaldosteronism, Bartter’s syndrome, and prior OSA diagnosis.
The control group included hypertensive patients who were identified through their use of antihypertensive medications but had no diagnosis of PA, secondary hypertension, or Gitelman syndrome (Supplemental Table 2). Both groups were meticulously matched for age, sex, and the presence of comorbidities, as well as the use of specific medications (Supplemental Table 3). We used propensity score matching (PSM) at a 1:1 ratio for similar baseline characteristics, using the built-in functions within the TriNetX platform with a caliper of 0.1 standard deviation. The matching considered age, sex, race, comorbidities, medication use, and laboratory data.
Methods
For the primary outcome, we identified patients with new OSA diagnoses post-COVID-19 by checking for OSA-specific ICD-10-CM codes, recorded at any time upmost to the 2-year period following the index date. The secondary outcome was mortality, and the composite outcome was defined as incident OSA as well as all-cause mortality (Supplemental Table 4).
Adjusted hazard ratios (aHRs) were calculated using Cox proportional hazard models to evaluate the outcomes of interest and assess proportionality. The generalized Schoenfeld approach within the TriNetX network tested for proportional hazard assumptions, with robust standard errors employed to account for interdependence among matched users. Kaplan–Meier methods calculated survival probabilities. Where proportional hazard assumptions were not met, aHRs were computed for distinct time intervals. E-values were calculated according to VanderWeele and Ding’s methodology. 17 Analyses included specificity and outcome controls, both positive and negative. A two-sided p-value <0.05 and a 95% confidence interval (CI) were used to determine statistical significance.
Results
From January 1, 2019, to January 1, 2023, we found 11,422,001 individuals who received SARS-CoV-2 PCR tests in the TriNetX Network. From this population, 38,279 were diagnosed with PA, while a control group consisted of 11,383,722 individuals (Figure 1). After excluding patients with other adrenal gland disorders and previous OSA diagnoses, we included PA patients (N = 3628, male: 38.1%, mean age: 63.1 years) and non-PA hypertensive patients (N = 972,590, male: 43.9%, mean age: 59 years) in the study.

Enrollment algorithm for PA and EH patients.
After PSM, there were 3628 patients with PA (mean age 63.1 years, 38.1% men) and 3628 hypertensive patients (mean age 63.4 years, 37.6% men) as controls (Table 1). The crude incidence of OSA rate was 28.9 per 1000 person-years, which was significantly higher than in the essential hypertension (EH) group (16.67 per 1000 person-years). The overall cohort had a mean duration of 1.9 years and a median of 0.98 years (IQR, 0.48–1.49), with the 90th percentile being 1.8 years. However, a notably higher risk of developing incident OSA was observed in the PA group (aHR 1.58, 95% CI: 1.25, 1.97, p < 0.001). Additionally, there was a significantly increased risk of mortality (aHR 1.12, 95% CI: 1.01, 1.25, p = 0.040), and risk of both mortality or OSA (aHR 1.21, 95% CI: 1.10, 1.34, p < 0.001; Figures 2 and 3).
Comparative demographic and clinical characteristics of COVID-19 patients with or without PA.

Matching item.
Do not match because of baseline characteristics.
COPD, chronic obstructive pulmonary disease; eGFR, estimated glomerular filtration rate; PA, primary aldosteronism.

aHRs for outcomes and exposures in PA and EH patients post-COVID-19. The forest plot displays the aHR with their 95% CI for a range of outcomes, controls, and exposures. Each blue square on the plot corresponds to the point estimate of the aHR, while the horizontal lines that intersect the squares represent the 95% CIs for these estimates. The analysis reveals a significant association between OSA and an increased aHR of 1.56 (p < 0.001). Isolated mortality presents an aHR of 1.12 (p = 0.040) and when assessing a composite outcome of OSA and mortality, the aHR is 1.21 (p < 0.001).

Kaplan–Meier curves of main outcome. The Kaplan–Meier curves depicting the cumulative incidence of outcomes across a span of 2 years. The left graph, focusing on the incidence of OSA (p < 0.001), and the right graph on the composite outcome including OSA and mortality (p < 0.001). Patients with PA, shown by the blue line, and the counterpart of EH, depicted by the red line. As time progresses, the divergence of the curves indicates that the PA cohort has a higher likelihood of developing OSA. The 95% confidence intervals are illustrated by the shaded regions surrounding the curves, reflecting the data’s variance.
The E-value for the outcome of all-cause mortality was calculated at 1.24. For the composite outcome of OSA or mortality, the E-value increased to 1.48 (Supplemental Table 5).
Specificity analysis
In the context of positive outcomes serving as controls, specifically hypokalemia, a significant association was observed among PA patients (aHR 1.35, 95% CI: 1.26, 1.45, p < 0.001). Conversely, concerning negative outcomes as controls, no significant differences were noted between PA patients and control groups regarding the risks of traffic accidents (aHR 1.02, 95% CI: 0.80, 1.30, p = 0.864), herniation (aHR 1.42, 95% CI: 0.75, 2.69, p = 0.277), or otitis media (aHR 0.8, 95% CI: 0.45, 1.44, p = 0.457). Furthermore, our analysis extended to examining the effects of positive and negative exposures. For positive exposure, we focused on patients with a body mass index (BMI) of 30 kg/m2 or above (N = 1,052,884), which was considered a risk factor for OSA. This group showed a significantly higher aHR of 2.79 (95% CI: 2.74, 2.83, p < 0.001).
Under the assumption that individuals with PA following influenza infection would not experience an increased risk of developing OSA, we conducted a comparative analysis between PA patients (n = 2346) and those with EH (n = 448,265) who concurrently contracted influenza during the same study period. Our investigation revealed no statistically significant association (aHR, 1.08; 95% CI: 0.82, 1.41, p = 0.583).
To substantiate the assertion that the heightened incidence of OSA is directly consequent to COVID-19, we performed a landmark analysis at disparate time intervals post-diagnosis. An analysis of the aHR depicted as a horizon plot post-discharge unveiled that patients with preexisting PA with current COVID-19 exhibited the highest risk of critical outcomes at 2 months (aHR = 2.34). Subsequent to this timeframe, there was a gradual decrease in the aHR.
Sensitivity analysis
We investigated the relationship between a variety of patient characteristics and the prevalence of OSA (Figure 4). Significant disparities in the risk of OSA were noted across various subgroups, including sex, age, diabetes mellitus, and several other factors. Notably, PA individuals with a BMI below 25 kg/m2 (aHR 0.80, 95% CI: 0.40, 1.61, p = 0.525) and those with a BMI ranging from 25 to 29 kg/m2 (aHR 0.98, 95% CI: 0.55, 1.73, p = 0.932) did not present a statistically significant risk for developing OSA after COVID-19.
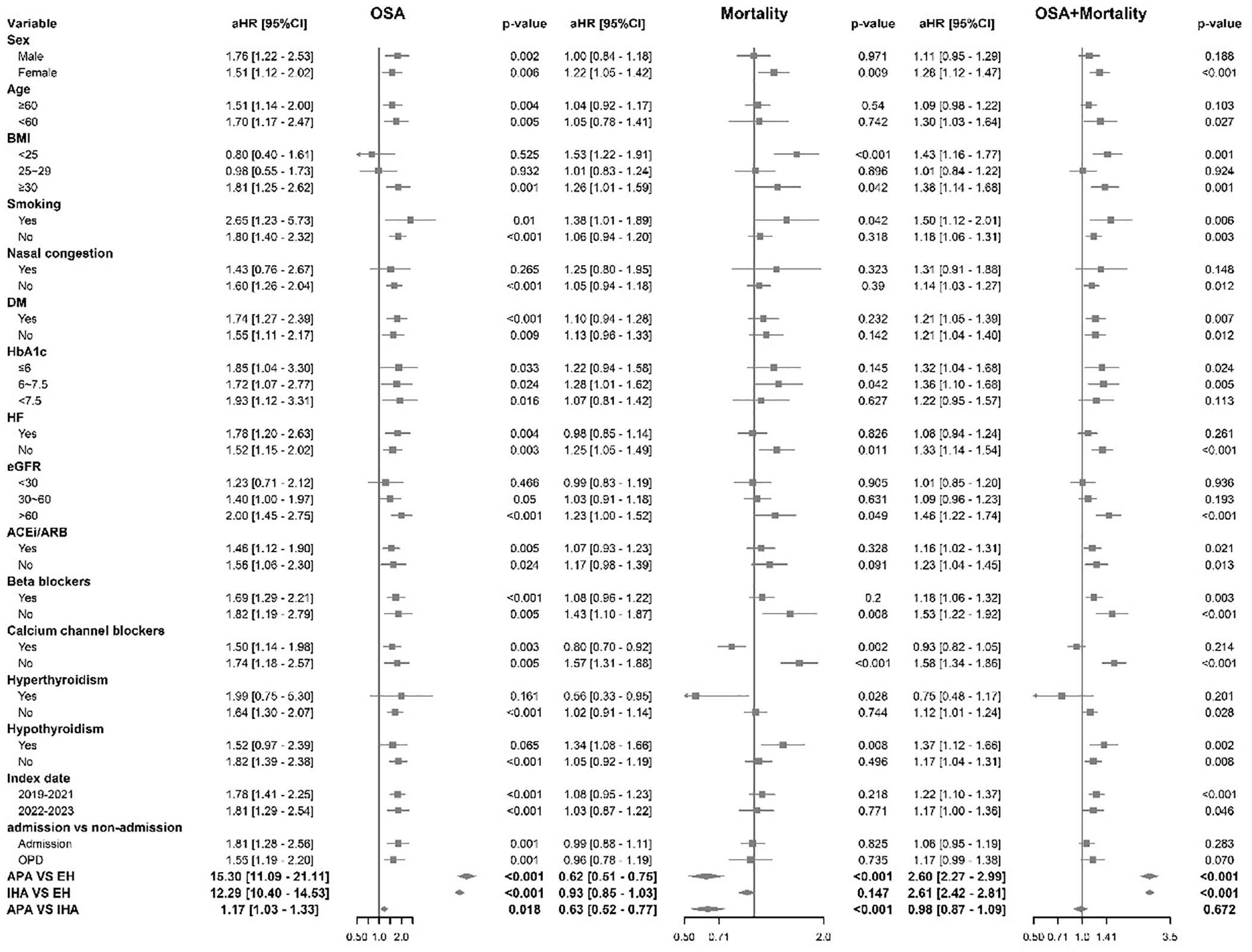
Subgroup analysis forest plot for the possibility of OSA. This forest plot graphically represents the results of a subgroup analysis assessing the aHR for the composite outcome of OSA prevalence and mortality rates with different clinical characteristics.
Among patients with PA, those without nasal congestion exhibited an aHR for developing OSA of 1.60 (95% CI: 1.26, 2.04, p < 0.001). Conversely, for those with hyperthyroidism, the aHR was 1.64 (95% CI: 1.30, 2.07, p < 0.001), and among PA patients without hypothyroidism, the aHR was 1.82 (95% CI: 1.39, 2.38, p < 0.001). Among those with preserved kidney function (estimated glomerular filtration rate (eGFR) above 60 mL/min/1.73 m2), the aHR was 2.00 (95% CI: 1.45, 2.75, p < 0.001). Additionally, we observed a disease severity-dependent risk of OSA after COVID-19, with a higher hazard ratio for in-hospital admission (aHR = 1.81) compared to non-admission (aHR = 1.55).
In subgroup analysis, patients with aldosterone-producing adenoma (APA) demonstrated a substantially increased risk of developing OSA with an aHR of 15.30 (95% CI: 11.09, 21.15, p < 0.001). Similarly, individuals with idiopathic hyperaldosteronism (IHA) exhibited a significantly increased risk of OSA, with an aHR of 12.29 (95% CI: 10.40, 14.53, p < 0.001). These aHRs were notably higher with APA patients displaying a greater risk than those with IHA (aHR 1.17, 95% CI: 1.03, 1.33, p = 0.02).
Discussion
In the largest international dataset on post-COVID-19 conditions, we observed an incidence rate of 28.9 per 1000 person-years for OSA among patients with PA, exceeding that of patients with EH with 16.7 per 1000 person-years, and surpassing the general population rate of 1.70 per 1000 person-years. 18 Notably, this risk remains consistent across different timeframes and subgroups of PA, particularly elevated in patients with preserved kidney function or obesity, underscoring the unique susceptibilities of this patient cohort in the ongoing aftermath of the pandemic. Furthermore, these patients also experienced a higher incidence of OSA that persisted for over 2 months.
The relatively low number of PA patients in our cohort is primarily due to two key exclusion criteria. First, we excluded individuals with a prior diagnosis of OSA, a condition known to be highly prevalent among PA patients. Second, we also excluded those who had undergone adrenalectomy, as surgical treatment may reduce the risk of OSA and alter the patient’s cardiometabolic profile. These exclusions likely removed a substantial portion of PA cases. However, they also allowed us to more precisely isolate a medically managed PA population at risk for incident OSA after COVID-19, reducing potential confounding and enhancing the validity of our findings.
In our study, we observed a higher proportion of women and an older average age among patients with PA. This may be explained by our study design. We excluded patients with a prior diagnosis of OSA, which is more common in men, possibly leading to a relative increase in female participants. In addition, we excluded patients who had undergone adrenalectomy, a treatment more commonly performed in younger or healthier individuals. As a result, our cohort included more older patients who remained on medical therapy.
The relationship between OSA and COVID-19
OSA independently increases the risk for severe COVID-19, even after adjusting for obesity and comorbidities.6–10 Systemic inflammation and hypoxemia are key pathophysiological links between OSA and COVID-19, with the repeated cycles of hypoxia and reoxygenation in OSA potentially worsening cytokine storms in COVID-19 patients. 19 Six months after COVID-19 infection, approximately 34% of patients require supplemental oxygen, and 2.6% need ventilatory support. Additionally, persistent shortness of breath is reported in 14.5% of cases. 20
However, comparatively, the topic of COVID-19-induced OSA has received minimal attention. A small group study highlights a potential causal effect wherein severe COVID-19 might increase the risk of developing OSA. 12 Our study indicates that COVID-19 further escalates the risk of OSA, especially in those ever admitted. Building upon this premise, our study findings indicate that even mild symptoms in patients with a positive COVID-19 PCR test are associated with an increased risk of OSA. This suggests that the respiratory complications associated with COVID-19 might contribute to the onset or exacerbation of OSA. 21
The relationship between OSA and PA
Several studies have indicated that OSA occurs more frequently in patients with PA than in those without.22–27 Several studies have indicated that OSA is more prevalent in patients with PA compared to those without. In our cohort, we observed a 23% incidence of OSA within 2 years following COVID-19 infection in PA patients, which is notably higher than the 18% prevalence reported in previous studies of PA. 27 This suggests that the physiological impact of COVID-19 may further elevate the risk of OSA in this already vulnerable population. Given the clinical consequences of untreated OSA, these findings underscore the importance of heightened awareness and routine screening for OSA among patients with PA, especially in the post-COVID-19 setting. We analyzed OSA’s incidence from 1 month to 3 years post-COVID-19 to determine its link to the virus. The highest aHR was observed at 2 months post-infection, indicating a significant impact shortly after. Therefore, follow-up in such patients should extend for at least 2 months (see Supplemental Figure 1).
Aldosterone, crucial for blood pressure regulation, has been found to aggravate OSA. 28 In addition, OSA can trigger the RAAS, and this interaction between OSA and aldosterone exacerbates hypertension in patients with OSA who have resistant hypertension. 23
In our study, the potential link between PA and OSA has the same shared risk factor of obesity, as indicated in previous research. 24 Furthermore, PA often results in fluid being displaced from the lower limbs to the neck structures. 28 This fluid shift can cause soft tissue edema, subsequently increasing upper airway resistance and leading to airflow obstruction, which further contributes to the development of OSA. In patients with preserved kidney function, the renal response to aldosterone may be more efficient, thereby enhancing fluid retention and amplifying the risk of OSA in this subgroup.
The relationship between COVID-19, OSA, and PA
We found that PA patients had a higher OSA incidence post-COVID-19. ACE2’s role in RAAS and as SARS-CoV-2’s receptor explains this trend. 29 PA patients show higher ACE2 and TMPRSS2 levels than the normotensive group. 2 SARS-CoV-2 infects humans through ACE2, potentially activating the RAAS, which in turn affects the production of Angiotensin II and aldosterone, 30 thereby exacerbating the mechanism leading to the development of OSA in PA patients. Studies, including the HYPNOS study, reveal a significant association between elevated plasma aldosterone levels and a diagnosis of moderate-to-severe OSA in white patients, 23 and other research highlights the link between elevated levels of Angiotensin II, and aldosterone. 31 The increased ACE plasma activity noted in patients with untreated OSA further substantiates this connection. 32
Subgroup analysis
Our findings highlight a strong link between OSA and PA in patients with a BMI over 30 kg/m2, similar to previous studies. 33 Our subgroup analysis revealed that patients with preserved kidney function, as indicated by a higher eGFR, might be more vulnerable to the impacts of long-term SARS-CoV-2 syndrome. 34
We also investigated the effects of varying HbA1c levels in diabetic patients and discovered significant differences across all groups, indicating that the likelihood of PA patients developing OSA after a COVID-19 infection is not influenced by the degree of variable blood sugar control.
Compared to earlier research suggesting severe COVID-19 may raise OSA risk, 12 we classified patients based on their condition’s severity into hospital admissions and outpatient follow-ups. Our analysis revealed significant differences in both groups, with aHR of 1.81 and 1.55. Furthermore, given the varying severity of the COVID-19 pandemic over time, we analyzed data from two periods, 2019–2021 and 2022–2023. Our findings showed significant differences in both intervals, with aHR of 1.78 and 1.81, respectively, indicating a consistent association across different waves of the pandemic. These results suggest that in individuals with PA, the severity of COVID-19 does not affect the likelihood of developing OSA.
We also observed that patients with APA have a higher risk of developing OSA following COVID-19 infection than those with IHA. The pronounced elevated aldosterone levels, hypertension condition, and fluid imbalance seen in APA compared to IHA could play a significant role in the risk and severity of OSA.
Study limitations
This study has several limitations. First, the retrospective design may introduce inherent biases. In addition, a formal sample size calculation was not performed due to the use of a real-world, population-based database. As such, the analysis was based on all eligible cases identified during the study period, rather than on a predetermined statistical power. Second, classifying diseases based on diagnostic codes might underrepresent mild or undocumented conditions, leading to ascertainment bias. However, we sought to mitigate the impact of unknown confounders by analyzing medication usage as a proxy. Its robustness is underscored by the utilization of sophisticated statistical methodologies, including PSM and E-value calculations, which augment the reliability and validity of the findings. A higher E-value, surpassing our aHR, indicates that only a limited unmeasured confounding variable would be needed to neutralize the estimated effect of the covariates, thus increasing the probability of a causal relationship. Third, although our methodology was rigorous, there is still a risk of misclassification bias and residual confounding. Factors not measured or unknown may be linked to the risk of adverse outcomes, thus introducing potential confounding elements. Nevertheless, we systematically employed a diverse array of methodological strategies, including the implementation of variable positive and negative controls, aimed at attenuating the influence of latent confounders and securing robust and consistent outcomes. Importantly, our study revealed that concurrent influenza infections did not elevate the risk of OSA among patients with PA. This suggests that other forms of recall bias are likely, but not substantial factors in our findings.
Another limitation of our study lies in the definition of the EH control group. We defined EH based on the documented use of antihypertensive medications together with the ICD code. This approach was intended to ensure that included controls had clinically significant hypertension requiring pharmacologic treatment. However, we acknowledge that some antihypertensive agents may also be prescribed for non-hypertensive indications, such as proteinuria control in nephrotic syndrome or the management of heart failure. Because the TriNetX database does not provide consistent information on medication indication, some degree of misclassification is possible. This methodological constraint is inherent to the use of real-world data and should be considered when interpreting the findings.
Conclusion
During an average follow-up of 1.9 years, we identified a 28.9 per 1000 person-years incidence of OSA in PA patients post-COVID-19, which is higher than in EH patients, particularly among those with obesity or preserved kidney function.
Supplemental Material
sj-docx-1-taj-10.1177_20406223251351779 – Supplemental material for Incident obstructive sleep apnea in patients with primary aldosteronism following COVID-19 infection: a health global federated network analysis
Supplemental material, sj-docx-1-taj-10.1177_20406223251351779 for Incident obstructive sleep apnea in patients with primary aldosteronism following COVID-19 infection: a health global federated network analysis by Wen-Kai Chu, Chih-Cheng Lai, Tai-Shuan Lai, Yen-Hung Lin and Vin-Cent Wu in Therapeutic Advances in Chronic Disease
Supplemental Material
sj-docx-2-taj-10.1177_20406223251351779 – Supplemental material for Incident obstructive sleep apnea in patients with primary aldosteronism following COVID-19 infection: a health global federated network analysis
Supplemental material, sj-docx-2-taj-10.1177_20406223251351779 for Incident obstructive sleep apnea in patients with primary aldosteronism following COVID-19 infection: a health global federated network analysis by Wen-Kai Chu, Chih-Cheng Lai, Tai-Shuan Lai, Yen-Hung Lin and Vin-Cent Wu in Therapeutic Advances in Chronic Disease
Footnotes
Acknowledgements
None.
Declarations
Supplemental material
Supplemental material for this article is available online.
Declaration of generative AI in scientific writing
During the preparation of this work, the authors used OpenAI’s ChatGPT to assist in improving the readability and language of the manuscript. All content generated was carefully reviewed and edited by the authors, who take full responsibility for the final content of the publication.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.