
Abstract
Background:
Patients with obstructive sleep apnea (OSA) may be at high risk for atrial fibrillation (AF), but data on the benefits of early AF screening in this population, including the prevalence of AF detected through such screening, remain limited.
Objectives:
This study evaluates the prevalence of AF in OSA patients using three screening methods and aims to identify the most effective approach, as well as the potential benefits of early AF detection in this population.
Design:
Prospective, single-center, cross-sectional study.
Methods:
This study assessed AF prevalence using three screening methods: opportunistic screening via pulse taking during a routine visit, systematic screening with a handheld electrocardiogram (EKG), and EKG during polysomnography. The analysis also included the proportion of patients with positive screenings who were indicated for anticoagulation and the prevalence of other non-AF arrhythmias.
Results:
A total of 201 OSA patients were enrolled, with a mean age of 46 years and a mean CHA2DS2-VASc score of 1. The prevalence of AF was 1.5%, 2.5%, and 2.0% when detected by pulse taking, handheld EKG, and EKG during polysomnography, respectively, with no statistically significant difference (p = 0.933). All patients with positive screenings were indicated for oral anticoagulant therapy. The prevalence of other non-AF arrhythmias was higher than in the general population, and detecting arrhythmias during sleep appeared to be more effective than detecting them while awake, particularly for atrial tachycardia.
Conclusion:
The prevalence of AF in OSA patients ranged from 1.5% to 2.5%, with the highest rate observed in handheld EKG systematic screening, though the difference was not statistically significant. Non-AF arrhythmias were also more common than in the general population, highlighting the need for broader arrhythmia surveillance. Further large-scale studies in higher-risk OSA populations are needed to confirm the benefits of systematic AF screening.
Plain language summary
People with obstructive sleep apnea (OSA), a condition in which the airway repeatedly becomes blocked during sleep—causing breathing to stop and start, poor sleep quality, loud snoring, and daytime tiredness—may have a higher risk of developing an irregular heartbeat called atrial fibrillation (AF), a common heart rhythm disorder that can lead to stroke. But it’s still not clear if checking for AF early in people with OSA is helpful. In this study, 201 people with OSA were tested to see how many had AF and which method worked best to find it. The three ways of checking were:
1. Feeling the pulse during a doctor visit
2. Using a small heart monitor at home for 2 weeks
3. Monitoring the heart during a sleep study
Most people in the study were about 46 years old and had low stroke risk. AF was found in 1.5% to 2.5% of people, depending on the method. The home monitor found the most cases, but not by much. Everyone who had AF needed treatment to reduce stroke risk. Other types of irregular heartbeats were also common in people with OSA—especially those found during sleep. One type, called atrial tachycardia (AT), could lead to AF in the future. In conclusion, although AF was not very common in this younger, low-risk group, the findings suggest that screening may be more helpful in older OSA patients with more health problems. Larger studies are needed to better understand the value of early AF screening in these higher-risk groups.

Keywords
Introduction
Atrial fibrillation (AF) is one of the most common arrhythmic syndromes worldwide. At least 33.5 million people are affected by AF, and this number is still increasing. 1 The incidence rate of AF is about 2%–3% in both white and African-American populations. 2 One of the most important risk factors for AF is advanced age. The prevalence of AF in patients over 65 years old is about 5.5% in a European study 3 and about 1.9% in a Thai study. 4 This demonstrates that different populations have varying prevalences of AF.
In patients with cerebrovascular disease, the prevalence of AF is 20%–30% in all ischemic stroke patients and 10% in cryptogenic stroke patients. 5 Due to the high morbidity and burden of cerebrovascular disease on patients and caregivers, AF screening could benefit certain populations by allowing earlier treatment and reducing the risk of developing cerebrovascular disease. Asymptomatic AF has been associated with increased risk and mortality compared to symptomatic AF, independently. The potential to prevent AF-related strokes depends on identifying appropriate methods for AF screening in at-risk populations, which could facilitate earlier treatment. However, there are still limited data on the optimal screening method and the populations to be screened in clinical practice. 6
Due to the potential risks of AF screening, such as patient anxiety, overdiagnosis, and overtreatment (which may lead to bleeding risks from anticoagulants and the detection of other abnormalities that require invasive diagnostic tests like angiography), clinicians should carefully select populations where the benefits of screening outweigh the harms. 5 According to the standard European AF guidelines, the only Class I recommendation for AF screening is opportunistic screening through pulse taking or electrocardiography (EKG) rhythm strips in patients over 65 years old, as well as regular interrogation of pacemakers and implantable cardioverter defibrillators for atrial high-rate episodes. Systematic EKG screening in patients over 75 years old or those at high risk of stroke is a Class IIa recommendation. 5 However, the US Preventive Services Task Force indicates that the evidence is insufficient to assess the balance of benefits and harms of AF screening using EKG at present. 7
Apart from the 12-lead EKG, there are many tools for AF screening, such as pulse taking, oscillometric blood pressure cuffs, photoplethysmograms on smartphones or smartwatch devices, handheld EKGs, Holter monitoring, EKG patches, or implantable loop recorders. 6 Each of these methods has different sensitivities and specificities, with the 12-lead EKG considered the gold standard. Due to the heterogeneity of the populations studied in AF screening tool research, we cannot determine which tools are best for AF screening. 5 The AliveCor or Kardia handheld EKG is one of the most convenient and easy-to-use screening tools, demonstrating good sensitivity and specificity in the results of many studies.8–11
In a previous randomized controlled trial for AF screening using handheld EKG, the REHEARSE-AF study, patients aged 65 years or older with a CHA2DS2-VASc score of at least 2, and who were free from AF, were randomized to either the handheld EKG arm or the routine care arm. The results showed that the handheld EKG arm was more likely to identify incident AF than the routine care arm over a 12-month period, with a hazard ratio (HR) of 3.9. 12 This demonstrated the efficacy of systematic AF screening using handheld EKG compared to routine care, which consisted of regular clinical follow-up with a general practitioner. Another recent large randomized controlled trial for AF screening using handheld EKG is the STROKESTOP trial. This study enrolled all individuals aged 75–76 years living in Sweden and randomly assigned them to either screening for AF with intermittent EKG (Zenicor handheld EKG, Zenicor Medical Systems AB, Stockholm, Sweden) over 14 days or a control group. The results showed that the proportion of people diagnosed with AF increased from about 12.1% to 14.0% in the invited group, while there was no change in the control group (the percentage remained around 12.8%). This led to a reduction in ischemic stroke in the participants who underwent screening versus those in the control group (HR: 0.76; 95% confidence interval: 0.68–0.87) over a median 6-year follow-up. 13 These studies highlight the benefits of systematic AF screening when performed in an appropriate population.
Obstructive sleep apnea (OSA) is a common comorbidity and risk factor for AF, with several studies demonstrating a strong association between the two conditions.14–16 The prevalence of sleep-breathing disorders is about 60% in AF patients with normal left ventricular function. 17 OSA may contribute to AF through several mechanisms, including structural remodeling of the pulmonary veins, functional remodeling of atrial conduction velocity and sinus node recovery time, hypoxemia leading to hypoxic vasoconstriction, and an increase in sympathetic autonomic tone, making it a high-risk condition for developing and sustaining AF.14,15,18–21 Recent evidence also emphasizes the critical role of OSA-induced sympathetic activation, a complex interplay between intermittent hypoxia, oxidative stress, inflammation, and autonomic dysregulation, which significantly contributes to cardiac arrhythmogenesis. 22 Furthermore, treatment of OSA can significantly increase the success rate of AF rhythm control. 19 Given the substantial overlap between OSA and AF, routine early AF screening in patients diagnosed with OSA, even in the absence of symptoms, may be beneficial. Implementing such proactive measures can facilitate early intervention, reduce the incidence of AF-related complications, and improve patient outcomes.
We hypothesize that patients with OSA are a high-risk group that would benefit from AF screening. To date, there are no data on the prevalence of AF in OSA patients from either opportunistic or systematic AF screening in Thailand. Since OSA occurs at night during sleep, the timing of AF screening may affect the prevalence of the disease (whether the patient is awake or asleep). Therefore, we decided to collect data from three different screening methods: awake opportunistic screening through pulse taking, awake systematic screening using handheld EKG, and asleep EKG during polysomnography. This is the first study to explore the prevalence of AF using different screening methods, and the results of this study could help determine whether AF should be screened in this group and which screening method is most appropriate. Additionally, we aim to study how many positive screening tests could lead to a change in AF treatment with anticoagulation, according to current standard guidelines.
Methods
Study design
This study was a prospective, single-center, cross-sectional study. The protocol was approved by the local ethics committee from the Institutional Review Board of Faculty of Medicine Chulalongkorn University (IRB number 0013/65). The investigators informed all patients through both oral and written documents. Written informed consent was obtained from all patients before the study was conducted. All analyses were performed independently by authors and statisticians at King Chulalongkorn Memorial Hospital.
Patients
All adult patients (⩾18 years old) who were suspected of having OSA based on clinical criteria and who had undergone polysomnography between March 2022 and March 2023 were screened. We enrolled patients who had a diagnosis of clinical OSA and were referred for polysomnography at King Chulalongkorn Memorial Hospital by a primary physician during this period. The clinical criteria for OSA were based on the Thai Obstructive Sleep Apnea Guideline 2018. All patients provided written informed consent. We excluded patients who were unable to follow up at King Chulalongkorn Memorial Hospital or did not send data from AliveCor to the primary investigator.
Interventions
AF was screened using three different methods in all patients: (1) Opportunistic AF screening through pulse taking for 60 s to check for an irregular pulse by a healthcare professional during a routine visit within a 2-week period after enrollment. Patients with an irregular pulse were advised to undergo a 12-lead EKG to confirm the presence of AF. (2) Systematic AF screening using a handheld EKG over a 2-week period. A handheld EKG (AliveCor device) was provided to all patients. Patients were instructed to use the device at least twice daily: once after waking up and once before going to sleep. They could also perform additional tests if they experienced palpitations. The data were sent to the investigators via a mobile application. (3) AF screening with a single-lead EKG recorded during polysomnography, which is routinely performed for all patients. These data were collected from the database on the day of the polysomnography at King Chulalongkorn Memorial Hospital. The first two AF screening methods were performed while patients were awake, and the third method was performed while patients were asleep. All AF screening data were reviewed by the primary investigators and cardiologists. The polysomnography EKG was interpreted for the entire duration of the sleep study (typically 6–8 h). AF was defined as an EKG recording of at least 30 s with an irregular rhythm and atrial fibrillatory waves.
Follow-up and data collections
Patients were followed for a total of 14 days after the day of enrollment. All medical data were collected through personal interviews and electronic medical records. Polysomnography data were reviewed by a sleep medicine specialist, and the EKG data in the study were reviewed by a cardiologist. Poor-quality EKGs that could not be interpreted were labeled as artifacts.
Outcomes
The primary outcome is the prevalence of AF detected using the three aforementioned methods. Prevalence from these methods will be collected and analyzed to determine whether there is any statistically significant difference between them. The secondary outcomes include the proportion of patients with detected AF who are recommended for anticoagulant treatment according to current standard AF guidelines (CHA2DS2-VASc score ⩾2 for male patients and ⩾3 for female patients), as well as the prevalence of other arrhythmias detected by the AliveCor handheld EKG and the EKG from the polysomnography.
Sample size and statistical analysis
This study is the first to screen for AF in OSA patients using three different methods. The sample size was calculated based on the prevalence of AF in OSA patients from the ICD-10 data at King Chulalongkorn Memorial Hospital (only inpatient data were available). According to the ICD-10 database of King Chulalongkorn Memorial Hospital, a total of 777 patients were diagnosed with OSA, and 112 out of these 777 patients were also diagnosed with AF, resulting in an expected prevalence of approximately 14.4%. Therefore, a total sample size of at least 191 patients was required. Categorical data are presented as numbers and percentages, while continuous variables are presented as means and medians. A comparison between the three screening methods was conducted using Fisher’s exact test and the Chi-square test. All analyses were performed using IBM SPSS version 22.0 (IBM Corp., Armonk, NY, USA).
Results
A total of 306 patients were invited to participate in this study. Of these, 201 patients provided written informed consent and were enrolled in the study. A total of 105 patients were excluded or did not participate. The most common reason for non-participation was personal preference (96 patients). Additionally, seven patients did not have mobile phones compatible with the AliveCor handheld EKG application, and two patients were lost to follow-up during data collection. The flowchart of patient recruitment is shown in Figure 1.

Allocation protocol.
Overall, the baseline characteristics are shown in Table 1. Interestingly, these OSA patients have fewer AF risk factors than we expected. Of the patients, 56.7% are male, and the mean age is 46 years. Regarding comorbidities, 3% have a history of heart failure, 2% have a history of paroxysmal AF, 12.4% have diabetes mellitus, 36.3% have hypertension, 37.8% have dyslipidemia, 4.5% have a history of cerebrovascular accident, 2.5% have chronic kidney disease stage III or higher, 4% have hyperthyroidism, and nearly half (47.8%) are obese. In summary, the overall mean CHA2DS2-VASc score is 1, indicating that these OSA patients have a low risk of AF.
Overall baseline characteristics (N = 201).

AADs, antiarrhythmic drugs; AF, atrial fibrillation; AHI, apnea-hypopnea index; BiPAP, bilevel positive airway pressure; CIEDs, cardiac implantable electronic devices; CPAP, continuous positive airway pressure; DHP-CCBs, dihydropyridine calcium channel blockers; DOACs, direct oral anticoagulants; NDHP-CCBs, non-dihydropyridine calcium channel blockers; NYHA, New York Heart Association; OACs, oral anticoagulants; OSA, obstructive sleep apnea.
All 201 patients have clinical OSA; 198 (98.5%) of these patients had confirmed OSA based on polysomnography results. Most of the patients (63.2%) have severe OSA, defined as an apnea-hypopnea index (AHI) >30, with a median AHI of 40.8. About one-quarter (25.4%) of the patients are currently receiving continuous positive airway pressure (CPAP) treatment, which seems low compared to the number of severe OSA patients.
Factors that may lower the prevalence of AF in this study include the infrequent use of antiarrhythmic drugs. Only 8.5%, 0.5%, and 1% of patients used beta-blockers, non-dihydropyridine calcium channel blockers, and class I antiarrhythmic drugs, respectively. None of the patients used class III antiarrhythmic drugs or any other antiarrhythmic medications. Seven patients (3.5%) were already using oral anticoagulants (OACs). Four of them used OACs for AF, and three used OACs for venous thromboembolism. Less than half (three out of seven) of them received direct oral anticoagulants (DOACs), while the other four patients were on warfarin.
Primary outcomes
The primary outcomes are the prevalence of AF detected by opportunistic AF screening via pulse taking, systematic AF screening using the handheld EKG for 2 weeks, and EKG from polysomnography, which were 1.5%, 2.5%, and 2.0%, respectively (Table 2). Notably, all four known paroxysmal AF patients had positive screening results from both the handheld EKG and EKG from polysomnography, but the opportunistic screening by pulse taking missed detecting AF in one of these patients. Additionally, there was one patient who had a positive AF screening test only from the systematic AF screening using the handheld EKG, with negative results from the other methods. However, no statistically significant difference was observed between these methods.
Primary outcome: Prevalence of AF detected by all screening methods.
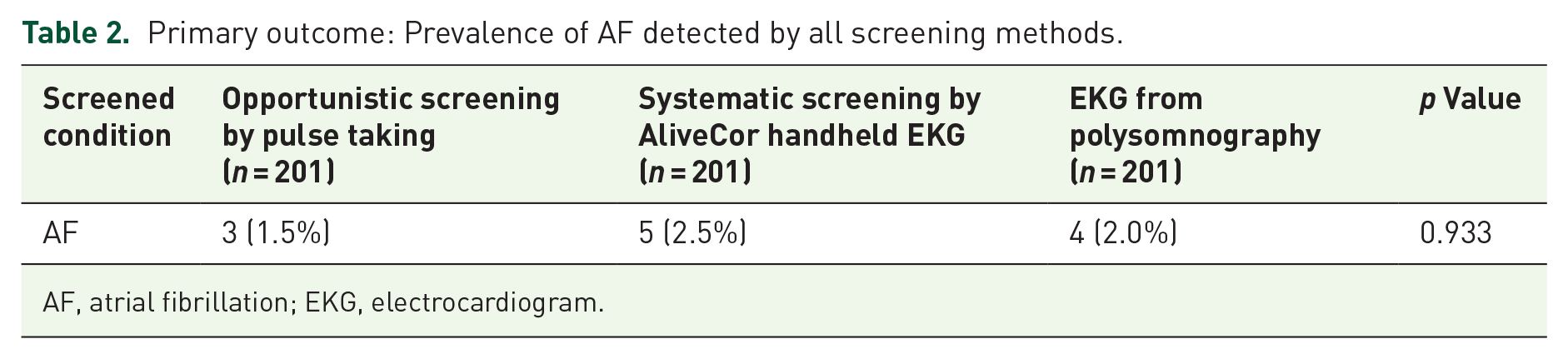
AF, atrial fibrillation; EKG, electrocardiogram.
Patients who test positive for AF using any screening method tend to be significantly older, with an average age of 61 ± 13, compared to 45 ± 15 for those who test negative (p = 0.034). They also have a higher incidence of valvular heart disease (20% vs 0%, p = 0.025), heart failure (40% vs 2%, p = 0.003), prior symptomatic AF (60% vs 0.5%, p < 0.001), diabetes mellitus (60% vs 11.2%, p = 0.014), and a history of hyperthyroidism (40% vs 3.1%, p = 0.013). Additionally, these patients tend to use more medication, including digoxin (40% vs 0%, p < 0.001), warfarin (40% vs 1%, p < 0.001), and DOACs (40% vs 0.5%, p < 0.001).
Screening positive for AF also indicates a higher risk for AF, as demonstrated by a significantly higher CHA2DS2-VASc score of 2.8 ± 1.1 compared to 1.0 ± 1.1 for screening-negative patients (p = 0.002). All patients who test positive have a CHA2DS2-VASc score of 2 or higher (see Table 3).
Baseline characteristics categorized by AF status.

AADs, antiarrhythmic drugs; AF, atrial fibrillation; AHI, apnea-hypopnea index; BiPAP, bilevel positive airway pressure; CIEDs, cardiac implantable electronic devices; CPAP, continuous positive airway pressure; DHP-CCBs, dihydropyridine calcium channel blockers; DOACs, direct oral anticoagulants; NDHP-CCBs, non-dihydropyridine calcium channel blockers; NYHA, New York Heart Association; OACs, oral anticoagulants; OSA, obstructive sleep apnea.
Secondary outcomes
The secondary outcomes are the proportion of patients with detected AF from the screening tests, which indicate the need for class I recommended anticoagulant treatment according to current standard AF guidelines. All patients (100%) who had positive AF screening tests from both opportunistic AF screening and systematic AF screening have indications for OACs (Table 4).
Secondary outcome: The proportion of patients with detected AF from the screening test who are indicated for anticoagulant treatment.
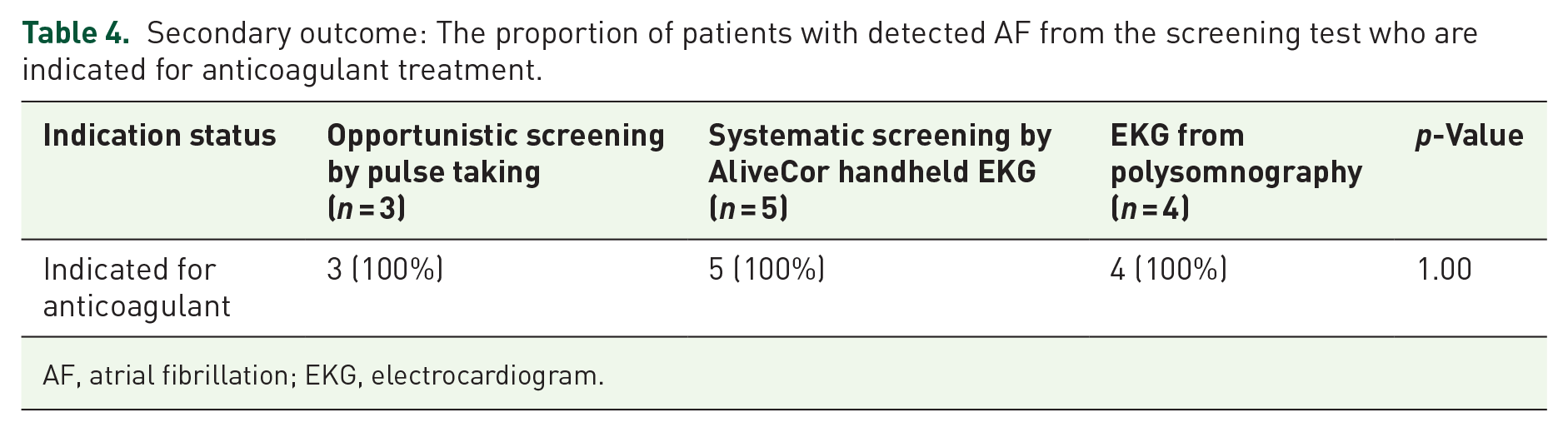
AF, atrial fibrillation; EKG, electrocardiogram.
Other secondary outcomes include arrhythmias other than AF detected by the handheld EKG and EKG from polysomnography (Table 5). Interestingly, several non-AF arrhythmias were significantly detected by both methods. These include sinus tachycardia (18.9%), premature ventricular contractions (PVCs; 8.5%), premature atrial contractions (PACs; 7.0%), atrial tachycardia (AT; 1%), both PACs and PVCs (1.5%), and sinus bradycardia (0.5%) detected by the handheld EKG. For the EKG from polysomnography, the detection rates for the same arrhythmias were 25.4%, 11.4%, 8.0%, 7.5%, 0.5%, and 0.5%, respectively.
Secondary outcome: arrhythmias other than AF.

AF, atrial fibrillation; AT, atrial tachycardia; PACs, premature atrial contractions; PVCs, premature ventricular contractions; SVT, supraventricular tachycardia; VT, ventricular tachycardia.
There was a statistically significant higher prevalence of AT (an arrhythmia that may lead to AF) detected from the polysomnography EKG compared to the handheld EKG (7.5% vs 1%, p = 0.001). The detection rates for other non-AT arrhythmias by both methods were not statistically different. Additionally, 4.5% of the EKGs from polysomnography were labeled as artifacts that could not be interpreted.
Post hoc analysis
We hypothesize that OSA is a significant risk factor for AF development and that younger patients with OSA are more likely to experience AF than the general population. To test this, we conducted a post hoc analysis to examine whether the severity of OSA and age (⩾46 years old, the mean age of the study population) affect AF prevalence as detected by screening tools.
Our analysis found that the AF prevalence was 4.3% in patients ⩾46 years old and 0.9% in those <46 years old. Additionally, the AF prevalence was 0%, 2.5%, and 3.2% in patients with mild, moderate, and severe OSA, respectively. However, there was no statistically significant difference in AF prevalence detected by screening tools when stratified by OSA severity (measured by the AHI) and an age cutoff of ⩾46 years old in this study (Tables 6 and 7). These findings may be limited by a lower AF prevalence than expected, which may have underpowered the study to demonstrate statistical significance.
Prevalence of AF categorized by age ⩾46 years old.

AF, atrial fibrillation.
Prevalence of AF categorized by the severity of OSA.

AF, atrial fibrillation; AHI, apnea-hypopnea index; OSA, obstructive sleep apnea; PSG, polysomnography.
Discussion
In this first AF screening study in OSA patients, the results demonstrated that there is no difference in the AF detection rate among awake opportunistic AF screening by pulse taking, awake systematic AF screening by AliveCor handheld EKG, and asleep EKG during polysomnography. Although the handheld EKG detected a numerically higher number of AF cases, this difference was not statistically significant, suggesting that further studies with larger sample sizes may be necessary to confirm the optimal screening method. The prevalence of AF detection in this population was about 1.5%–2.5%, which is much lower than initially expected, but slightly higher compared to the prevalence of AF in patients over 65 years old in Thailand (1.9%), 4 a population currently considered for AF screening according to standard AF guidelines.
Due to the lower AF prevalence than expected, this study may be underpowered to identify differences in AF prevalence among the different screening methods. It may be that more patients need to be screened. The lower-than-expected AF prevalence in this OSA patient group could be attributed to several factors: the patients are relatively young (mean age 46 years), have few comorbidities, and have a low baseline CHA2DS2-VASc score (mean 1.1), which indicates low AF risk. During enrollment, about one-third of the patients (103 out of 306) were excluded due to their preferences or lack of available devices for testing. This may have led to selection bias, as older patients tend to be less comfortable using electronic devices and mobile applications, making them more likely to refuse participation, while younger patients generally do not face this issue. Increasing age and comorbidity burden are strong predictors of AF.16,23–26 Systematic AF screening in older adults has been shown to reduce stroke and improve the detection of asymptomatic cases, supporting the benefit of targeting high-risk populations.13,27 Therefore, the younger and healthier patient population (with a low CHA2DS2-VASc score) in this study would be expected to have a lower prevalence of AF, consistent with our findings. Additionally, the initial estimated AF prevalence was calculated from the ICD-10 data, which included more inpatient (IPD) patients than outpatient (OPD) patients. The critical illness associated with hospital admission may also have affected the AF prevalence, causing it to be higher than in the results of this study.
To demonstrate, compared to previous studies that showed positive outcomes for systematic AF screening by handheld EKG in detecting more asymptomatic AF,12,13 the median age in this AFOSA study is much lower than in previous studies (65–75 vs 46 years old), and comorbidities are also much lower. These factors may explain why this study showed negative results. Nonetheless, our post hoc analysis revealed that there was no significant difference in the prevalence of AF based on age when compared to the mean age of this study. Additionally, it appears that the severity of OSA does not have a significant impact on the prevalence of AF. However, all patients detected by these screening methods have clinical significance that warrants anticoagulant treatment.
Interestingly, the findings of significantly higher prevalence of non-AF arrhythmias in patients with OSA in this study, particularly sinus tachycardia, PVCs, PACs, and notably AT, are clinically meaningful and deserve further attention. Previous studies have shown a substantially lower prevalence of these arrhythmias in healthy populations, with reported rates of PACs, PVCs, and AT being approximately 0.14%, 19 0.45%, 28 and 0.46%, 29 respectively. In contrast, our study demonstrated much higher prevalence rates in OSA patients: PACs at 7%–8%, PVCs at 8.5%–11.4%, and AT significantly higher at 7.5% during sleep monitoring by polysomnography, compared to just 1% detected during awake monitoring with a handheld EKG. However, continuous EKG monitoring during polysomnography lasted 6–8 h, which is considerably longer than the brief, intermittent recordings obtained with a handheld EKG, thereby increasing the likelihood of detecting arrhythmias. The heightened prevalence of these arrhythmias suggests that OSA may act as an arrhythmogenic substrate rather than merely coexisting with arrhythmias. The physiological stresses induced by OSA, including intermittent hypoxia, fluctuations in intrathoracic pressure, oxidative stress, and increased sympathetic nervous system activation, are well-established mechanisms contributing to atrial and ventricular remodeling.14,19 Particularly noteworthy is AT, which is recognized as a potential precursor to AF, underlining its significance as a clinical marker warranting proactive intervention and closer surveillance in OSA patients. 29 These results imply the need for clinicians to be vigilant regarding not only AF but also other significant arrhythmias when managing patients with OSA. Furthermore, therapeutic strategies targeting OSA, such as CPAP or bilevel positive airway pressure, could potentially reduce these arrhythmias and associated cardiovascular risks. Follow-up studies investigating changes in arrhythmia prevalence following effective OSA management are required to confirm this hypothesis and potentially refine screening and management guidelines for this high-risk population.
Limitations
The major limitations of this study are: (1) the small sample size, calculated using inpatient ICD-10 data, which may overestimate AF prevalence compared to the broader outpatient OSA population, potentially limiting generalizability and leading to underpowered results; (2) selection bias, as nearly one-third of the patients did not provide written informed consent to participate in the study; (3) the unclear influence of race/ethnicity, sex, and obesity status on AF prevalence, which our study was not designed or powered to assess; and (4) the use of intermittent AF screening, which may miss some AF patients compared to continuous monitoring methods such as long-term Holter monitoring or implantable loop recorders. However, intermittent AF screening using a handheld EKG is significantly more convenient and cost-effective, making it a more practical option for AF screening in real-world settings.
Conclusion
AFOSA study is the first AF prevalence study in OSA patients via three different screening methods, opportunistic AF screening by pulse taking, systematic AF screening by handheld EKG, and EKG from polysomnography. The prevalence of AF in this study ranged from approximately 1.5% to 2.5%. The handheld EKG systematic screening method had the highest AF detection rate (2.5%), but this was not statistically significant. All of the patients who had positive screening tests had indications for OAC treatment. The prevalence of other arrhythmias was higher than in the general population, especially AT. Longer-duration systematic AF screening methods may be more beneficial in OSA patients, particularly those of older age with more comorbidities.
Clinical perspectives
AF screening with appropriate methods in high-risk populations may lead to early detection and early treatment that reduces morbidity and mortality. OSA patients may have a high risk for AF that benefit from screening. This study aimed to show the burden of AF in OSA patients and provide information about appropriate screening methods. Opportunistic AF screening by pulse taking seems to have the same AF detection rate in OSA patients compared to other systematic AF screening by EKG. The results support the current standard guideline recommendations from the 2024 ESC guidelines for the management of AF, which state that sleep apnea is one of the risk factors associated with incident AF. Population-based screening for AF should be considered in individuals aged ⩾65 years with additional risk factors to ensure earlier detection of AF. 23
Future directions
Further large-scale studies are needed to evaluate the health outcomes of AF and non-AF arrhythmia screening in patients with OSA. A longer follow-up or extended AF screening duration may increase the detection rate. While younger OSA patients may benefit from AF screening, it is likely to be more efficient and have a greater clinical impact when focused on older OSA patients with additional cardiovascular comorbidities. Future research should prioritize this higher-risk group to optimize screening efficiency and improve outcomes.
Footnotes
Acknowledgements
We would like to thank all the supporting personnel who assisted us by providing the essential data, without which we would not have been able to efficiently complete this project.