
Abstract
Background:
This was a meta-analysis of continuous positive airway pressure (CPAP) compliance. We compared telemonitor (TM) care with usual care and supervised PAP titration (SPT) in the sleep unit with home auto-adjusting pressure titration (HAPT) in patients with obstructive sleep apnea (OSA).
Methods:
We searched PubMed, Web of Science, Scopus, and Medline for appropriate randomized controlled trials (RCTs) that compared TM care with usual care for patients with OSA. Review Manager 5.3 was used for all comparisons and analyses.
Results:
Our meta-analysis included 19 studies involving a total of 2464 patients with OSA; CPAP compliance was significantly higher in the TM care group [mean difference (MD) 0.68 h, 95% confidence interval (CI) 0.48–0.89 h, I2 = 49%] compared with the usual care group. When we compared SPT and HAPT, two groups did not exhibit significantly different levels of CPAP compliance (MD −0.34 h, 95% CI −0.72–0.05 h, I2 = 91%). Subgroup analysis comparing the SPT with HAPT in CPAP compliance was grouped by follow-up time (⩾3 months or <3 months). Once again, there were no between-group differences in either long-term (MD = 0.56 h, 95% CI = 1.39–0.26 h, I2 = 91%), or short-term (MD = 0.34 h, 95% CI = 0.26–0.27 h, I2 = 14%) follow up.
Conclusions:
TM care was associated with significantly greater CPAP compliance compared with usual care. Also, HAPT was not inferior to SPT for CPAP compliance.
Introduction
Obstructive sleep apnea (OSA) is caused by a blockage or obstruction of the airway, and features a range of symptoms, including snoring, episodes of oxygen desaturation, and arousals from sleep. The prevalence of OSA increases with age 1 ; among middle-aged people, it influences more than 20% of males and more than 8% of females. 2 Health care resources related to the diagnosis and treatment of OSA are reportedly inadequate. 3 OSA poses a range of risks, including hypertension, stroke, heart failure, etc.2,4,5 Some of these risks can be alleviated by continuous positive airway pressure (CPAP) treatment. Especially for patients with moderate and severe OSA, CPAP has been recommended as a first-line treatment. 6
Compliance is important during CPAP treatment. Over the past two decades, several psychoeducational and technological interventions (e.g. group education sessions, 7 intensive patient education and support protocol,8,9 and motivational enhancement programs 10 ) have emerged with the common goal of increasing CPAP compliance. Most of these interventions have demonstrated only a modest impact on compliance. Moreover, intensive support protocols still required substantial time and resources to implement.
Current technological advances have facilitated telemonitor (TM) care in routine clinical practice.11,12 In addition, the devices that patients use can auto-adjust pressure titration at home without the supervision of sleep technicians/doctors.13,14 Few prior integrated studies or and meta-analyses have been used to guide clinical practice. We sought to carry out a comprehensive meta-analysis of previously published studies that examined supervised PAP titration (SPT) and home auto-adjusting pressure titration (HAPT), and follow-up procedures, including TM care or usual care, with regards to CPAP compliance.
Methods
Search strategy
Two investigators independently searched articles from several databases (PubMed, Web of Science, Scopus, and Medline). The reference lists of eligible studies and relevant papers were also searched manually and reviewed. The search terms included ‘OSA’, ‘obstructive sleep apnea’, ‘OSAHS’, ‘obstructive sleep apnea and hypopnea syndrome’, ‘sleep apnea’, ‘compliance’, and ‘adherence’. In PubMed, we used (‘OSA’ or ‘OSAHS’ or ‘obstructive sleep apnea’ or ‘obstructive sleep apnea and hypopnea syndrome’ or ‘sleep apnea’) and (‘compliance’ or ‘adherence’). The final search date was 17 August 2019. The search terms and search strategies for two topics (topic 1: TM care versus usual care; topic 2: SPT versus HAPT) are shown in the supplementary data. We identified 3451 articles after removal of duplications. We excluded 3431 articles by reading the title and abstract. Finally, there were 19 included RCTs (13 studies for topic 1, and 6 studies for topic 2.11–29 (Figure 1)

Flow diagram for selection of appropriated articles.
Inclusion and exclusion
Inclusion criteria: randomized controlled trial (RCT) primary comparing TM care with usual care, and SPT to HAPT; primary outcome: CPAP compliance; published in English.
We excluded studies that were reviews, retrospective research, or case reports; and studies that did not report insufficient data [e.g. no reports of precise CPAP usage time or rates of CPAP compliant (>4 h) patients].
Data extracted
Two authors (Chongxiang Chen and Lanlan Pang) independently reviewed the identified abstracts and selected articles for full review. A third reviewer (Wei Liao) was brought in to address any discrepancies. For each selected publication, the following baseline and study characteristics were extracted: first author, publication year, country, participant characteristics, follow-up time, and baseline characteristics (Table 1). Interventions included in our studies comprised TM care, usual care, SPT, and HAPT. The definitions of TM care in all the included studies involved collecting data on CPAP treatment efficacy (CPAP compliance, air leaks) in real-time, and transmission of treatment data to clinical sleep center staff. The staff would then contact the patients, if necessary, to solve various problems. In the context of these studies, ‘usual care’ meant regular follow-up and face-to-face contact during the treatment period. ‘SPT’ meant that sleep doctors supervised PAP titration based on polysomnography (PSG) in these studies. ‘HAPT’ meant using autotitration pressure at home. All intervention group settings that were included in the studies are shown in Supplementary Tables 1 and 2. The risks of bias for the included studies are presented in Figures 2 and 3. The risk-of-bias analysis showed that all the studies were comparable (high-quality RCTs) and could be integrated. The efficacy outcome measure was CPAP compliance.
Characteristics of baseline patients.
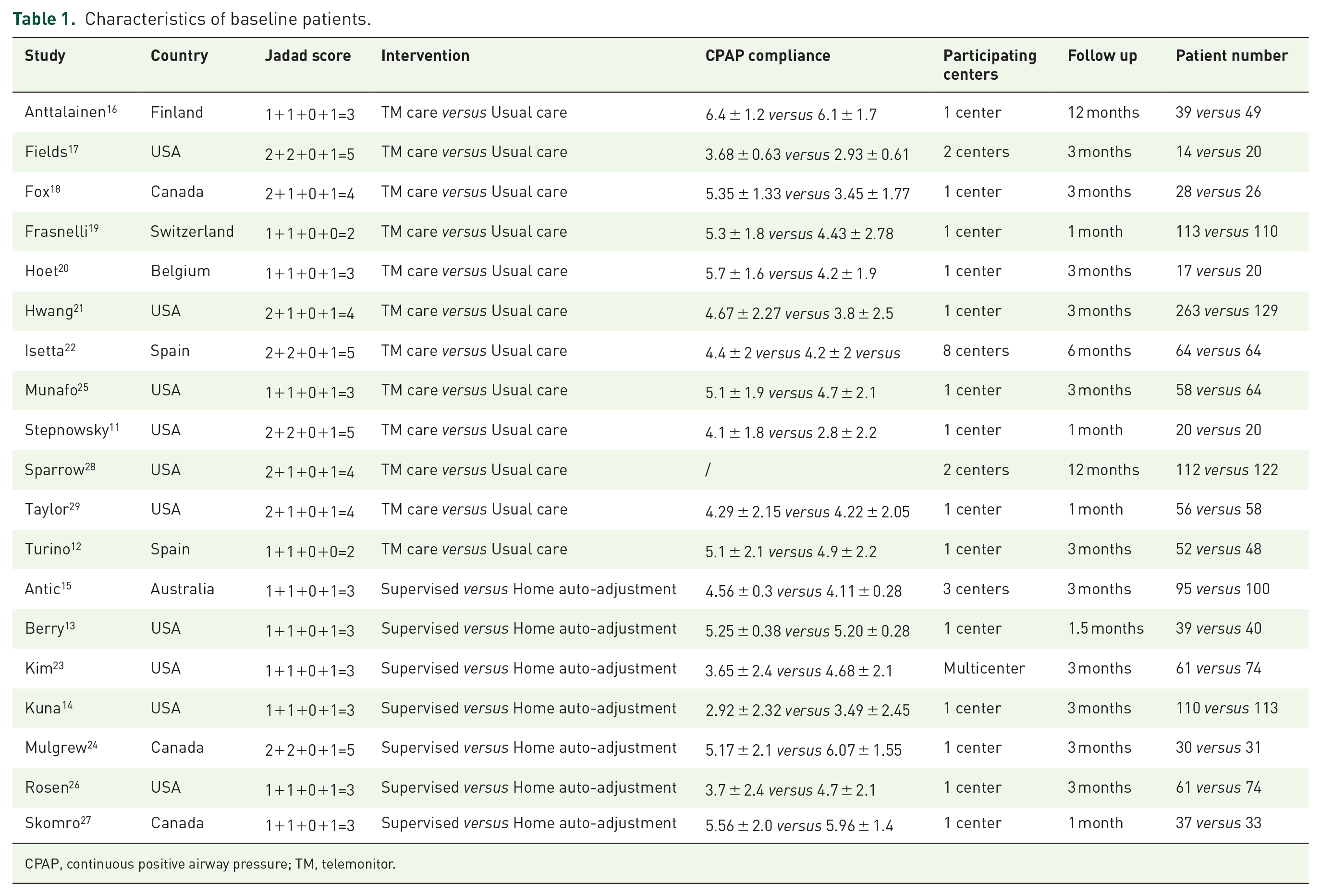
CPAP, continuous positive airway pressure; TM, telemonitor.

Risk of bias graph.

Risk of bias summary.
Risk-of-bias assessment
Trial risk-of-bias was assessed according to the recommendations of the Cochrane Handbook of Systematic Reviews of Interventions, in the following domains: selection bias (random sequence generation and allocation concealment), performance bias (blinding of participants and personnel), detection bias (blinding of outcome assess-ment), attrition bias (incomplete outcome data), and reporting bias (selective outcome reporting) (http://handbook.cochrane.org). The Jadad scale was used to calculate the quality of every enrolled study. In the review of randomization, every study that contained the exact randomized method, we scored as ‘low risk’; however, when the study did not report the exact randomized method, but indicated that the studies were carried out under randomized, controlled designs, we scored them as ‘unclear’, which was similar to other scoring in allocation of randomization, blind method, incomplete outcome data, selective reporting. Other bias sometimes contains unknown risk, so we think we should score all the other bias in every article as ‘unclear’.
Statistic analysis
We pooled data and used mean deviation (MD), with 95% confidence interval (CI) for continuous outcomes: CPAP compliance, Epworth Sleepiness Scale (ESS) change, and changes in the Functional Outcomes of Sleep Questionnaire (FOSQ). We used odds ratios (OR), with 95% CI for the dichotomous outcome: the rate of CPAP compliant (>4 h) patients. We used a fixed-effect model if there was no considerable heterogenous factors among the various studies. We used a random-effects model if the I2 statistic was above 50% and Cochran’s Q statistic had a p value ⩽ 0.1. Funnel plots were used to screen for potential publication bias. All statistical analyses were carried out with Review Manager 5.3 (The Cochrane Collaboration)
Results
The studies included in our meta-analysis were all RCTs, published from 2006 to 2018. The studies were conducted in the USA,11,13,14,17,21,23,25,26,28,29 Spain,12,22 Australia, 15 Canada,18,24,27 Belgium, 20 Switzerland, 19 and Finland. 16 Table 1 presents the basic characteristics of included trials and participants’ demographic data. Three trials were multicenter studies,15,17,22,23,28 and the Jadad Scales of all included studies ranged from 2 to 5.
In total, there were 19 RCTs with 2464 patients. These studies addressed OSA treatment and management, and explored which methods could contribute improved CPAP compliance. Article quality evaluation results are presented in Figures 2 and 3.
Telemonitor care versus usual care
CPAP compliance
When we compared TM care with usual care, our study indicated that telemonitoring follow up could significantly increase CPAP compliance. Our study included 11 studies with a total of 1332 patients11,12,16–22,25,29; the results showed that the compliance outcome of the TM care group was significantly higher than the usual care group (MD 0.68 h, 95% CI 0.48–0.89 h). Heterogeneity testing revealed I2 = 49%, indicating low heterogeneity (Figure 4). We then analyzed CPAP compliance grouped by follow-up time (>3 months or less). The results showed that TM care group compliance was significantly higher than that in the usual care group (MD 0.79 h, 95% CI 0.56–1.01 h, I2 = 48%) for short-term follow up; however, long-term results were not significantly different (MD 0.26 h, 95% CI −0.20–0.71 h, I2 = 0%; Figure 5).

CPAP compliance (hours of daily use) comparing TM care with usual care in OSA patients.
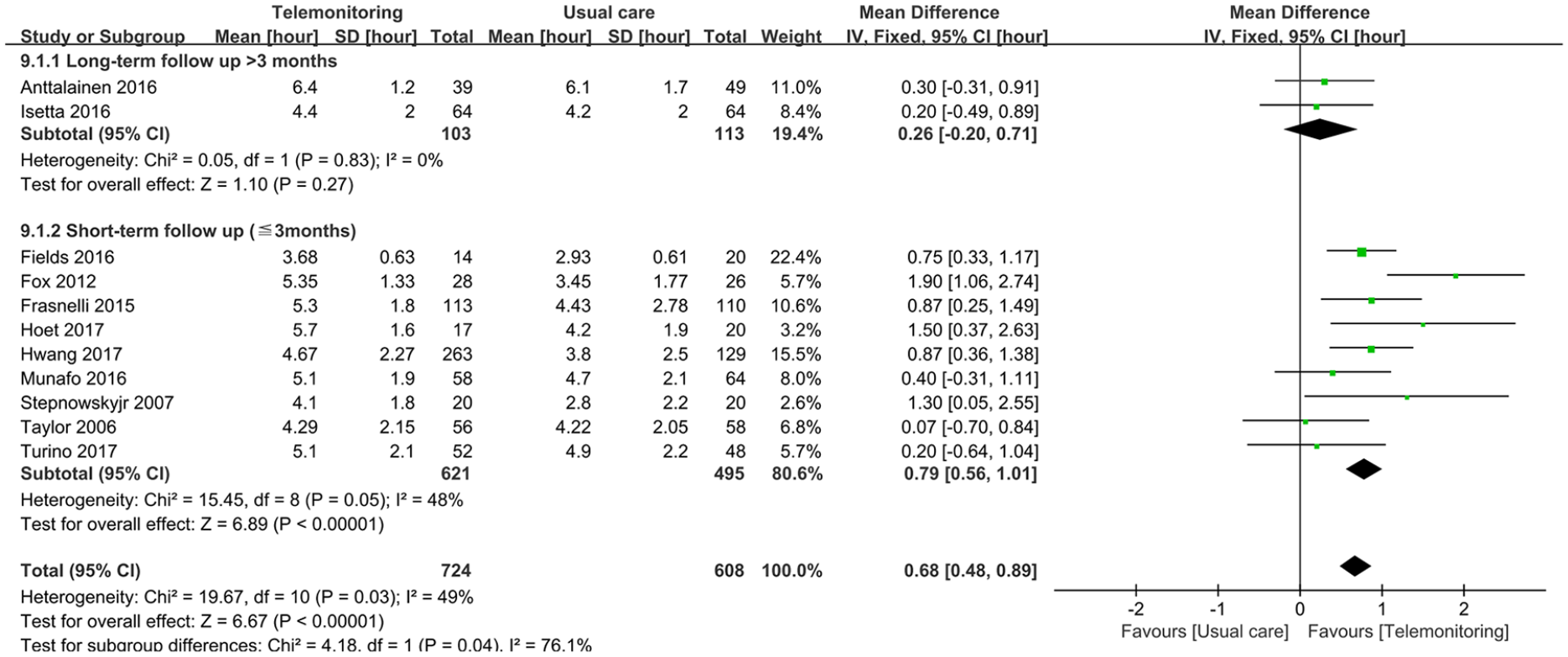
Subgroup analysis of CPAP compliance (hours of daily use) comparing TM care with usual care in OSA patients grouped by follow-up time.
Additionally, we compared the rate of CPAP compliant (>4 h) patients between the TM care and usual care groups. Here, TM care had a significantly higher rate of CPAP compliant patients than usual care (OR 1.81, 95% CI 1.33–2.46). Heterogeneity testing revealed I2 = 0%, indicating low heterogeneity (Supplementary Figure 1).
ESS change
To compare TM care with usual care in terms of change in ESS, our study included six studies with a total of 726 patients11,16–18,21,25; the results did not show a significant between-group difference (MD 0.12, 95% CI −0.65 to 0.89). Heterogeneity testing revealed I2 = 0%, indicating low heterogeneity (Supplementary Figure 2).
FOSQ change
To compare TM care with usual care for change in FOSQ, we included three studies with a total of 462 patients11,17,21; the results demonstrated a significantly greater change in FOSQ for the TM group (MD 2.05, 95% CI 0.65–3.46). Hetero-geneity testing revealed I2 = 0%, indicating low heterogeneity (Supplementary Figure 3).
Supervised PAP titration versus home autoadjusting pressure titration
CPAP compliance
We compared CPAP compliance in patients who underwent SPT or HAPT. Our search strategy revealed seven studies with a total of 898 patients13–15,23,24,26,27; the two groups did not exhibit any significant differences in CPAP compliance (MD −0.34 h, 95% CI −0.72–0.05 h). Hetero-geneity testing showed that I2 = 91%, indicating high heterogeneity (Figure 6). Subgroup analysis of the included studies, grouped by follow-up time (⩾3 months or <3 months) also demonstrated that two groups were not significantly different in long-term follow up (MD −0.56 h, 95% CI −1.39–0.26 h, I2 = 91%), or short-term follow up (MD 0.00 h, 95% CI −0.26–0.27 h, I2 = 14%; Figure 7).

CPAP compliance (hours of daily use) comparing supervised PAP titration with home auto-adjusting pressure titration in OSA patients.

Subgroup analysis of CPAP compliance (hours of daily use) divided by follow-up time comparing supervised PAP titration with home auto-adjusting pressure titration in OSA patients.
In addition, we compared rates of CPAP compliant (>4 h) patients between patients who received SPT and those who received HAPT. The results showed no significant between-group difference in the rate of CPAP compliant patients (OR 0.72, 95% CI 0.48–1.08). Heterogeneity testing revealed I2 = 0%, indicating low heterogeneity (Supplementary Figure 4).
ESS change
Comparing the SPT and HAPT groups for change of ESS, we identified five studies with a total of 635 patients.13–15,24,26 The two groups were not significantly different (MD −0.21, 95% CI −0.68 to 0.26). Heterogeneity testing showed that I2 = 68%, indicating high heterogeneity (Supplementary Figure 5).
FOSQ change
For comparing SPT with HAPT in the change of FOSQ, we included four studies with a total of 592 patients.13–15,26 The results indicated there was a significantly greater change in FOSQ among patients who underwent SPT (MD 0.22, 95% CI 0.07–0.38). Heterogeneity testing revealed I2 = 0%, indicating low heterogeneity (Supplementary Figure 6).
We analyzed potential publication bias of treatment and management methods used for treating patients with OSA. Our results revealed a funnel plot, and the results showed no significant differences (Supplementary Figure 7).
Discussion
Tools for diagnosing and making individualized treatment decisions are needed by practitioners who manage patients with OSA. As the first-line recommended treatment, compliance with CPAP is crucial to improving quality of life and cardiovascular outcomes 30 ; however, the predictors of therapy adherence remain unknown. Consequently, we must enhance CPAP compliance through intervention methods.
Our results provide a comprehensive strategy for improving the management and treatment of patients with OSA. Our results indicate that the TM care group had significantly better CPAP compliance compared with the usual care group. Effective follow up should be considered first in patients with OSA who are treated with CPAP. A study conducted by Mendelson and colleagues showed that TM did not improve blood pressure to reduce the occurrence of cardiovascular events. 31 From our point of view, why blood pressure was used as an outcome is unclear. Further, the follow-up time in their study was too short to detect differences in blood pressure changes.
Moreover, in our study, HAPT was non-inferior to SPT in terms of CPAP compliance. Traditionally, when a patient is diagnosed with OSA, they returns to the sleep unit for additional polysomnography to determine the therapeutic CPAP level. Nowadays, home diagnosis and auto-adjusting pressure titration are alternative treatment methods. However, for the purposes of diagnosis, the accuracy of these technologies remains insufficient. 32 For pressure-titration, some studies have shown that HAPT produces effects similar to SPT.33–35 Nowadays, auto-adjusting pressure titration is becoming popular in OSA patients, and we believe that simplified OSA diagnosis and treatment methods are more important for patients in rural or remote areas.
In 1997, Weaver and colleagues developed the FOSQ, 36 a self-administered tool that quantifies the effects of daytime sleepiness on activities of everyday living. 37 In 2009, Chasens and colleagues designed a short and easier-to-use version of the FOSQ based on the original. 38 In our study, the change of FOSQ in the TM care group was significantly greater than that detected in the usual care group. Further, the scores increased more in the SPT group than in the HAPT group, which meant that TM care and SPT had better treatment efficacy than the comparators.
The limitations of our study were as follows. First of all, the primary outcome in our study was CPAP compliance, but the follow-up time was different for each included study, leading to high heterogeneity in the results. To address this, in subgroup analysis, we used 3 months as a cut-off to calculate long- and short-term compliance. In addition, although the TM care group had the same definition in every study, which were real-time feedback on compliance and problem solving, most of the included studies used telephone or E-mail to follow-up, but some also used specific advanced devices. Although TM care is more useful in CPAP compliance than usual care, the application of advanced devices depends largely on individual income, and thus is not useful for most patients of lower socioeconomic status. Lastly, HAPT is not a pathway suitable for all patients suffering from OSA. It is limited to cases of apnea hypopnea index (AHI) >30; no obesity hypopnea syndrome (OHS); no central sleep apnea (CSA), cardiac/pulmonary comorbidities; the patient must be able to manage APAP alone for the first night; and not live too far from their nearest treatment center. The guidelines also recommended that APAP should be utilized in OSA patients with no significant comorbidities. 39 This study presents a comprehensive clinical pathway for improving CPAP compliance; however, we still have a long way to go. 39
Conclusion
To improve CPAP compliance, using TM care is more useful than usual care. In addition, HAPT showed non-inferior efficacy in CPAP compliance than SPT in the sleep unit. Clinicians should consider the use of more effective methods for improving CPAP compliance in patients with OSA.
Supplemental Material
Supplementary_Data – Supplemental material for Telemonitor care helps CPAP compliance in patients with obstructive sleep apnea: a systemic review and meta-analysis of randomized controlled trials
Supplemental material, Supplementary_Data for Telemonitor care helps CPAP compliance in patients with obstructive sleep apnea: a systemic review and meta-analysis of randomized controlled trials by Chongxiang Chen, Jiaojiao Wang, Lanlan Pang, Yanyan Wang, Gang Ma and Wei Liao in Therapeutic Advances in Chronic Disease
Footnotes
Acknowledgements
Authors Chongxiang Chen, Jiaojiao Wang, and Lanlan Pang contributed equally to this work.
We acknowledge all the authors of the contributing studies.
Author contributions
Chongxiang Chen designed the study. Chongxiang Chen designed the search strategy and performed the search. Chongxiang Chen and Lanlan Pang performed abstract screening, full text screening, data extraction, and risk of bias assessment. All the authors drafted the manuscript. Jiaojiao Wang, and Gang Ma helped in the revision process. All authors revised the manuscript, as well as reading and approving the final manuscript.
Funding
The author(s) received no financial support for the research, authorship, and publication of this article.
Conflict of interest statement
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval and consent to participate
Not applicable.
Consent for publication
All authors have agreed to the publication of this manuscript.
Availability of data and materials
The datasets used and/or analyzed in the current study are available from the corresponding author upon request.
Data availability
All data generated or analyzed during this study are included in this published article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.