
Abstract
Background:
The role of postoperative radiotherapy (PORT) for patients with completely resected stage N2 non-small-cell lung cancer (NSCLC) has been controversial. This study aimed to investigate the efficacy of PORT and prognosis in these patients.
Objectives:
An updated meta-analysis was conducted in this study to investigate the efficacy of PORT and prognosis in patients with completely resected and pathologically confirmed stage N2 NSCLC.
Design:
This study is a systematic review and meta-analysis.
Data source and methods:
Databases were searched up to 2 March 2022. All trials on patients with completely resected and pathologically confirmed stage N2 NSCLC undergoing PORT were screened, and data indicators in the PORT and non-PORT groups were extracted, respectively. The effect of PORT on overall survival (OS), disease-free survival (DFS), local recurrence-free survival (LRFS), and distant metastasis-free survival (DMFS) was estimated. Subgroup and sensitivity analyses were performed.
Results:
In all, 20 studies involving 6340 patients were finally included. The PORT significantly increased OS [hazard ratio (HR) = 0.77, 95% CI: 0.71–0.84, p < 0.001), LRFS (HR = 0.63, 95% CI: 0.52–0.76, p < 0.001), and DFS (HR = 0.72, 95% CI: 0.63–0.82, p < 0.001) while it showed no significant difference in improving DMFS (HR = 0.86, 95% CI: 0.71–1.05, p = 0.14).
Conclusion:
Our results suggest that in the postoperative treatment of patients with completely resected and pathologically confirmed stage N2 NSCLC, the addition of PORT provides better local recurrence control and survival benefit, but no benefit for distant metastases. The PORT may be incorporated into the postoperative treatment options for some patients with high-risk factors. However, it needs to be validated by more prospective studies in the future.
Trail registration:
CRD42022314095.
Introduction
Lung cancer is one of the leading causes of cancer-related deaths worldwide. Non-small-cell lung cancer (NSCLC) accounts for 80–85% of all kinds of lung cancer, 1 with 30% of patients found already at a locally advanced stage at the time of detection. Notably, the completely resected stage N2 NSCLC is considered a heterogeneous and poorly prognostic disease subgroup with diversity in anatomy (location and the number of involved lymph nodes) and biology (histopathology and genetics). 2 Surgical resection is the only potential cure; yet, the risk of local recurrence after surgery is as high as 20–40% 3 and the 5-year overall survival (OS) rate is only 15–25%.4,5 Hence, how can we improve the OS and prognosis in patients with completely resected stage N2 NSCLC through comprehensive postoperative treatment is a hotspot of current research.
Postoperative chemotherapy (POCT) has been proven to be the standard of care in the postoperative period3,6 and can provide a survival benefit, although the role of postoperative radiotherapy (PORT) has been controversial. A meta-analysis conducted in 1998 showed that PORT adversely affected patients with completely resected NSCLC, and although there was a slight increase in survival in patients with pN2, the difference was not statistically significant, 7 which may be related to the excessive late side effects caused by outdated radiation techniques at the time. With the development of radiotherapy techniques, an analysis based on the Surveillance, Epidemiology, and End Results (SEER) database in 2006 8 and the Adjuvant Navelbine International Trialist Associatin (ANITA) trial in 2008 9 has successively confirmed the association of PORT with prolonged survival in patients with postoperative pN2 disease . Multiple studies and meta-analyses have also shown that PORT reduces the incidence of local recurrence and improves disease-free survival (DFS) or OS in patients with completely resected stage N2 NSCLC.5,6,10,11 However, the results of two recent randomized controlled trials (Lung-ART 12 and PORT-C 13 ) conclude that PORT while reducing local recurrence, had no survival benefit, which may be related to the long time span of the studies, the inclusion of early radiotherapy techniques, and the advances in systemic and local treatment of NSCLC. 14 The latest meta-analysis also suggests that PORT, although helpful in increasing DFS and local recurrence-free survival (LRFS), may not be associated with improved OS and should be selected with caution. 15 These conflicting results render the role of PORT uncertain and make researchers rethink the value of PORT.
Early studies involving radiotherapy techniques are not representative of the effectiveness of modern radiotherapy techniques, and the value of PORT in N2 patients should not be easily dismissed. 16 After the publication of the Lung-ART trial, 82% of experts from the European Society for Therapeutic Radiology and Oncology still recommended PORT for pN2 patients with risk factors, especially those pathologically characterized by multiple or multisite lymph nodes. 17 Other clinical factors such as heavy smoking and squamous cell carcinoma are also considered to be closely associated with a higher risk of local recurrence and poor survival outcomes.18,19 Therefore, the question of risk factors for local recurrence in the postoperative period and who might benefit from PORT may become increasingly important. Previous meta-analyses on PORT did not include the stratified analysis from the combination mode of chemoradiotherapy (sequential or concurrent), radiotherapy techniques and dose, and suspected risk factors, and there was a lack of studies on the appropriate population for PORT. In this study, we conducted a meta-analysis of published research trials in recent years with the aim of reassessing the possible benefits of PORT in patients with completely resected stage N2 NSCLC and identifying subgroups of patients who may derive the greatest benefit from PORT to help to improve the pertinence of PORT treatment and provide relevant guidance for clinical work.
Materials and methods
This meta-analysis followed the guidance of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) and the Meta-Analysis of Observational Studies in Epidemiology (MOOSE) guidelines and was registered with the International Prospective Register of Systematic Reviews (ICRS) prior to submission (CRD42022314095).
Search strategy
We comprehensively searched PubMed, Web of Science, Embase, and Cochrane Library databases, and the data search period was up to 2 March 2022. The search terms included the medical terms (Mesh) ‘Carcinoma, Non-Small-Cell Lung’, ‘Radiotherapy’, ‘Chemoradiotherapy, Adjuvant’, and the keyword ‘N2 OR III’. The specific search strategy is presented in the Supplemental Materials. We reviewed the reference lists of all primary studies and references of other review articles. After the duplicate publications of the same trial or multiple articles covering the same study population were identified, studies with the most complete and up-to-date reports were included.
Inclusion and exclusion criteria
Studies were included in this study if they met the following criteria: (1) study subjects: patients aged ⩾18 years with completely resected and pathologically confirmed stage N2 NSCLC; (2) interventions: PORT in the study group and non-PORT in the control group, regardless of whether postoperative adjuvant chemotherapy was combined in both groups; (3) type of outcome: OS, DFS, LRFS, or distant metastasis-free survival (DMFS); (4) type of study: randomized controlled trials (RCTs) or retrospective studies.
Exclusion criteria included the following: (1) reviews, meta-analyses, comments, consensus, animal studies, case reports, and letters; (2) use of preoperative neoadjuvant radiotherapy, and non-R0 resection; (3) data unavailable; and (4) duplicate published trials.
Literature search and screening, data extraction, and quality assessment were performed independently by two authors, and the results were compared. If there was any disagreement, a third reviewer was consulted to reach a consensus.
Data extraction
The following information was extracted from each study, including first author, year of publication, country, research design, study group, and control group (sample size, age, gender, stage, lymph node status, pathological category), intervention (radiotherapy technique and dose, target area, and chemotherapy), follow-up time, and survival data [including hazard ratio (HR) values and 95% confidence intervals (CIs) for OS, DFS, LRFS, and DMFS]. If the HR value and 95% CI data were provided explicitly in the original article, they were extracted directly. Otherwise, they were extracted from the Kaplan–Meier survival plots using Engauge Digitizer version 10.8 (StataCorp LLC, US).
Quality assessment
The Cochrane risk of bias tool was employed to assess the quality of RCT studies and the risk of bias, including the following aspects: (1) random sequence generation; (2) allocation concealment; (3) blinding of participants and personnel; (4) blinding of outcome assessors; (5) incomplete outcome data; (6) selective outcome reporting; and (7) other sources of bias. 20 Each item was given a rating of ‘high’, ‘low’, or ‘unclear’. Data generated by RevMan version 5.4 (The Cochrane Collaboration, 2020) provided a summary assessment of the risk of bias. Retrospective studies (non-RCTs) were evaluated for quality using the Newcastle–Ottawa Scale (NOS), which consists of three major components, namely, subject selection, comparability, and exposure.
Data analysis
The extracted survival data were processed and analyzed using Stata SE15 version 15.1 (Stata Corporation, College Station, TX, United States). The combined HR and its 95% CI were calculated as the effect indicators for the efficacy evaluation. Q test and I2 test were adopted to assess the statistical heterogeneity. An I2 value greater than 50% indicated significant heterogeneity and a random-effects model was used. Otherwise, a fixed-effects model was used. Subgroup analyses were performed on study design, radiotherapy technique and dose, combination mode of chemoradiotherapy, and T-stage to explore sources of heterogeneity. A sensitivity analysis was conducted to determine the stability of the results. A p value of <0.05 indicated a statistically significant difference. Funnel plots were used to assess publication bias.
Results
Study selection
A total of 16,265 articles were retrieved, with 9008 duplicates removed, and 190 articles were included in the initial screening. In all, 20 published articles were finally included by reading the full texts, and the specific screening flow chart is shown in Figure 1. Of note, studies based on the SEER database were not included since they did not provide information on the margin status as well as chemotherapy. Two studies were derived from the NCDB database, and the most complete and up-to-date studies were included to avoid data duplication.6,21

Screening flow chart.
Study and patient characteristics
In all, 20 studies13,18,21–38 were finally included after literature screening, including 6 randomized controlled trials and 14 retrospective studies. A total of 6340 patients were enrolled, of which 1972 patients received PORT and 4368 patients did not. The baseline characteristics indicated that participants were predominantly males, multiple or multisite lymph node metastases were common, and the radiotherapy dose range was 30–66 Gy and 1.8–3.0 Gy/d. The basic characteristics of the included studies are shown in Tables 1–4.
Characteristics of retrospective studies.

AC, adenocarcinoma; DFS, disease-free survival; DMFS, distant metastasis-free survival; LRFS, local recurrence-free survival; NA, not available; NOS, Newcastle–Ottawa Scale; OS, overall survival; PORT, postoperative radiotherapy; RS, retrospective cohort study; SCC, squamous cell carcinoma.
Characteristics of randomized controlled trial studies.

DFS, disease-free survival; DMFS, distant metastasis-free survival; LRFS, local recurrence-free survival; NA, not available; NOS, Newcastle–Ottawa Scale; OS, overall survival; PORT, postoperative radiotherapy; RCT, randomized controlled trial; SCC, squamous cell carcinoma.
Summary of radiotherapy and chemotherapy of included retrospective studies.
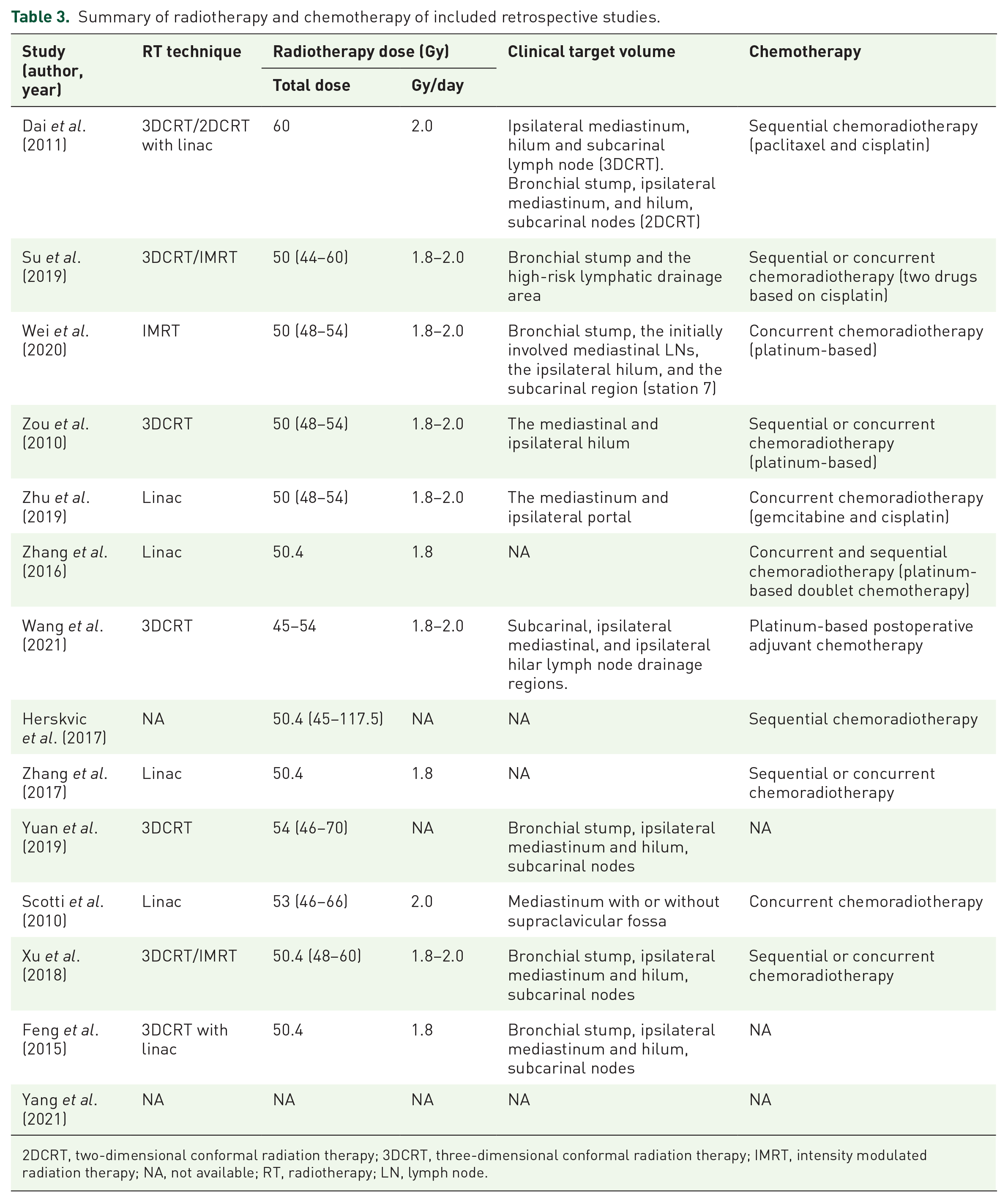
2DCRT, two-dimensional conformal radiation therapy; 3DCRT, three-dimensional conformal radiation therapy; IMRT, intensity modulated radiation therapy; NA, not available; RT, radiotherapy; LN, lymph node.
Summary of radiotherapy and chemotherapy of included randomized controlled trial studies.

2DCRT, two-dimensional conformal radiation therapy; 3DCRT, three-dimensional conformal radiation therapy; IMRT, intensity modulated radiation therapy; NA, not available; RT, radiotherapy.
Quality assessment
According to the assessment by the Cochrane instrument, most studies were considered at low risk of bias, four studies24,31,32,39 were unclear on the risk of allocation concealment, one study 23 was unclear on the risk of blinding of participants and personnel and blinding of outcome assessors, and four studies23,24,32,33 were unclear on the risk of selective outcome reporting. For non-RCT studies, the NOS quality scores ranged from 7 to 9, and all studies were rated as of ‘high quality’. The results of the methodological quality assessment of the included studies are presented in the Supplemental Materials.
Efficacy outcomes
OS was reported in all studies, and the heterogeneity test suggested that there was no significant heterogeneity among studies (I2 = 40.0%), and a fixed-effects model was therefore adopted. PORT significantly improved OS compared with the non-PORT group [HR = 0.77, 95% CI: 0.71–0.84, p < 0.05, Figure 2(a)]. Eight studies reported DFS and LRFS, respectively, and significant improvements in DFS [HR = 0.72, 95% CI: 0.63–0.82, p < 0.05, Figure 2(b)] and LRFS [HR = 0.63, 95% CI: 0.52–0.76, p < 0.05, Figure 2(c)] were observed in the PORT group, with no significant heterogeneity among studies (I2 = 44.1% and 36.1%). Four studies reported DMFS, and there was no significant difference in improving DMFS between the two groups [HR = 0.86, 95% CI: 0.71–1.05, p > 0.05, Figure 2(d)] as shown in Figure 2.

HR forest plots of OS, DFS, LRFS, and DMFS for the included studies. (a) OS. (b) DFS. (c)LRFS. (d) DMFS.
Subgroup analyses
We performed subgroup analyses of OS by study type, radiotherapy technique and dose, combination mode of chemoradiotherapy (sequential or concurrent), and T-stage of disease. The results showed that significantly improved OS in patients was observed in the retrospective study group (HR = 0.75, 95% CI: 0.69–0.82, p < 0.05) compared with the RCT study group (HR = 0.87, 95% CI: 0.71–1.07, p > 0.05) as shown in Figure 3(a). Advantages in improving OS were observed in subgroups of T1–3 (HR = 0.71, 95% CI: 0.63–0.81, p < 0.05) and T1–4 (HR = 0.82, 95% CI: 0.73–0.93, p < 0.05) as shown in Figure 3(b). Compared with the subgroup without adjuvant chemotherapy, significantly improved OS in patients was observed in the sequential postoperative chemoradiotherapy group (HR = 0.79, 95% CI: 0.70–0.90, p < 0.05) and postoperative concurrent chemoradiotherapy group (HR = 0.73, 95% CI: 0.60–0.90, p < 0.05) or a subgroup with both sequential and concurrent chemoradiotherapy (HR = 0.75, 95% CI: 0.62–0.90, p < 0.05) as shown in Figure 3(c). The modern radiotherapy techniques represented by linear accelerators (HR = 0.74, 95% CI: 0.66–0.82, p < 0.05) had obvious advantages in improving OS over outdated radiotherapy techniques such as cobalt as shown in Figure 3(d). Compared with the subgroup with radiotherapy dose <50 Gy (HR = 0.78, 95% CI: 0.54–1.14, p > 0.05), the subgroup with radiotherapy dose ⩾50 Gy (HR = 0.74, 95% CI: 0.64–0.86, p < 0.05) also showed a significant advantage in improving OS as shown in Figure 3(e). Furthermore, we also found that in the subgroups by study type and radiotherapy techniques, the I2 of each subgroup was less than 50%, indicating that the two may be the main sources of study heterogeneity. In terms of radiotherapy dose, combined mode of chemoradiotherapy, and T-stage of disease, there were still subgroups with I2 greater than 50%, indicating that they were not clear sources of heterogeneity.

HR forest plot of OS based on subgroup analyses. (a) study type. (b) T-stage of disease. (c) combination mode of chemoradiotherapy. (d) radiotherapy technique. (e) radiotherapy dose.
Publication bias and sensitivity analysis
Sensitivity analysis by removing each study, in turn, revealed no significant changes in the recalculated combined effect sizes, indicating that the results of this study were relatively stable and there were no outlier studies that significantly affected the overall results. The funnel plots showed relative symmetry with insignificant publication bias among studies. The results of the publication bias and sensitivity analysis of the included studies are presented in Supplemental Figures S1–S4.
Discussion
Patients with completely resected stage N2 NSCLC are among the heterogeneous population with a variety of clinicopathologic features and poor prognosis and low survival rate even after complete surgical resection and POCT. Early radiotherapy techniques cause cardiac toxicity due to adverse events, which may offset the local control benefits of PORT to some extent, making it difficult to accurately reflect the value of PORT. With the wide application of linear accelerators and the emergence of technologies such as three-dimensional conformal radiation therapy (3DCRT) and intensity-modulated radiation therapy (IMRT), radiotherapy techniques have gradually become more precise and have reduced damage to normal tissues. 40 However, previous studies held inconsistent views on the role of PORT with a lack of information on high-risk factors, radiotherapy and chemotherapy, etc.5,15,41 Currently, there is insufficient evidence on whether patients with completely resected stage N2 NSCLC derive a survival benefit from PORT. Therefore, this study provides an updated and more comprehensive data summary to assess the overall efficacy of PORT for completely resected stage N2 NSCLC, identify and validate high-risk patients who would benefit most from PORT as well as information on chemoradiotherapy, thereby providing reliable guidance for clinical practice and future research.
With a total of 20 studies included, the results indicated that PORT improved OS in completely resected stage N2 NSCLC, and also showed significant improvements in LRFS and DFS. For completely resected stage N2 NSCLC, PORT may yield better survival outcomes, which is consistent with the meta-analysis results of Zhang et al. 5 but different from the recent findings of Lei et al. 15 We explored the following points to analyze and explain the survival outcomes with advantages.
First, improved survival outcomes may be secondary to better patient selection. We selected patients who underwent complete surgical resection, and the prognosis of patients receiving R0 resection was generally better than those receiving incomplete resection. Studies involving neoadjuvant therapy were excluded, including the Lung-ART trial, to better ensure the baseline homogeneity between the PORT and non-PORT groups, which distinguishes this paper from other meta-analyses. Neoadjuvant therapy is often applied to N2 patients with well-defined imaging. This study included patients who were not suspected preoperatively but were confirmed N2 positive postoperatively. Furthermore, the retrospective study group was more pronounced in terms of survival benefit, while the positive effect of PORT in RCT studies was not significant. Retrospective studies were subject to some bias in the selection of patients and extraction of data. Given the early initiation, long time span, excessive toxicity, and non-cancer-related deaths associated with these RCTs, combined with the need to obtain more chemoradiotherapy and baseline data, we retained all research types of studies.
Second, the continuous improvement and refinement of radiotherapy techniques contribute to the survival benefit. We included more recent studies which often cover the latest radiotherapy techniques, and performed subgroup analyses by radiotherapy techniques and radiotherapy doses. As in the previous studies, 41 modern radiotherapy techniques (using only linear accelerators) provided a survival advantage with improved OS and LRFS over outdated radiotherapy techniques including cobalt-60. Compared with 3DCRT, IMRT has been reported to have a lower incidence of severe pneumonia and cardiac toxicity.26,42 In this study, the differences between IMRT and 3DCRT were not evaluated as most studies failed to explain the linear accelerator-related technologies. As for radiotherapy doses, most of the included studies used doses of 50 Gy and above, and subgroup analysis showed that increasing radiotherapy doses could improve the therapeutic effect of PORT. Although high radiotherapy doses may result in more favorable local control, the high toxic response and treatment tolerability caused thereby still need to be fully considered. There is a lack of data on toxic reactions, and a trade-off in radiotherapy doses needs to be explored through a large number of future prospective studies.
Furthermore, this discrepancy may be because most of the included cases underwent POCT. With the maturity of systemic treatment options for NSCLC, POCT has become the standard of care for patients with lymph node-positive NSCLC after surgery. 27 Studies have shown a trend toward improved DFS and OS in patients when PORT is performed on the basis of POCT, 43 which is consistent with our results that an OS benefit was found from performing POCT in the subgroup analysis. However, the addition of adjuvant chemotherapy may also bring about more PORT-related toxic reactions, and previous studies have drawn different conclusions regarding concurrent or sequential chemoradiotherapy. Several prospective clinical trials have confirmed that concurrent chemoradiotherapy has a greater survival benefit than sequential chemoradiotherapy for completely resected stage N2 NSCLC. 44 However, patients treated with postoperative concurrent chemoradiotherapy have a higher probability of grade 3 adverse events, 45 and the toxicity of concurrent chemoradiotherapy may offset the benefits of PORT. Other studies have shown that the use of complementary sequential CRT can significantly improve the survival rate 46 and has the advantage of reducing toxicity 47 compared with concurrent chemoradiotherapy. We performed a subgroup analysis of the chemotherapy sequence, and the results showed that the survival benefit of PORT after concurrent chemoradiotherapy was similar to that after sequential chemoradiotherapy, which was consistent with the results of the literature. 48
Despite many studies with negative results in recent years, many scholars believe that some patients can benefit from PORT,35,39 and the assessment of the benefit of PORT should be individualized. Multiple pN2 lymph node metastases have been reported to be an independent risk factor for the development of recurrent metastases and poor prognosis in patients with NSCLC.24,49 The PORT improved OS and DFS in patients with multiple N2 metastases or multiple N2 station involvement compared with the non-PORT group, but there was no significant difference between the two groups for patients with single N2 station involvement.26,50 This evidence suggests that researchers can screen patients who may benefit from PORT based on lymph node involvement. Moreover, patients with lung squamous cell carcinoma have a worse prognosis than patients with lung adenocarcinoma due to insensitivity to chemotherapy and lack of effective targeted therapies [i.e. EGFR tyrosine kinase and anaplastic lymphoma kinase (ALK) inhibitors]. Studies have demonstrated that patients with lung squamous cell carcinoma can derive significant survival benefits from PORT 25 and PORT may be an option for postoperative treatment in patients with N2 lung squamous cell carcinoma. In addition, due to the continuous progression of disease staging, the early literature mostly studied IIIA-N2, with T1, T2, and with or without the T3 stage. Our subgroup analysis showed a more pronounced survival benefit of PORT in patients in the T1–3 or T1–4 subgroups, whereas due to the small sample of patients included in T4, it could not be concluded that PORT had an advantage in patients at the late T stage. In our meta-analysis, the lymph node status and histopathological status of patients in both groups included in the study are described in Table 1, but no statistical conclusions could be drawn as the data from retrospective cohort studies could not be pooled and analyzed, and a large number of future prospective studies based on these characteristics are needed to validate the above results.
Future studies should consider more detailed clinical characteristics and molecular genetic information to accurately identify appropriate patients who will or will not benefit from PORT. When a clinician recommends PORT to a patient with completely resected stage N2 NSCLC, a thorough assessment of the patient’s status is required. With the improvement of modern precision radiotherapy and the addition of chemotherapeutic, targeted, and immunotherapeutic agents, the future of PORT for patients with completely resected stage N2 NSCLC may be further improved.
This study also has some limitations: (1) The data from the included retrospective studies have inherent limitations that may produce selective bias or other potential bias and more prospective randomized controlled trials are required to validate the results in the future. 2 Some of the studies provided incomplete data, especially information related to radiotherapy and chemotherapy, which inevitably leads to inconclusive and unreliable conclusions. 3 Subgroup analysis based on the baseline characteristics of patients (e.g. gender, age, histopathology, lymph node status) could not be performed due to the lack of individual study data, which may affect the extrapolation of results. 4 The Tumor Node Metastasis (TNM) staging of lung cancer has been revised in recent years, and patients with stage III N2 as currently defined may not be the same population as defined in the past, but we have used part of the obsolete data, which may affect the reliability of the results. 5 The proportion and regimen of combined POCT were inconsistent between the two groups of patients in some studies, which may have led to the influence of baseline factors besides PORT on outcomes.
Conclusions
The results of this study suggest that PORT may provide better local recurrence control and survival benefit in the postoperative treatment of patients with completely resected stage N2 NSCLC, and may be included in the postoperative treatment options. Nevertheless, this conclusion needs to be further confirmed by more prospective studies based on modern precision radiotherapy techniques in the future, and long-term survival needs to be observed in future follow-ups.
Supplemental Material
sj-docx-1-taj-10.1177_20406223231195622 – Supplemental material for Effect of postoperative radiotherapy on survival in patients with completely resected and pathologically confirmed stage N2 non-small-cell lung cancer: a systematic review and meta-analysis
Supplemental material, sj-docx-1-taj-10.1177_20406223231195622 for Effect of postoperative radiotherapy on survival in patients with completely resected and pathologically confirmed stage N2 non-small-cell lung cancer: a systematic review and meta-analysis by Lin Wang, Wenyu Chen, Xiaofei Xu, Wenbo Chen, Derong Bao, Ye Zhang and Yufen Xu in Therapeutic Advances in Chronic Disease
Supplemental Material
sj-docx-2-taj-10.1177_20406223231195622 – Supplemental material for Effect of postoperative radiotherapy on survival in patients with completely resected and pathologically confirmed stage N2 non-small-cell lung cancer: a systematic review and meta-analysis
Supplemental material, sj-docx-2-taj-10.1177_20406223231195622 for Effect of postoperative radiotherapy on survival in patients with completely resected and pathologically confirmed stage N2 non-small-cell lung cancer: a systematic review and meta-analysis by Lin Wang, Wenyu Chen, Xiaofei Xu, Wenbo Chen, Derong Bao, Ye Zhang and Yufen Xu in Therapeutic Advances in Chronic Disease
Supplemental Material
sj-docx-3-taj-10.1177_20406223231195622 – Supplemental material for Effect of postoperative radiotherapy on survival in patients with completely resected and pathologically confirmed stage N2 non-small-cell lung cancer: a systematic review and meta-analysis
Supplemental material, sj-docx-3-taj-10.1177_20406223231195622 for Effect of postoperative radiotherapy on survival in patients with completely resected and pathologically confirmed stage N2 non-small-cell lung cancer: a systematic review and meta-analysis by Lin Wang, Wenyu Chen, Xiaofei Xu, Wenbo Chen, Derong Bao, Ye Zhang and Yufen Xu in Therapeutic Advances in Chronic Disease
Supplemental Material
sj-tif-4-taj-10.1177_20406223231195622 – Supplemental material for Effect of postoperative radiotherapy on survival in patients with completely resected and pathologically confirmed stage N2 non-small-cell lung cancer: a systematic review and meta-analysis
Supplemental material, sj-tif-4-taj-10.1177_20406223231195622 for Effect of postoperative radiotherapy on survival in patients with completely resected and pathologically confirmed stage N2 non-small-cell lung cancer: a systematic review and meta-analysis by Lin Wang, Wenyu Chen, Xiaofei Xu, Wenbo Chen, Derong Bao, Ye Zhang and Yufen Xu in Therapeutic Advances in Chronic Disease
Supplemental Material
sj-tif-5-taj-10.1177_20406223231195622 – Supplemental material for Effect of postoperative radiotherapy on survival in patients with completely resected and pathologically confirmed stage N2 non-small-cell lung cancer: a systematic review and meta-analysis
Supplemental material, sj-tif-5-taj-10.1177_20406223231195622 for Effect of postoperative radiotherapy on survival in patients with completely resected and pathologically confirmed stage N2 non-small-cell lung cancer: a systematic review and meta-analysis by Lin Wang, Wenyu Chen, Xiaofei Xu, Wenbo Chen, Derong Bao, Ye Zhang and Yufen Xu in Therapeutic Advances in Chronic Disease
Supplemental Material
sj-tif-6-taj-10.1177_20406223231195622 – Supplemental material for Effect of postoperative radiotherapy on survival in patients with completely resected and pathologically confirmed stage N2 non-small-cell lung cancer: a systematic review and meta-analysis
Supplemental material, sj-tif-6-taj-10.1177_20406223231195622 for Effect of postoperative radiotherapy on survival in patients with completely resected and pathologically confirmed stage N2 non-small-cell lung cancer: a systematic review and meta-analysis by Lin Wang, Wenyu Chen, Xiaofei Xu, Wenbo Chen, Derong Bao, Ye Zhang and Yufen Xu in Therapeutic Advances in Chronic Disease
Supplemental Material
sj-tif-7-taj-10.1177_20406223231195622 – Supplemental material for Effect of postoperative radiotherapy on survival in patients with completely resected and pathologically confirmed stage N2 non-small-cell lung cancer: a systematic review and meta-analysis
Supplemental material, sj-tif-7-taj-10.1177_20406223231195622 for Effect of postoperative radiotherapy on survival in patients with completely resected and pathologically confirmed stage N2 non-small-cell lung cancer: a systematic review and meta-analysis by Lin Wang, Wenyu Chen, Xiaofei Xu, Wenbo Chen, Derong Bao, Ye Zhang and Yufen Xu in Therapeutic Advances in Chronic Disease
Footnotes
Acknowledgements
Data curation: Ye Zhang, Lin Wang; Funding acquisition: Yufen Xu, Wenyu Chen; Project administration: Yufen Xu, Ye Zhang, Wenyu Chen; Resources: Yufen Xu, Ye Zhang, Lin Wang; Software: Ye Zhang, Lin Wang; Supervision: Yufen Xu, Ye Zhang, Wenyu Chen; Validation: Yufen Xu, Ye Zhang, Wenyu Chen; Visualization: Yufen Xu, Ye Zhang, Wenyu Chen.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.