
Abstract
Introduction:
High blood pressure in midlife is an established risk factor for cognitive decline and dementia but less is known about the impact of raised blood pressure on cognition in childhood and early adulthood.
Method:
We systematically reviewed and quantified the existing evidence base relating to blood pressure in early life and subsequent cognitive performance. Medline, Embase, PsycINFOo, Scopus, and Web of Science were searched from inception to July 2020. We included longitudinal cohort and case–control studies involving participants aged 0–40 years with a baseline and at least one follow-up blood pressure assessment alongside at least one measure of cognition, occurring at the same time as, or subsequent to blood pressure measures. Risk of bias was assessed independently by two reviewers. PROSPERO registration CRD42020214655.
Results:
Of a total of 5638 records identified, three cohort and two case–control studies were included with ages ranging from 3 to early 30s. Repeated blood pressure measurements averaged over 25 years or cumulative blood pressure in the 25–30 years prior to assessment of cognitive function were associated with poorer cognitive performance in the two largest cohort studies. The smallest cohort study reported no evidence of an association and the results from the two case–control studies were contradictory. All studies were at risk of bias.
Conclusion:
Overall, the evidence in this area is lacking and study quality is mixed. Our review highlights an urgent need for studies evaluating the potential for a relationship between raised blood pressure and poorer cognition in early life given the potential for possible risk reduction if such a relationship exists.
Introduction
Over the last 40–50 years, a large literature has developed linking raised blood pressure to an increased risk of cognitive decline or dementia in later life. Leading examples of early work include data from Sweden showing those who developed dementia at age 79–85 had higher systolic and diastolic pressures at age 70 1 and from the Honolulu Asia Aging Study where systolic pressures of greater than 139 mmHg and or diastolic pressures over 89 mmHg in midlife were associated with over twofold increase in risk of incident dementia in those never treated for hypertension. 2 This inevitably prompted work to evaluate the impact of blood pressure lowering as a therapeutic strategy for dementia risk reduction, and in so doing, has highlighted the complexity of the relationships between blood pressure and cognition, relationships that we are still trying to unravel.3–5
Collating the evidence has shown that these relationships are stronger when the raised blood pressure is experienced in midlife (40–65 years) and that the evidence in later life is more mixed – perhaps also more confounded.3,6,7 Blood pressure also evolves across the life-course rising until midlife after which diastolic pressure begins to fall. 8 In addition, as the clinical trials of antihypertensives have shown, our understanding of what is an acceptable or goal blood pressure has changed over time.9,10 Finally, blood pressure, of course, is also continuously present; unlike some of the other established dementia risk factors (e.g. smoking) we cannot remove it.
The gradual nature by which dementia pathology is accrued over decades, 11 the lifelong presence of blood pressure and evidence from the cardiovascular arena of in utero or early life exposures linked to later life risk12,13 point us towards needing a lifelong understanding of the impact of the blood pressure cognition relationship. 14 We need to begin to help develop this understanding and to highlight research gaps in the current evidence base. Our aim was to systematically review the literature, focusing on the age group that has been largely omitted so far, those aged 0–40 years at the time of blood pressure measurement.
Methods
Standard systematic review methodology was used. Databases Medline, Embase, PsycINFO®, Scopus, and Web of Science were searched from inception to 01 July 2020 with search terms including ‘cognition’, ‘neuropsychology’, ‘attention’, ‘memory’, ‘language’, ‘processing speed’, ‘executive function’, ‘visuo-spatial ability’ and ‘blood pressure’, ‘hypertension’ (see online supplement, for example, search strategy for PsycINFO). The full search strategy was developed in consultation with a university research librarian. Title, abstract and full-text screening were carried out by two independent reviewers (K.L., R.P.) with any disagreement resolved by discussion. The reference lists of the publications examined at the full-text stage were also examined for additional articles. Data including the first author`s surname, publication year, country(ies) where sample was obtained, recruitment source, participant demographics, sample size at baseline and follow-up assessments, duration of follow-up, details of blood pressure measurement, blood pressure value or classification, cognitive or neuropsychological test administered and result, statistical analyses conducted, variables adjusted for, main outcomes, and relevant summary statistics were extracted into predesigned forms and checked by a third reviewer (Y.X.). Where multiple models with different adjustment for confounders were available, the most adjusted model was extracted. Studies were included if they were of longitudinal prospective design (including cohort and case–control studies) with a baseline, at least one follow-up assessment of blood pressure and at least one measure of cognition, using recognised quantitative cognitive or neuropsychological measures, occurring at the same time as, or after, follow-up assessment of blood pressure. Where there were multiple publications from the same population the reports with the longest follow-up and largest sample size with appropriate blood pressure and cognitive measures were selected. Animal studies were excluded as were human studies where baseline and at least one follow-up blood pressure assessment were not collected between birth and age 40. A wide age range was used to ensure that all potential data were captured. An upper age limit of 40 years was selected based on the widely used definition of midlife in dementia risk factor epidemiology as between 40 and 65 years. Studies on prenatal or pregnancy specific blood pressure were excluded as systematic reviews have already focused in these areas.15,16 Randomised controlled trials of phase 0–2 inclusive, single case studies, systematic reviews, meta-analyses, editorials, commentaries, protocols, conference papers, or theses were excluded. Studies that included participants with conditions that could potentially influence the relationships under investigation, such as acute cardiovascular disease, immunological disorders, metabolic disorders, cancer, neurological and psychiatric conditions, head trauma, alcohol use disorders and substance disorders, were excluded. Also excluded were studies involving conditions or interventions known to have an effect on cognition (e.g. pre/postoperative cognitive functioning, anaesthetics, educational interventions, lead or chemical exposure). To evaluate the potential for aspects of the study design, assessment or follow-up to have exposed the study results to risk of bias this was assessed independently by two reviewers (K.L., R.P.) using key factors selected from the Critical Appraisal Skills Programme checklists for evaluating case–control and cohort studies. 17 The use of a focused research question, appropriate methodology, measurement of exposure and outcome, attrition, confounding and reporting were considered and a categorical judgement made of low, moderate or high potential risk of bias. A formal scoring system was not used as this can lead to a loss of subtlety. Any disagreement between reviewers was resolved by discussion.
The principles of the PRISMA statement were followed and the protocol was registered with PROSPERO: registration CRD42020214655.
Results
Searches found 5638 records reduced to 5316 after duplicates were removed. Title and abstract screening removed a further 5294 with 22 articles assessed at full-text stage of which 16 were excluded as ineligible (Supplementary Text 2), leaving 6 included articles18–23 reporting on 5 studies (2 articles21,22 were from 1 study) (Figure 1).

PRISMA flow chart.
Table 1 shows the characteristics of the included studies. The five studies were carried out in the United States,18,19,21,22 Finland 23 and the Seychelles, 20 two were case–control studies comparing groups with hypertension (cases) to those without hypertension (matched controls)18,19 with populations of 150 19 and 82, 18 respectively. The remaining three studies were cohort studies of 580, 20 2026 23 and 338121,22 participants. There were no studies reporting on the very young (ages 0–2); however, the ages of those included ranged from 3 23 to those in their 30s. 18 Overall follow-up times ranged from 1 19 to 25–30 years21–23 with all studies including both male and female participants. Two of the studies did not report details of the procedure used for blood pressure measurement,18,23 two studies provided comprehensive details19,21,22 and another study leveraged data collected in school surveys. 20 All studies used some level of neuropsychological battery for cognitive testing.
Characteristics of the included studies.

DBP, diastolic blood pressure; MAP, mean arterial pressure; SBP, systolic blood pressure; SD, standard deviation; SE, standard error.
Case–control studies
Both case–control studies assessed change in cognitive function. Miller et al. used analysis of variance to compare overall cognitive change over 15 months combining battery of sensory-perceptual, cognitive and psychomotor test performance and found that hypertensive cases with treated hypertension showed a significantly improved overall cognitive function z score, whereas in those who were untreated declined, and the controls (normotensive group) showed no change (Table 2). 18 In contrast, Lande et al. 19 with a year of follow-up used analysis of covariance adjusting for key confounders and reported both subjects with hypertension (regardless of the effectiveness of antihypertensive therapy) and normotensive controls significantly improved in scores of subtests of the Rey Auditory Verbal Learning Test (RAVLT), Grooved Pegboard Test and Delis–Kaplan Executive Function System Tower Test. However, the control group also significantly improved compared with the hypertensive group on the Wechsler Intelligence Scale for Children-Fourth Edition Spatial Span Forward. 19
Cognitive testing and results.

DBP, diastolic blood pressure; MAP, mean arterial pressure; SBP, systolic blood pressure.
Cohort studies
The cohort studies reported on longitudinal blood pressure exposure but only assessed cognition at a single time point rather than measuring change. For the two studies with longer follow-up, the Coronary Artery Risk Development in Young Adults (CARDIA)21,22 and the Young Finn’s study, 23 blood pressure was collected repeatedly throughout follow-up and cognition collected after around 25–30 years of follow-up. For the CARDIA study, blood pressure averaged over 25-year follow-up was categorised as poor, intermediate and ideal. 21 Trend tests found a relationship between category of mean blood pressure and performance on the Digit Symbol Substitution Test (DSST) speed, a Stroop test interference score (calculated by subtracting score on subtest II from subtest III) and the delayed recall trial of the RAVLT such that those with higher pressures performed more poorly than those with lower pressures. 21 Additional analyses using cumulative blood pressure exposures reported similar results with poorer performance on the DSST speed, Stroop test interference score and RAVLT delayed recall associated with a greater area under the curve (AUC) of systolic blood pressure and poorer performance on the DSST speed and Stroop test interference score associated with greater AUC of diastolic blood pressure. 22 The Young Finn’s study also reported on cumulative blood pressure exposure overall (from 6 to 24 years) and by age group, for childhood, adolescence and early adulthood. Overall, they reported that a significant increase in cumulative systolic blood pressure (per ~6 mmHg) associated with one standard deviation lower performance on a rapid visual processing test [i.e. the Paired Associate Learning test (PAL)], but no significant findings for spatial working memory or rapid visual information tests. 23 Results on the PAL were similar across the three age groups (6–12, 12–18 and 18–24 years old) and stronger for systolic rather than diastolic pressure but did not always reach statistical significance. 23 The smaller cohort study reported no consistent evidence for an association between blood pressure measured earlier in adolescence (12 and 15 years) and cognitive function assessed at age 17 or 19. 20
Risk of bias
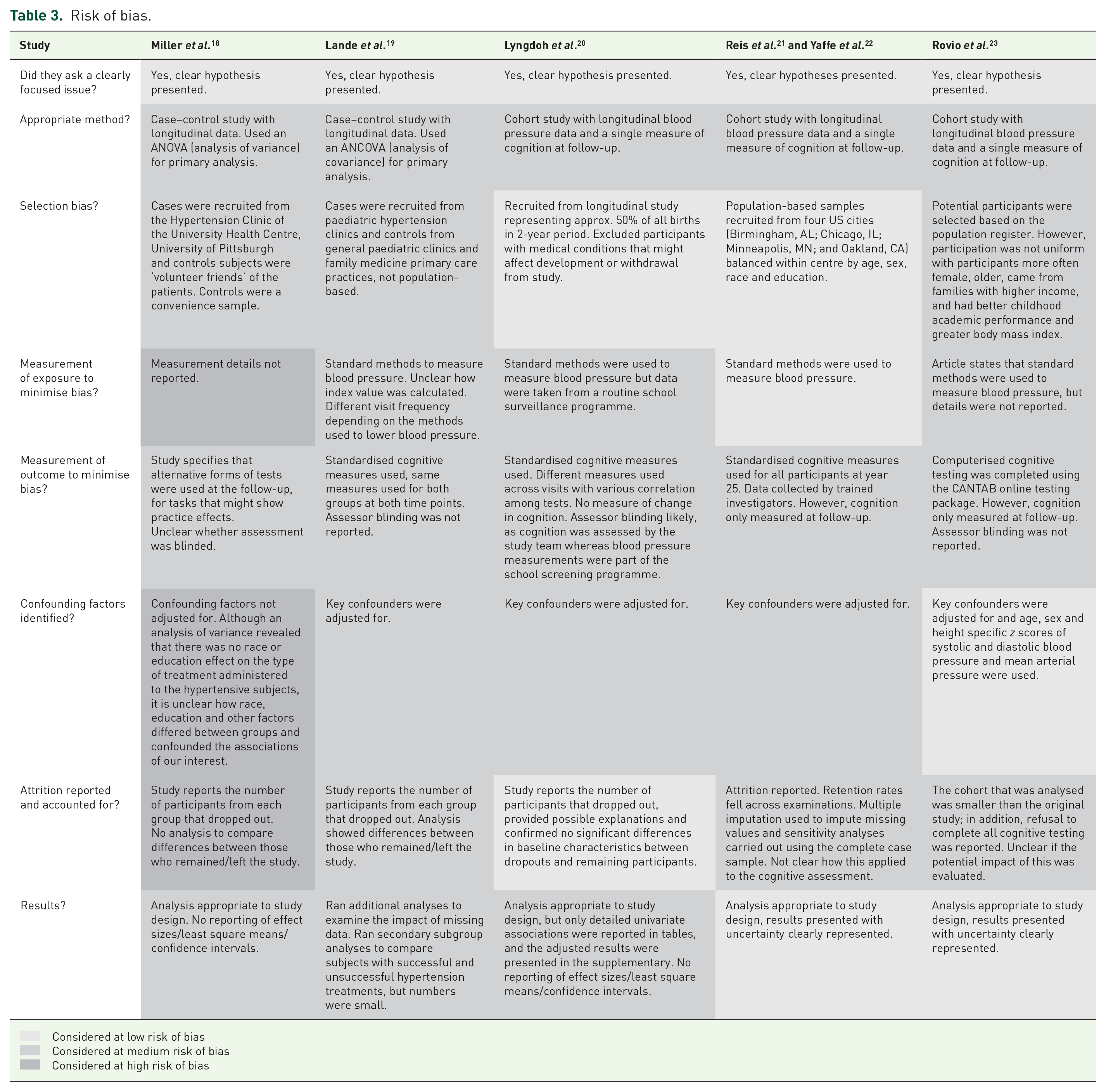
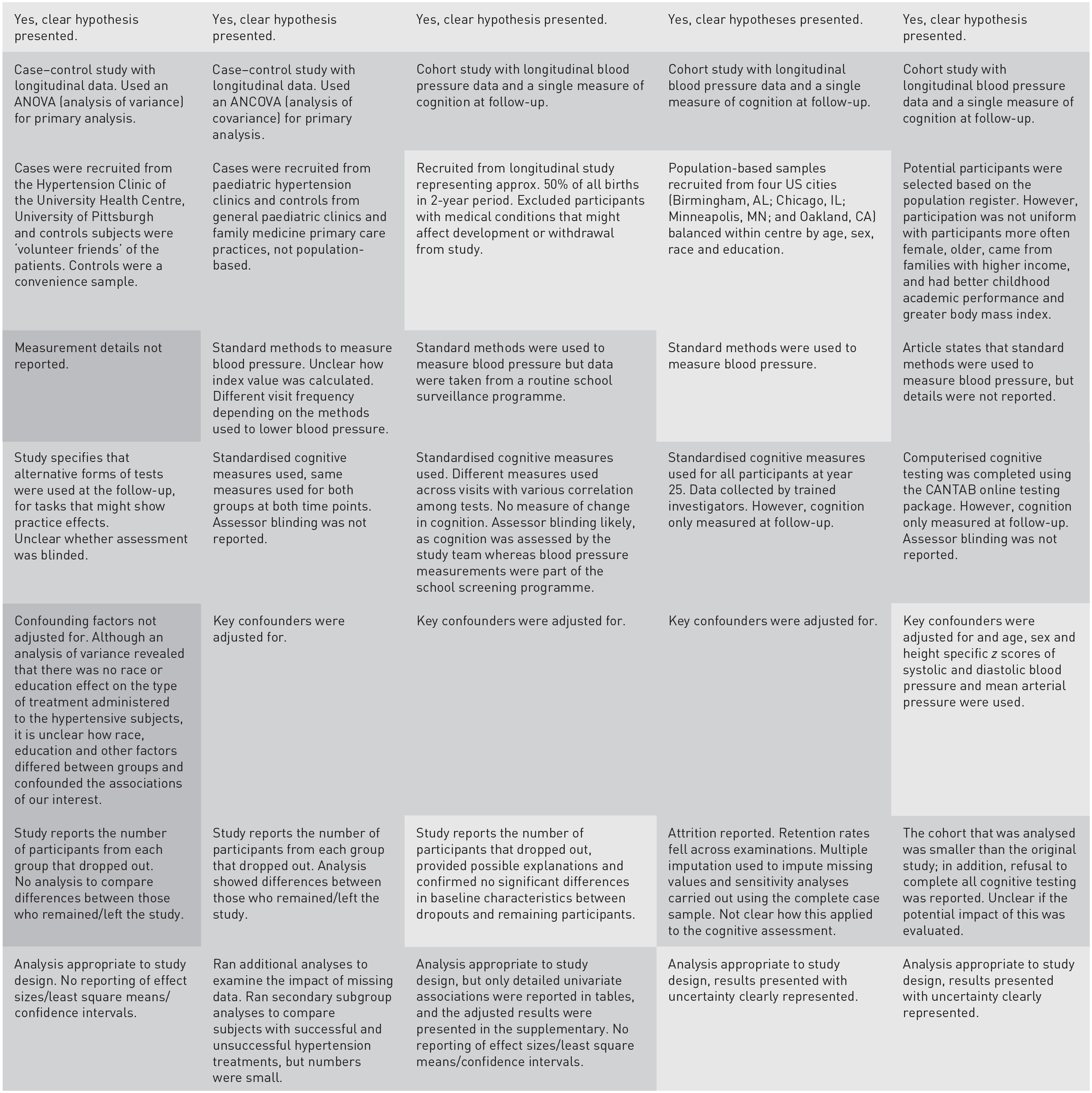
All of the studies were at some risk of bias (Table 3). In general, exposure and outcome measurement was adequate. Blood pressure measurement was reported by the authors as having been completed using standard methods and cognitive testing was by well-validated neuropsychological tests rather than cognitive screening tests. When considering the potential impact of blood pressure on cognition, however, the case–control studies were small and relatively short given the length of time that may be needed to see the impact of blood pressure on cognition, and the cohort studies, although larger and longer, were unable to measure cognitive change. In terms of statistical methods to determine significant cognitive change, the relevant longitudinal studies used adequate methods. When considering all the studies, a minority used demographically corrected blood pressure measures and cognitive scores, and most adjusted for demographic variables within their samples. In this regard, only one study used age-, sex- and height-specific z scores of systolic and diastolic blood pressure and mean arterial pressure and found that the association between blood pressure and cognition did not differ by sex. 20 This is particularly relevant in diverse populations where the use of adjustment with the study population may mask important demographic differences.
Risk of bias.
 Considered at low risk of bias
Considered at low risk of bias
 Considered at medium risk of bias
Considered at medium risk of bias
 Considered at high risk of bias
Considered at high risk of bias
Discussion
A systematic review of the evidence examining the relationships between raised blood pressure and cognitive function in early life is indicative. Studies tentatively indicate the potential for the relationship between higher blood pressure and poorer cognition earlier than midlife. Nevertheless, the evidence base is not yet strong enough to provide unequivocal evidence for, or even against, a link between higher early-life blood pressures and cognition.
Limitations in the current evidence base include a lack of data with relatively small number of studies, only two of which were able to report on change in cognition and neither of which reported a clear relationship between blood pressure and poorer cognition in their primary analyses. Furthermore, these two studies18,19 are small case–control studies with follow-up durations of 12 and 15 months, attrition at follow-up (not controlled for statistically), assessment of the outcome measures is unblinded and there are small numbers in their analyses leaving them at risk of bias. The larger cohort studies20–23 that have reported in this area were longer and were able to address cumulative blood pressure exposure with interestingly similar results across crucial age groups (e.g. between 6 and 12, 12 and 18 and 18 and 24) 23 but were unable to assess change in cognition meaning that it is impossible to fully understand whether general cognitive competence and other shared risk factors such as socioeconomic status may be driving the associations. The lack of studies in this area also precluded the use of meta-analysis to derive summary estimates and assessment of publication bias.
There are also some limitations in our methods. We used a combination of title and abstract screening, and although we searched the published evidence and the clinical trial registries, we did not include conference abstracts or theses and it is nevertheless possible that we missed relevant grey literature. We also chose to exclude additional reports in population subgroups; however, it should be noted that the CARDIA study in particular has multiple publications examining the relationships between various blood pressure and cardiovascular parameters and cognition.21,22,25,26
Future considerations
While the data to date give some indication that a relationship may be present, we still lack an understanding of when and how such relationships may develop. The sparsity of data and lack of longer-term assessment of cognition and blood pressure at each developmental age is important for several reasons. In particular, without repeat assessment over longer follow-up and a greater breadth of assessment from additional studies we will not be able to quantify whether, when or how relationships between blood pressure and cognition occur.
Careful assessment at different ages is particularly important as cognitive skills develop through childhood, adolescence and early adulthood and blood pressure also changes. While there is evidence from later life cohorts that shows the midlife period as a time when we are susceptible to the impact of raised blood pressure increasing risk of dementia in later life, we lack understanding of whether there are also developmental periods prior to age 40 during which we are susceptible. Assessing cognitive function using developmentally relevant testing with a focus on the skill sets most pertinent to the developmental age of the population will be important for future research. Furthermore, future, robust longitudinal studies in this area should use optimal statistical methods to measure cognitive change (e.g. mixed-effect models). The heterogeneity in cognitive outcomes also suggests that this field of research may require some level of harmonisation in the selection of cognitive domains. Furthermore, the use of normative data on the selected neuropsychological test scores at least at baseline may assist in determining whether the control group and the clinical group perform within expectations. This is important because poor performance is the number one factor associated with cognitive change. 27 Alongside this, evaluating the impact of raised blood pressure on cognition over time requires disentangling the roles of blood pressure trajectory, absolute blood pressure level and expected blood pressure for each age group.
In addition, without repeated and larger studies in similar age populations with robust methods, we will continue to lack the statistical power to disentangle relationships driven by population characteristics or external factors. For example, there are major differences between sexes in terms of brain development and blood pressure.28,29 Therefore, it would be advisable that this demographic characteristic be correctly represented and systematically analysed. Skilled adjustment and analysis is also needed to take account of other factors that may play a role including underlying issues such as socioeconomic status, race/ethnicity (when relevant, either to due to biological or to historical racial discrimination and related lack of quality in education and social opportunities), lifestyle (including aspects of this that may influence both blood pressure and cognition, e.g. body mass index or obesity) and experience of adversity especially during the childhood years and related mental health sequalae.
It remains a possibility that exposure to elevated blood pressure during childhood, adolescence and early adulthood either as a consequence of or in conjunction with other factors may have a negative impact on cognitive performance with the potential for a subsequent impact on academic and workplace performance.
Blood pressure lowering through lifestyle and pharmacological means is available and (for the latter at least) shows significant promise in protecting cognition in later life stages. Because blood pressure is lifelong, it is also important to develop our understanding of early-life blood pressure impact and trajectory. This review represents the first synthesis of data on the relationship between early-life blood pressure and cognition and highlights a need for additional data to further our understanding. It is too early to say whether we can identify an at-risk population, in childhood or early adulthood, and whether we can intervene to protect cognition earlier in the life-course.
Supplemental Material
sj-docx-1-taj-10.1177_20406223221085111 – Supplemental material for Blood pressure change and cognition in childhood and early adulthood: a systematic review
Supplemental material, sj-docx-1-taj-10.1177_20406223221085111 for Blood pressure change and cognition in childhood and early adulthood: a systematic review by Kurt Lancaster, Ying Xu, Greg Savage, Lucette A. Cysique and Ruth Peters in Therapeutic Advances in Chronic Disease
Footnotes
Acknowledgements
We thank Dr. Jean Peters for her work. No previous presentations of the whole or part of the work presented in the article.
Author contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is supported by the Australian National Health and Medical Research Council (NHMRC) project (APP1160373).
Conflict of interest statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval and consent to participate
Ethical approval was not required for this work.
Availability of data and material
All data is derived from published work.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.