
Abstract
Objective
Few studies have investigated the relationships between high-sensitivity C-reactive protein (hs-CRP) concentration and conventional cardiometabolic markers in young adults. The aim of this study was to characterize the cardiometabolic profile of young adults who are at high cardiovascular risk, according to hs-CRP concentration.
Methods
A cross-sectional study was conducted in 300 young adults (18 to 30 years old) from southern Mexico (n = 150 normal-weight and n = 150 obese). Their circulating lipid and glucose concentrations were measured using colorimetric enzymatic assays, and their hs-CRP, ApoA, and ApoB concentrations were measured using turbidimetric assays.
Results
The most prevalent abnormalities in the participants with high cardiovascular risk, determined using an hs-CRP >28.57 nmol/L, were high waist circumference (85.7%), obesity (83.9%), high low-density lipoprotein-cholesterol (64.3%), low high-density lipoprotein-cholesterol (50%), Apo B in the highest tertile (39.3%), hypertriglyceridemia (35.7%), and high blood pressure (30.4%). In addition, there were strong associations between hs-CRP >28.57 nmol/L and obesity (odds ratio [OR] = 13.9), high waist circumference (OR = 8.0), hypertriglyceridemia (OR = 4.0), high blood pressure (OR = 3.4), hypercholesterolemia (OR = 2.8), and Apo B in the highest tertile (OR = 2.4).
Conclusion
The principal cardiometabolic alterations associated with high cardiovascular risk, determined using hs-CRP, are obesity, dyslipidemia, and high blood pressure in young adults.
Keywords
Introduction
In the last 20 years, there has been an increase in the incidence of cardiovascular disease (CVD) in young adults (18 to 45 years) in developed countries. This has been attributed to the higher prevalence of conventional cardiovascular risk factors, such as obesity, a poor diet, and physical inactivity. 1
In Latin America and the Caribbean, the prevalences of conventional cardiovascular risk factors are similar to those in developed countries: ∼5% for diabetes and ∼30% for obesity. In addition, when the prevalences of high blood pressure, diabetes, and smoking were compared between populations in Latin America and the United States, they were found to be similar. 2 In 2017, CVD was the principal cause of death in Mexico, and the number of deaths from CVD increased by 110% between 1990 and 2017. 3 Furthermore, cardiometabolic risk factors have also been identified from an early age. In a multi-center study of children and adolescents, high prevalences of obesity (11.4%), hypertriglyceridemia (27.7%), and low high-density lipoprotein-cholesterol (HDL-C) concentration (29.5%) were identified. 4 The presence of other conditions, such as dyslipidemia, hyperuricemia, and insulin resistance, increases the risk of CVD. 5 However, most previous studies have focused on adults of ≥40 years old and only a few have evaluated the relationships between these factors and the risk of premature death in adolescents and young adults. 6
In 1997, high-sensitivity C-reactive protein (hs-CRP) was shown to be a predictor of an initial vascular event in healthy individuals, and an increase in its concentration is associated with higher risks of coronary heart disease and cardiovascular morbidity. 7 The Centers for Disease Control and the American Heart Association proposed that hs-CRP concentrations <9.52 nmol/L, between 9.52 nmol/L and 28.57 nmol/L, and >28.57 nmol/L are associated with low, intermediate, and high risks, respectively, of developing CVD. 8
In adults, overweight and obesity have been shown to be associated with high serum hs-CRP concentrations. 9 Previous studies have shown that anthropometric indices of adiposity, such as body mass index (BMI), waist circumference, and waist-hip ratio, correlate with hs-CRP concentration.10,11 However, few studies have addressed the influence of body fat on hs-CRP concentration in young individuals.
Moreover, the young population may also possess subclinical metabolic abnormalities, even if healthy and non-obese, but when their adiposity increases, these cardiometabolic abnormalities increase in prevalence. Fortunately, many cardiometabolic risk factors are modifiable; therefore, it is important to identify these defects early of life, between childhood and young adulthood, as well as to determine their prevalence. Timely identification will allow more effective programs to be established that aim to reduce the prevalences of cardiometabolic risk factors in countries like Mexico, which has a very high prevalence of obesity. Unfortunately, few studies have been conducted in southern Mexico regarding the prevalences of metabolic disorders in any age group, nor have the relationships between systemic inflammation, evaluated using hs-CRP, and metabolic disorders been investigated as cardiovascular risk factors. Therefore, the purpose of the present study was to characterize the cardiometabolic defects present young adults from southern Mexico who are at high cardiovascular risk, as indicated by high hs-CRP concentrations.
Methods
Study participants
We recruited young adults aged 18 to 30 years from the State of Guerrero in southern Mexico, who were allocated to two groups according to their BMI: normal-weight controls (BMI 18.5–24.9 kg/m2) and obese participants (BMI ≥30 kg/m2). 12 The exclusion criteria were the presence of an infectious disease, the use of any medication at the time of the investigation, and an hs-CRP concentration ≥952 nmol/L. 13 The participants were selected through convenience sampling and all gave their written informed consent after the purpose and nature of the study had been explained. Approval for the study was obtained from the Research Ethics Committee of the University of Guerrero (number 11/2018).
Anthropometric and clinical measurements
The body, fat, and muscle masses of the participants were measured in light clothing, without shoes, using a body composition analyzer (MC-780U, Tanita, Arlington Heights, IL, USA) and their heights were measured using a stadiometer (Seca, Hamburg, Germany). Using these measurements, BMI was calculated as body mass/height 2 in kg/m2. Their waist and hip circumferences were measured using a diameter tape (Seca, Hamburg, Germany). High waist circumference was defined using the International Diabetes Federation (IDF) criteria as ≥90 cm for men and ≥80 cm for women. Blood pressure was measured while seated using a blood pressure monitor (HEM-7120, Omron Healthcare Inc, Hoffman Estates, IL, USA) on the left arm after a 10-minute rest. The systolic blood pressure (SBP) and diastolic blood pressure (DBP) were calculated as the means of two readings made at least 10 minutes apart. High blood pressure was defined as a mean SBP ≥130 mmHg and/or a mean DBP ≥85 mmHg, according to the IDF criteria.
Laboratory measurements
A 5-mL venous blood sample was obtained from each participant after at least a 12-hour fast. The serum lipid and glucose concentrations were determined by enzymatic methods using commercially available kits (Spinreact, Barcelona, Spain). Abnormal concentrations were defined as: total cholesterol (TC) ≥5.17 mmol/L, triglycerides (TG) ≥1.69 mmol/L, low-density lipoprotein-cholesterol (LDL-C) ≥2.59 mmol/L, HDL-C ≤1.03 mmol/L in men and ≤1.29 mmol/L in women, and glucose ≥5.55 mmol/L. These values were based on the criteria of the National Cholesterol Education Program Expert Panel on the Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). The serum concentrations of hs-CRP and apolipoproteins A (Apo A) and B (Apo B) were measured by turbidimetric assays on a clinical chemistry analyzer (Mindray BS-200, Shenzhen, China). Cardiovascular risk was determined according to the recommendations of the American Heart Association, in which hs-CRP concentrations of <9.52, 9.52 to 28.57, and >28.57 nmol/L correspond to low, moderate, and high risks of cardiovascular disease, respectively. Apo A and Apo B serum concentrations were analyzed in tertiles, using the lowest tertile as the reference.
Statistical analysis
Categorical data were analyzed using the chi-square test. Normally distributed continuous data were analyzed using Student’s t-test or one-way ANOVA, as appropriate. Non-normally distributed continuous data were analyzed using the Mann–Whitney U-test or the Kruskal–Wallis test, as appropriate. Data are presented as the mean and standard deviation if they were normally distributed and as the median and 25th to 75th percentiles if not. Spearman’s correlation coefficients were computed to evaluate the relationships between hs-CRP concentration and other parameters across the complete sample. Multiple regression analysis was used to determine the odds ratios for hs-CRP with respect to cardiometabolic defects. Statistical analysis was performed using Stata software (V.11, StataCorp, LLC., College Station, TX, USA) and P <0.05 was considered to represent statistical significance.
Results
We recruited 300 young adults (173 women and 127 men), of whom 150 were allocated to the normal-weight group and 150 to the obesity group. Table 1 shows the clinical and biochemical characteristics of the study groups. The obese participants had significantly higher BMI, fat mass, waist and hip circumferences, SBP, DBP, glucose, TC, TG, LDL-C, hs-CRP, and Apo B, but significantly lower HDL-C and Apo A than the controls. The cardiometabolic defects present in the obese group were, in order of prevalence, waist circumference (97.3%), high LDL-C (70.1%), low HDL-C (55.8%), hypertriglyceridemia (41.3%), Apo B in the highest tertile (32.7%), high blood pressure (28%), and hypercholesterolemia (20%).
Clinical and biochemical characteristics of each study group.
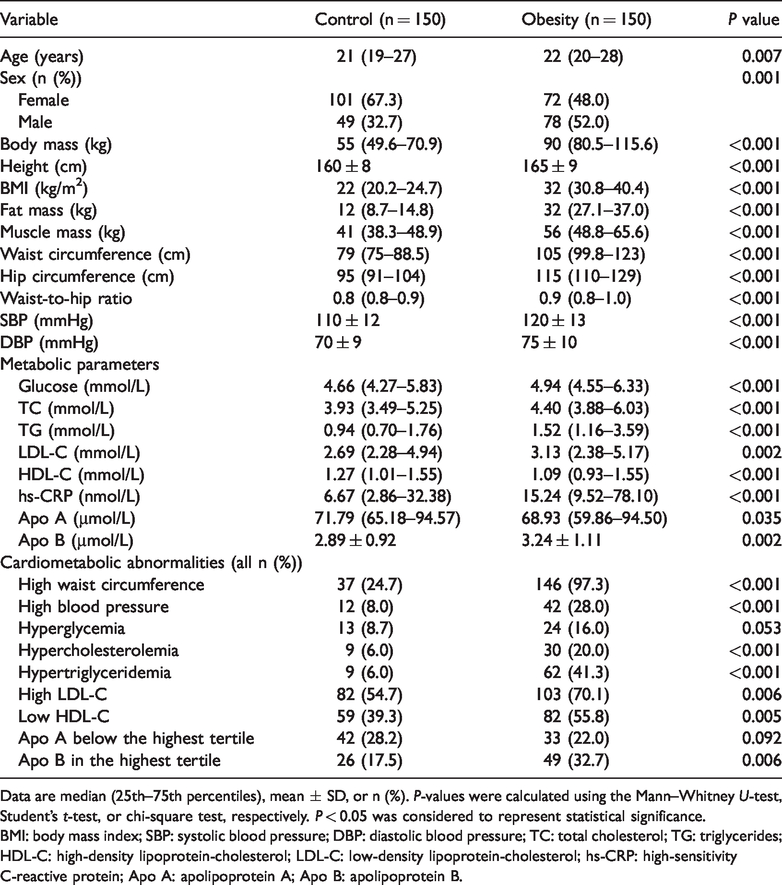
Data are median (25th–75th percentiles), mean ± SD, or n (%). P-values were calculated using the Mann–Whitney U-test, Student’s t-test, or chi-square test, respectively. P < 0.05 was considered to represent statistical significance.
BMI: body mass index; SBP: systolic blood pressure; DBP: diastolic blood pressure; TC: total cholesterol; TG: triglycerides; HDL-C: high-density lipoprotein-cholesterol; LDL-C: low-density lipoprotein-cholesterol; hs-CRP: high-sensitivity C-reactive protein; Apo A: apolipoprotein A; Apo B: apolipoprotein B.
Table 2 shows an analysis of the data in each group, according to cardiovascular risk, determined using hs-CRP concentration. The obese participants had higher BMI (P = 0.006), fat mass (P = 0.011), muscle mass (P = 0.012), waist circumference (P = 0.024), systolic blood pressure (P = 0.042), and LDL-C (P = 0.019) in the high- and intermediate-risk groups than in the low-risk group.
Clinical and biochemical characteristics of the participants after their categorization according to cardiovascular risk.

Data are median (25th–75th percentiles), mean ± SD, or n (%). P-values were calculated using the Kruskal-Wallis test, one-way ANOVA, or chi-square test, respectively. P < 0.05 was considered to represent statistical significance.
hs-CRP concentrations of <9.52, 9.52 to 28.57, and >28.57 nmol/L were accepted as indicating low, moderate, and high risks of cardiovascular disease, respectively.
BMI: body mass index; SBP: systolic blood pressure; DBP: diastolic blood pressure; TC: total cholesterol; TG: triglycerides; HDL-C: high-density lipoprotein-cholesterol; LDL-C: low-density lipoprotein-cholesterol; Apo A: apolipoprotein A; Apo B: apolipoprotein B.
The correlations between hs-CRP and selected variables are shown in Table 3. Among the obese participants, there were moderate correlations with BMI (r = 0.29, P < 0.001), fat mass (r = 0.28, P < 0.001), waist circumference (r = 0.21, P < 0.001), waist-to-hip-ratio (r = 0.17, P = 0.039), and LDL-C concentration (r = 0.19, P = 0.023). In addition, in the control group, hs-CRP correlated positively with waist-to-hip-ratio (r = 0.21, P = 0.008).
Correlations between hs-CRP concentration and selected variables in each group.

*Spearman’s correlation coefficient. P < 0.05 was considered to represent statistical significance.
BMI: body mass index; SBP: systolic blood pressure; DBP: diastolic blood pressure; TC: total cholesterol; TG: triglycerides; HDL: high-density lipoprotein-cholesterol; LDL-C: low-density lipoprotein-cholesterol; Apo A: apolipoprotein A; Apo B: apolipoprotein B.
Table 4 shows the prevalences of cardiometabolic defects, classified according to hs-CRP category, in the full sample. Low cardiovascular risk was the most common category (44%), followed by intermediate risk (37%), and high cardiovascular risk (19%). There were significantly higher prevalences of obesity (83.9%), high waist circumference (85.7%), high blood pressure (30.4%), hypercholesterolemia (21.4%), hypertriglyceridemia (35.7%), and Apo B concentration in the highest tertile (39.3%) in the high cardiovascular risk group than in the low-risk group.
Prevalences of cardiometabolic abnormalities for each cardiovascular risk group in the full sample.

P-values were calculated using the chi-square test. P < 0.05 was considered to represent statistical significance.
hs-CRP concentrations of <9.52, 9.52 to 28.57, and >28.57 nmol/L were accepted as indicating low, moderate, and high risks of cardiovascular disease, respectively.
LDL-C: low-density lipoprotein-cholesterol; HDL-C: high-density lipoprotein-cholesterol; Apo A: apolipoprotein A; Apo B: apolipoprotein B.
This analysis was also performed separately in the obese and control groups, but significant differences was only identified in the obese group, because hypertriglyceridemia was more prevalent in the intermediate cardiovascular risk group than in the low-risk group (15.2% vs. 2.1%, respectively; P = 0.007).
The relationships between cardiometabolic defects and hs-CRP concentration in the moderate and high cardiovascular risk groups are shown in Table 5. In the full sample, there were strong associations of hs-CRP ≥28.57 nmol/L with obesity (OR = 13.9, 95% confidence interval [CI] = 6.1–32.09, P < 0.001), high waist circumference (OR = 8.0, 95% CI = 3.49–18.39, P < 0.001), hypertriglyceridemia (OR = 4.0, 95% CI = 1.82–8.97, P < 0.001), high blood pressure (OR = 3.4, 95% CI = 1.47–7.86, P = 0.004), hypercholesterolemia (OR = 2.8, 95% CI = 1.15–6.98, P = 0.023), and ApoB in the highest tertile (OR = 2.4, 95% CI = 1.01–5.99, P = 0.045). In the control group alone, only hs-CRP 9.52 to 28.57 nmol/L was significantly associated with hypertriglyceridemia (OR = 9.8, 95% CI = 1.82–53.21, P = 0.008), and in the obese group there were no significant associations.
Association of clinical and laboratory findings with cardiovascular risk.

Associations were analyzed using logistic regression and were adjusted for age and sex. P < 0.05 was considered to represent statistical significance.
hs-CRP concentrations of 9.52 to 28.57 and >28.57 nmol/L were accepted as indicating moderate and high risks of cardiovascular disease, respectively.
HDL-C: high-density lipoprotein-cholesterol; LDL-C: low-density lipoprotein-cholesterol; Apo A: apolipoprotein A; Apo B: apolipoprotein B; CI: confidence interval; OR: odds ratio.
Discussion
The main finding of the present study was that obesity, dyslipidemia, and high blood pressure are strongly associated with high hs-CRP concentrations in young adults from southern Mexico. In particular, in those with obesity, the serum hs-CRP correlated with body composition measurements (BMI, body fat percentage, and waist circumference) and serum LDL-C concentration; whereas only one of these parameters showed a significant correlation in the control group.
Similarly, in a previous study of premenopausal women, positive correlations were identified between hs-CRP and BMI, waist circumference, body fat, and visceral fat; 14 and in a study of postmenopausal women, between hs-CRP and BMI, waist circumference, and serum TG. 15 Furthermore, indices of adiposity in children have been shown to be positively related to hs-CRP.16,17
The results of several previous studies have suggested that obesity represents a low-grade inflammatory state, as indicated by a high serum hs-CRP concentration. 18 Adipose tissue has an endocrine function, secreting numerous adipokines with a wide variety of effects. These include cytokines, such as tumor necrosis factor alpha (TNF-α), interleukin-1 (IL-1), and interleukin-6 (IL-6), which induce the synthesis of acute phase proteins, such as CRP, in the liver. 19 This may be one mechanism by which obesity confers greater cardiovascular risk at all stages of life.
In the present study, the metabolic defects that were identified in the young adults with high cardiovascular risk, identified using the measurement of hs-CRP concentration, were obesity, high waist circumference, high blood pressure, hypercholesterolemia, hypertriglyceridemia, and Apo B in the highest tertile. These results are consistent with those that were reported in a study of young adults from Jamaica, in which individuals with hs-CRP >28.57 nmol/L had high prevalences of obesity, high waist circumference, hypertriglyceridemia, and low serum HDL-C concentration. 20 Taken together, these results suggest that subclinical inflammation may be associated with obesity, high blood pressure, and abnormal lipid metabolism.
In the present study, we also identified strong associations of obesity, high waist circumference, hypertriglyceridemia, high blood pressure, hypercholesterolemia, and Apo B in the highest tertile with high cardiovascular risk in young adults. Similar associations have been reported in a number of different populations. In the National Health and Nutrition Examination Survey (NHANES) 2009–10, metabolic syndrome was found to be associated with high hs-CRP, and in addition, the larger the number of metabolic abnormalities that were present, the higher was the risk of an individual having a high hs-CRP concentration. 21 Furthermore, in a study of retired individuals in the US, obesity was found to be associated with a higher risk of having an hs-CRP >28.57 nmol/L. 22 In a study conducted in Iran, it was shown that the fasting glucose, TC, LDL-C, and TG concentrations of the participants were associated with both CVD risk and an hs-CRP concentration >28.57 nmol/L. 23 Finally, in the Framingham Offspring Study, a significant relationship was identified between components of the metabolic syndrome or insulin resistance and high hs-CRP. 24
The low-grade systemic inflammation that is a feature of metabolic syndrome can be explained by the production of proinflammatory cytokines, such as TNF-α and IL-6, by adipose tissue, which inhibit insulin signaling and increase the hepatic synthesis of CRP.25,26 In addition, IL-6 inhibits lipoprotein lipase, which increases the serum TG concentration. 26 Moreover, insulin resistance may lead to greater hepatic CRP production because the insulin-induced inhibition of acute-phase protein expression is inhibited. 27 Thus, a vicious circle can be created that promotes inflammation and insulin resistance, which is the principal underlying pathophysiological defect in metabolic syndrome. This systemic inflammation may be useful for the identification of young adults who are at high risk for the development of CVD.
High-fat diet-induced obesity is associated with systemic inflammation. The mechanism involves the binding of toll-like receptor (TLR4) by saturated fatty acids, which triggers the activation of inflammatory signaling pathways. In addition, some dietary factors can reduce the concentrations of proinflammatory molecules in young people, thereby preventing the development of insulin resistance, type 2 diabetes, and CVD. 28 Therefore, future studies should evaluate the efficacy of nutritional interventions aimed at ameliorating inflammation in obese individuals, using CRP to monitor the effects.
The limitations of the present study include the small sample size, which reduces its statistical power, the use of a single hs-CRP measurement, and its cross-sectional design.
Conclusion
We have identified strong associations between cardiometabolic parameters and high cardiovascular risk, indicated by high serum hs-CRP concentration, in young adults from southern Mexico.