
Abstract
Arterial hypertension is one of the major causes of cardiovascular morbidity and mortality worldwide. Effective and sustained reduction in blood pressure is essential to reduce individual cardiovascular risk. In daily clinical practice, single-pill fixed-dose combinations of different drug classes are important therapeutic resources that could improve both treatment adherence and cardiovascular risk management by targeting distinct pathophysiological mechanisms. The aim of this practical narrative review is to help physicians choosing the right single-pill fixed-dose combination for the right patient in the daily clinical practice, based on the individual clinical phenotype and cardiovascular risk profile.
Keywords
Introduction
Hypertension is one of the most relevant modifiable risk factors in the genesis and progression of micro- and macrovascular damage and their sequelae, including coronary heart disease (CHD), heart failure (HF), ischemic and hemorrhagic stroke, chronic kidney disease (CKD) and peripheral arterial disease (PAD).1–4 Hypertension is often coupled with other cardiovascular (CV) comorbidities, such as dyslipidemia, which contributes to atherosclerosis in hypertensives. 5 After nonpharmacologic interventions as first therapeutic approach, antihypertensive and lipid-lowering drugs are usually needed to obtain the appropriate therapeutic targets, especially in patients at higher CV risk. Unfortunately, recommended therapeutic targets are sometimes difficult to achieve, especially in high-risk patients, in the setting of real-world practice.6–8 Low adherence to prescribed therapy in chronic conditions, such as hypertension and dyslipidemia, was found to cause worsening of prognosis and mortality and may frequently be related to complex drug regimens with multiple pills given at multiple times.9,10 The availability of pills with fixed-dose combinations (FDC) of antihypertensive drugs and lipid-lowering drugs is useful to remind physicians of the need to identify and manage multiple CV risk factors, improve treatment adherence, and achieve therapeutic targets.11–14
Nevertheless, a one-size-fits-all FDC strategy cannot work well in the era of precision medicine. The aim of the following practical review is to help physicians choosing the right single-pill FDC, or the right combination of two FDC pills, for the right patient in the daily clinical practice, based on the individual clinical phenotype and CV risk, to improve both treatment effectiveness and adherence, leading to a better control of major risk factors with consequent reduction of CV morbidity and mortality. Hypertension guidelines suggest preferred treatments for hypertensive patients with specific ‘profiles’ like, for example, ‘uncomplicated hypertension’ or ‘hypertension and associated established conditions’. In this focused clinical review, we chose to generally define those hypertensive patients’ ‘phenotypes’, according to their peculiar features, that are the most commonly encountered in the daily clinical practice, in which FDC play a key role to improve both treatment adherence and effectiveness.
Rationale for single-pill FDC use in hypertension management and their current availability
According to the 2018 European Society of Cardiology/European Society of Hypertension (ESC/ESH) Guidelines for the management of arterial hypertension, the best strategy to reach blood pressure (BP) target and to reduce CV risk is starting the treatment with an association of two different drugs, preferably in a single-pill FDC, in most patients. 15 The rationale for the use of combinations of different drug classes lies in the greater effectiveness, because of targeting distinct pathophysiological mechanisms, an adequate 24-h coverage, and a greater adherence to long-term drug therapy. Moreover, correct combinations provide a better safety and tolerability profile.16,17 The single-pill FDC most commonly used and currently available for hypertension treatment and control are made up of two (or more) of these five major drug classes: angiotensin II type 1 receptor antagonists (ARB), angiotensin-converting-enzyme inhibitors (ACEi), thiazide (TD) and thiazide-like diuretics (TLD), calcium channel blockers (CCB), beta-blockers (BB), in various combinations (Table 1). Each component is also available at various doses, so physicians can choose the best treatment strategy for each patient phenotype. Besides the several two-drug FDC of antihypertensive drugs, there are also ‘triple combo’ available for prescription to date, such as the combination of perindopril/indapamide/amlodipine and olmesartan/amlodipine/hydrochlorothiazide (HCT). Furthermore, FDC of ARB/statin, CCB/statin, or the ‘triple combo’ of atorvastatin/perindopril/amlodipine are also available for the management of both hypertension and dyslipidemia (Table 1).
Currently available single-pill FDC for the management of hypertension and for the management of combined hypertension and dyslipidemia.

ACEi, angiotensin-converting-enzyme inhibitor; ARB, angiotensin II type 1 receptor antagonist; BB, beta-blocker; CCB, calcium channel blocker; FDC, fixed-dose combination; MRA, mineralocorticoid receptors antagonist; TD, thiazide diuretic; TLD, thiazide-like diuretic.
The choice of the best antihypertensive therapeutic strategy should take into account global CV risk profile, primary or secondary prevention setting, comorbidities, and treatment adherence of each patient. In any case, this choice must rely on evidence-based medicine and randomized controlled trials (RCT) that tested the efficacy, safety, and tolerability of the several available FDC.
How to choose the single-pill FDC according to BP levels and treatment targets
High-normal BP and grade 1 hypertension with low cardiovascular risk
This phenotype is commonly underdiagnosed and undertreated. Lifestyle changes are the first and sometimes only initial approach to be taken in both patients with high-normal BP and patients with grade 1 hypertension and low CV risk. Lifestyle changes allow to reduce the risk of progressing to established or higher degree hypertension and may further reduce the CV risk of these subjects. Salt restriction to < 5 g per day, moderation of alcohol consumption, high consumption of vegetables and fruits, weight reduction or ideal body weight, regular physical activity, and smoking cessation are the well-known key points for a correct lifestyle. 15 Given the context of low CV risk in this population, several position papers suggest the opportunity to take into account also antihypertensive supplements or nutraceuticals that are likely able to help in BP lowering without significant side effects, in addition to lifestyle advice.18,19 Among many nutraceuticals, most with unproven or unlikely benefits, bioactive substances enriched with nitrates, sources of nitric oxide (i.e. red beets) exert proven vasodilator effects and decrease BP levels.19,20 When lifestyle changes and supplements or nutraceuticals are not enough, both the guidelines for CV prevention 21 and for BP management 22 indicate the possibility to use antihypertensive drugs in patients with grade 1 hypertension, even if at low CV risk, and even in high-normal BP individuals when CV risk is high. Usually, monotherapy with an ARB or an ACEi is enough to reduce BP to optimal levels (at least below 130/80 mmHg).
Hypertension in patients uncontrolled by monotherapy
The 2018 ESC/ESH Guidelines for the management of arterial hypertension suggest an initial monotherapy only in subjects with grade 1 hypertension and low CV risk, or in very old, frail patients. 15 When BP target is not achieved by monotherapy, the best choice is using different drugs to target multiple mechanisms, such as inhibition of the renin-angiotensin-system (RAS), vasodilatation, and diuresis. The use of a single-pill FDC could lead to a better 24-h BP control and improve treatment adherence at the same time, based on very large and solid evidence. 15 Combination therapy of two drugs has greater efficacy than monotherapy, even at doubled dose. 17 Moreover, low-dose combination therapies are associated with fewer adverse events than the higher doses of single agents that would be required to achieve the same level of BP control. 23 The first choice of single-pill FDC is based on the combination of ACEi or ARB with a CCB or a diuretic, 22 therefore four possible different FDC pills. The multicenter, prospective, randomized controlled Anglo-Scandinavian Cardiac Outcomes Trial-Blood Pressure Lowering Arm (ASCOT-BPLA) trial 24 enrolled 19,257 hypertensive patients aged 40–79 years with at least three other CV risk factors. The amlodipine ± perindopril regimen was found to prevent more major CV events and mortality than the BB ± TD combination, with a better metabolic safety profile: stroke −23%, acute coronary event −13%, renal failure −15%, CV-caused mortality −24%, and developing diabetes −30%. The single-pill FDC perindopril/amlodipine (ACEi and CCB) has shown efficacy in reducing BP, target organ damage, and CV risk in patients with hypertension.25–28 In the PEARL ABPM study, 262 patients were evaluated with ambulatory BP monitoring (ABPM), showing that the FDC perindopril/amlodipine led to an effective, safe, and sustained 24-h BP control in patients with hypertension uncontrolled by ACEi or CCB alone or a free combination of them. 26
Other single-pill FDC are ARB/CCB or ARB/TD. Clinical studies on the use of single-pill FDC of telmisartan/amlodipine and telmisartan/HCT found that these therapies provided significant BP reduction, BP goal rates, and response rates in patients at all stages of hypertension, compared with the respective monotherapies. Moreover, in patients with mild-to-moderate hypertension, the telmisartan/amlodipine combination provided superior 24-h BP-lowering efficacy compared with either treatment administered as monotherapy. Similarly, the telmisartan/HCT FDC treatment provided superior 24-h BP-lowering efficacy, especially in the last 6 h, compared with other RAS inhibitor–based single-pill FDC, such as losartan/HCT. 29 With its long half-life characteristics, once-a-day olmesartan/amlodipine FDC is very powerful in BP reduction consistent across the 24-h dosing interval, ensuring good coverage of the nighttime, the one most associated with organ damage.30,31 In the Combination of Olmesartan Medoxomil and Amlodipine Besylate in Controlling High Blood Pressure (COACH) trial, the reduction in BP (−30.1 mmHg in office systolic BP with the maximum dosage) was achievable already in the first 2 weeks of therapy with olmesartan/amlodipine FDC. 32 Both the FDC of olmesartan/amlodipine and perindopril/amlodipine have been shown to maintain their similar effectiveness in lowering BP even after 48 hours from last administration. 33 The FDC valsartan/amlodipine compared with nifedipine GITS in patients with hypertension inadequately controlled by monotherapy was also found to be more efficacious and better tolerated. 34 Moreover, the availability of FDC with valsartan/TD and valsartan/CCB allows the administration of the first FDC in the morning and of the second FDC in the evening, with valsartan given twice daily, to obtain an adequate 24-h coverage. 15
Hypertension in patients uncontrolled by two-drug regimens
Three antihypertensive drugs, better if combined in a single-pill FDC, are often needed to reach the desired BP target. 15 The three-drug single-pill FDC of perindopril/indapamide/amlodipine is one of the first ‘triple therapy’ available in several countries and contains the direct vasodilator amlodipine, indapamide that increases natriuresis, while the consequent RAS stimulation is efficaciously counteracted by the ACEi perindopril. 35 In the PIANIST (Perindopril-Indapamide plus AmlodipiNe in high rISk hyperTensive) trial, the efficacy of perindopril/indapamide plus amlodipine was evaluated. This trial included 4731 patients at high or very high CV risk, and uncontrolled hypertension. BP targets were reached by 72.0% of patients treated with triple therapy and by 81% and 91% of patients previously treated with an ACEi/HCT or an ARB/HCT combination, respectively. 35 Confirming these data, the PAINT (Perindopril-Amlodipine plus Indapamide combination for controlled hypertension Non-intervention Trial) study found that perindopril/amlodipine plus indapamide led to an adequate 24-h BP control in patients who did not reach target with two antihypertensive drugs. 36 This 4-month, open-label, observational, prospective, multicenter study included 6088 patients with hypertension uncontrolled by previous monotherapy or dual therapy, including RAS inhibitor/amlodipine or RAS inhibitor/HCT, and free triple therapy associations (28%, 37%, and 36% of the patients enrolled, respectively). A 24-h ABPM was performed in a subgroup of 62 patients, finding a significant reduction of 24-h BP, both systolic blood pressure (SBP) (from 138.7 ± 12.5 to 125.5 ± 12.8 mmHg) and diastolic blood pressure (DBP) (from 77.5 ± 11.4 to 70.4 ± 8.7 mmHg). 36
Another three-drug single-pill FDC available in several countries is olmesartan/amlodipine/HCT. A 12-week, randomized, double-blind, parallel-group trial (TRINITY) conducted in 2492 patients with BP ⩾ 140/100 or ⩾ 160/90 mmHg found that the proportion of patients reaching BP target at study end was significantly higher with this triple combination (69.9%) compared with dual therapies (52.9% for olmesartan/amlodipine, 53.4% for olmesartan/HCT, and 41.1% for amlodipine/HCT), with a significantly greater reduction in sitting BP. 37
In a recent paper on 520 hypertensive patients, which compared ACEi-based triple therapy versus ARB-based triple therapy, we found an apparently better 24-h, daytime and nighttime BP control in the first group of patients, but it was linked to the lower number of antihypertensive pills taken. In fact, the only single-pill triple therapy FDC available in our country (Italy) is an ACEi-based one. These data confirm the important role played by FDC of two or more drugs in improving adherence, by reducing the number of pills needed. 38
Combination therapy also offers advantages concerning the possible side effects of antihypertensive drugs. Malleolar edema is the most common side effect reported during the chronic treatment with CCB, 39 while hypokalemia can be induced by diuretics. 15 The use of therapeutic combinations of ACEi (or ARB) and CCB and/or diuretic reduces the risk of these undesirable side effects, thanks to counterbalancing effect elicited by RAS inhibition and the possibility of using lower dosages of each drug. 15
Although much more limited combinations are available (Table 1), the addition of mineralocorticoid receptors antagonist (MRA)/potassium-sparing diuretics, alpha-blockers, or BB are possible further therapeutic options in patients with hypertension resistant to triple combination therapy 15 or in patients with specific indications for these drugs. A salt-retaining state, most likely due to inappropriate aldosterone secretion, is often present in some of these patients, especially if obese with elevated intake of sodium, and MRA may therefore offer some advantage over other antihypertensive drug classes. 40
How to choose the single-pill FDC according to comorbidities
Hypertension in patients with dyslipidemia
Dyslipidemia and low-density lipoprotein cholesterol (LDL-C) levels are too often neglected in hypertensives, especially in patients at higher CV risk. 3 On one side, autosomal-dominant hypercholesterolemia (known as familial hypercholesterolemia) is the most severe and most common monogenic hypercholesterolemia with an estimated incidence of one case every 250–300 births. 41 These patients are often diagnosed only after a first CV event. 42 This condition implies to reach a target of LDL-C below 70 or 55 mg/dl, according to the 2019 European Society of Cardiology/European Atherosclerosis Society (ESC/EAS) Guidelines for the management of dyslipidemia, infrequently achievable with a single-drug therapy. 43 Earlier detection and greater use of combination therapies are required to reduce the CV risk of these patients. 44 On the other side, more commonly, patients have cholesterol levels within the ‘normal range’, but they may still be dyslipidemic ‘de facto’, having too high LDL-C levels according to their individual CV risk.3,45 Adding statins to the antihypertensive therapies has great benefits according to several clinical studies that justify their use in hypertensive subjects with moderate-to-high CV risk.15,45 Indeed, BP reduction alone cannot optimally manage the CV risk in hypertensive patients with moderate or high risk of atherosclerotic cardiovascular disease (CVD). These patients benefit from statins besides antihypertensive therapy: this association further reduces the risk of myocardial infarction and stroke, even in case of well-controlled BP.15,46,47 The single-pill FDC atorvastatin/perindopril/amlodipine is indicated for treatment of essential hypertension and/or coronary artery disease, in association with primary hypercholesterolemia or mixed hyperlipidemia, as substitutive therapy in adult patients not adequately controlled with atorvastatin, perindopril, and amlodipine given separately at the same dose. The Anglo-Scandinavian Cardiac Outcomes Trial (ASCOT) was an independent, investigator-initiated, randomized, multicentric trial designed to compare two antihypertensive therapeutic strategies for the prevention of CHD events in more than 18,000 hypertensive patients with no history of CHD. In the ASCOT-Lipid Lowering Arm (LLA), 10,305 of the 19,342 patients randomized to one of the two antihypertensive regimens (atenolol ± bendroflumethiazide and amlodipine ± perindopril) were further randomized to receive atorvastatin 10 mg/day or placebo. 46 The trial showed how in hypertensive patients, mostly at moderate CV risk, lipid-lowering treatment with atorvastatin 10 mg, combined with anti-hypertensive therapy based on amlodipine ± perindopril, resulted in a significant (36%) reduction in fatal CHD and nonfatal myocardial infarction compared with placebo. 46 The positive effects of this therapeutic approach are also maintained in the long term, as demonstrated by ASCOT-Legacy trial, related to mortality outcomes after 16 years follow-up of the participants recruited in the UK (n = 8580) from the original ASCOT trial. 48 In addition, patients in LLA group treated with atorvastatin in ASCOT trial experienced a significant reduction in CV mortality compared with the placebo group [hazard ratio (HR) = 0.85, 95% confidence interval (CI) = 0.72–0.99]. 48 The single-pill FDC atorvastatin/perindopril/amlodipine was the first available ‘triple’ therapy to reduce both BP and cholesterol levels as well as total CV risk.
A single-pill FDC with rosuvastatin and amlodipine was also recently available. According to a multicenter, randomized, double-blind, parallel-group phase III clinical trial, combination treatment with rosuvastatin 20 mg + amlodipine 10 mg effectively reduced both BP and LDL-C levels while maintaining safety. 49
Many hypertensive patients, despite receiving high-intensity statin, do not reach an adequate LDL-C target and require treatment with combinations of lipid-lowering drugs. 3 Single-pill FDC usually combine two drugs with complementary mechanisms of action providing enhanced efficacy. Treatment options include FDC of a statin plus ezetimibe. Statins act by inhibiting 3-hydroxy-3-methylglutaryl coenzyme A (HMG-CoA) reductase thus reducing cholesterol synthesis in all tissues and increasing the availability of the LDL-C receptor, whereas ezetimibe inhibits the intestinal absorption of cholesterol. These FDC are safe and more effective than increasing the dosage of the single statin in patients with hypercholesterolemia or dyslipidemia with or without diabetes and with or without CVD.50–53 Patients taking a statin/ezetimibe FDC could have a greater chance of being highly adherent to treatment than those taking a free combination of these two drugs. 54 The aggressive lipid lowering using this drug combination was associated with a greater coronary plaque regression in patients who underwent percutaneous coronary intervention (PCI) and lower risk of myocardial infarction and ischemic stroke in high CV risk patients with no evidence of harm caused by adding ezetimibe to the statin or further LDL-C reduction, in terms of serum transaminases and creatine kinase elevation, muscle-related adverse events, or cancer.55–57
In the next future, FDC with bempedoic acid, which acts by reducing cholesterol synthesis in the liver but not in the muscles, and ezetimibe, or indeed a triple combination (bempedoic acid, ezetimibe, and statin), will also enhance therapeutic choices.58,59 Therefore, patients affected by both hypertension and dyslipidemia may also benefit from two different single-pill FDC, one for BP control and one for a more potent cholesterol reduction, with the opportunity to tailor the therapy.
Hypertension in patients with overweight/obesity
Overweight/obese phenotype is likely the most common in daily clinical practice. It is estimated that about 75% of essential hypertensives have an overweight/obese phenotype. Adiposity is one of the main factors contributing to the BP increase in essential hypertension, through multiple pathophysiological mechanisms.4,31,60–62 Weight loss is recommended in hypertensive overweight/obese patients to control metabolic risk factors, nevertheless a weight stabilization could be a reasonable goal for most of them. 15 This phenotype tends to salt and water retention, because of enhanced RAS activity and reduced levels of natriuretic peptides. 61 Moreover, a sustained sympathetic overdrive is also present. 63 The consequent BP increase has the functional role to increase sodium filtration to avoid edema accordingly to the well-established pressure/natriuresis relationship. 61 Therefore, diuretic therapy is usually needed to reach an adequate 24-h BP control in these patients. However, diuretic therapy could also facilitate hypokalemia, if RAS is not simultaneously antagonized, especially because these patients usually have also a very high salt intake 64 (even up to an average of 12 g/day in obese hypertensives) and more sodium reaches the distal tubule and is reabsorbed in exchange with potassium and hydrogen. Therefore, hypertension control rate among overweight/obese subjects is often suboptimal, because of these specific pathophysiologic mechanisms and comorbidities. In a context of a concomitant metabolic syndrome, TD and BB have shown to increase insulin resistance, while ACEi/ARB may increase insulin sensitivity. 65
In the observational study FORSAGE, 66 a post hoc analysis was performed to evaluate whether it was useful to switch from previous antihypertensive therapy to the single-pill FDC perindopril/indapamide (10/2.5 mg), in relation to body mass index (BMI) at baseline. The BP target was achieved in all BMI groups, even included overweight/obese patients. Perindopril/indapamide FDC, given the mechanisms of action, is particularly suitable for overweight/obese hypertensive patients, as also confirmed in the recent post hoc analysis of pooled raw data from four large observational studies (FORTISSIMO, FORSAGE, ACES, PICASSO) with a −30 mmHg (systolic BP) in obese patients or patients with metabolic syndrome at 3 months. 67
Single-pill FDC of ARB and TD could be another therapeutic option. For example, large multicenter studies demonstrated the efficacy and tolerability of FDC irbesartan/HCT, available at several dosages (150/12.5 mg, 300/12.5 mg, and 300/25 mg). Patients with moderate or severe hypertension receiving FDC irbesartan/HCT as initial therapy obtained more rapid BP reductions compared with irbesartan monotherapy and enabled a greater proportion of patients with severe hypertension to achieve their BP target. 68 It is noteworthy that the association of ACEi or ARB with lower doses of HCT (i.e. 12.5 mg) could not reach the adequate 24-h BP control, particularly if administered once daily, because of HCT short half-life.69,70 This inefficacy of the 12.5 mg HCT dose is particularly emphasized in the obese patient with high sodium intake coupled with reduced renal function.
Nighttime hypertension and nondipper pattern are highly prevalent in overweight/obese hypertensive patients, as well as in older patients and in patients with diabetes mellitus, resulting in greater target organ damage.31,71 In this context, RAS inhibitors, CCB, and diuretics were found to be superior to BB and alpha-blockers for restoring normal dipping pattern. 72 The triple FDC of perindopril/indapamide/amlodipine taken in the morning showed a drop in nighttime BP values, also without any other evening administration of antihypertensive drugs, 73 highlighting the long half-life and the sustained antihypertensive effect over 24 hours of these drugs. Therefore, longer half-life drugs are preferable in this population. FDC containing a RAS inhibitor and a CCB can be given advantageously in the evening, whereas FDC containing a RAS inhibitor and a long half-life TLD could be given in the morning. Attention should be paid to the possible accentuation of nocturia, which is highly prevalent in patients with nighttime hypertension (typically found in overweight/obese patients with obstructive sleep apnoea), following the administration of CCB, especially if in monotherapy in the evening and not counteracted by an appropriate RAS inhibition. 74
Hypertension in patients with type 2 diabetes mellitus
This patient phenotype, commonly seen in clinical practice, shares many aspects with the obese patient, but when T2DM is diagnosed after years/decades of altered glucose metabolism (prediabetes), patients are usually already at high or very high CV risk. Diabetes through the years leads to a sharp amplification of BP-related micro- and macrovascular damage, promoting the progression of hypertension-mediated organ damage (HMOD), which is at the base of the increased risk of developing major CV events. 15 Polypharmacy is a frequent problem in T2DM patients having hypertension, dyslipidemia, and often other comorbidities. The use of FDC is essential for this patient phenotype to both improve treatment adherence and achieve the multiple therapeutic targets needed. In these patients, it is recommended to start the treatment with a combination of an ACEi or an ARB and a CCB or a TD/TLD. 15 Using an ACEi or an ARB has also the aim of protecting kidneys and renal function. 75 Therefore, preventive therapy (often as secondary prevention in T2DM) needs to reach a BP target even below 130/80 mmHg in patients younger than 65 years old. In patients older than 65 years old, BP target could be within the range of 130 to 139 mmHg, even though recent evidence indicate that lower BP levels could be more beneficial even in fit older patients.22,76 According to ADVANCE (Action in Diabetes and Vascular disease: PreterAx and DiamicroN MR Controlled Evaluation) trial, adding a diuretic to an ACEi (perindopril/indapamide in this case) could be taken into account to obtain a consistent BP reduction. 77 In this trial, the arm of the study evaluating BP reduction with perindopril plus indapamide showed also a reduction in major CV events and mortality, regardless baseline BP levels. 77 In ADVANCE-ON trial, 78 8494 patients were included for a median of 5.9 years (BP-lowering comparison) or 5.4 years (glucose-control comparison). The patients randomized to antihypertensive therapy with the association perindopril/indapamide had shown a significant reduction in the risk of death from any cause and of death from CV causes, a reduction by 9% that had been observed also at the end of the post-trial follow-up. 78 On the contrary, no differences were observed according to the intensive glucose control. 78 This study, as well as others, highlighted the key role of BP reduction in T2DM patients over a tight glucose control. A subanalysis of another real-life, open-label, observational trial (PICASSO trial) was carried out in a subgroup of 2762 uncontrolled hypertensive patients affected by T2DM or prediabetes to evaluate the efficacy of FDC perindopril 10 mg/indapamide 2.5 mg. 79 After 3 months of treatment, the T2DM cohort showed a significant reduction in office BP (−27.0 ± 14.8/−12.7 ± 9.8 mmHg) and the BP control was reached in 61% of patients. Decreases in systolic and diastolic BP were statistically significant regardless of hypertension grade at baseline. 79 These data confirmed that FDC with ACEi/TLD could be regularly taken into account in the treatment of hypertensive patients affected by T2DM uncontrolled by another antihypertensive therapy. On the other side, FDC without a diuretic work well only in overweight/obese T2DM patients who maintain a low-sodium diet, otherwise the combination with a TD or TLD is the most recommended. If necessary, triple FDC (perindopril/amlodipine/indapamide) has also been shown to be effective with a protective metabolic profile in long-term studies. 80
Data on T2DM patients are also present regarding FDC with ARB. A population-based, retrospective cohort study examined a group of 54,186 patients with T2DM aged 66 years and older who started treatment with candesartan, irbesartan, losartan, telmisartan, or valsartan, to evaluate which ARB was associated with a lower risk of hospital admission for acute myocardial infarction, stroke, or HF. Investigators found a lower risk of hospital admission in patients taking telmisartan (adjusted HR = 0.85, 95% CI = 0.74–0.97) or valsartan (adjusted HR = 0.86, 95% CI = 0.77–0.95). 81 Irbesartan and losartan were found to exert renoprotective activities in T2DM patients with concomitant CKD, therefore FDC of these two ARBs should be preferred in these patients. In two large studies (Irbesartan in Type 2 Diabetes with Microalbuminuria 2 – IRMA 2 and Irbesartan Diabetic Nephropathy Trial – IDNT), irbesartan exerted a renoprotective effect in hypertensive patients with T2DM at both early and later stages of diabetic nephropathy.82,83 The renoprotective effect was at least partly independent of the BP-lowering effect. The efficacy and tolerability analysis results of the Reduction of Endpoints in Non Insulin Dependent Diabetes Mellitus with the Angiotensin II Antagonist Losartan (RENAAL) study strongly support the use of losartan as part of the standard of care in patients with T2DM and nephropathy to reduce the risk of progression to end-stage renal disease (ESRD). 84
Hypertension in patients with ischemic heart disease
Heart disease is a common sequela in hypertensive patients. Older hypertensive patients, especially with T2DM and CKD, very often suffer from ischemic heart disease and HF with or without atrial fibrillation. 85 The development of left ventricular hypertrophy, as detected by cardiac ultrasonography, is the most common sign of HMOD. 86 The 2018 ESC/ESH Guidelines for the management of arterial hypertension included three simplified algorithms for the treatment of hypertension in patients with coronary artery disease, HF, and atrial fibrillation. 15 BB have proven to be particularly useful in hypertension treatment of patients with specific heart conditions, including symptomatic angina, heart rate disturbances, post-myocardial infarction, and HF with reduced ejection fraction (HFrEF). 15 The addition of perindopril to BB therapy was effective in CV protection in hypertensive patients with stable coronary artery disease in a subanalysis of the EUropean trial on Reduction Of cardiac events with Perindopril in stable coronary Artery disease (EUROPA), 87 in which it determined a reduction of combined primary endpoint of CV death, fatal and nonfatal acute myocardial infarction (−28%). The positive outcome in this trial was mainly due to the larger BP reduction (over 4 mmHg) of the treatment arm compared with the placebo arm. 87 In the Prospective Urban Rural Epidemiology (PURE) study, less than 50% of patients with CVD worldwide (and less than 10% of patients in low-income countries) received the three or more drugs needed in secondary prevention. 88 According to the Fixed-Dose Combination Drug for Secondary Cardiovascular Prevention (FOCUS) study, the use of a polypill strategy may improve adherence for secondary prevention following an acute myocardial infarction. 89 The therapeutic regimen should include lipid-lowering drugs (statin alone or combined with ezetimibe), antihypertensive drugs (usually two or more), and an antiplatelet (low-dose aspirin). 90 In this context, the recently published TIPS3 trial 91 using a polypill with 40 mg of simvastatin, 100 mg of atenolol, 25 mg of HCT, 10 mg of ramipril, and 75 mg of aspirin in a large intermediate-risk population in primary prevention, led to a 31% reduction of major CV events during a mean follow-up of 4.6 years. These findings, as well as those in several other previous studies, are heralding the incoming of many polypills in the near future, being useful in both primary and secondary prevention. A novel FDC capsule containing rosuvastatin (5-10-20 mg) and 100 mg of acetyl salicylic acid may have a key role in secondary prevention together with single-pill FDC to lower BP when needed. 92
Hypertension in patients with previous stroke and/or cognitive impairment
Hypertensive patients with previous stroke, regardless by the subtype (lacunar ischemic stroke, thromboembolic stroke, atherothrombotic stroke, or hemorrhagic stroke), are at high risk of further cerebral and noncerebral CV events and death. Stroke is likely the most preventable CV event thanks to an intensive BP lowering. 93 Previous RCT suggest that BB are less effective in stroke prevention than other classes of antihypertensive agents. Inversely, CCB were found to be superior to other drugs for the prevention of stroke.94,95 In the PROGRESS Trial, perindopril, with the addition of indapamide, if necessary, led to a reduction from 26% to 49% in the risk of recurrent stroke in patients with a history of cerebrovascular events. 96 Therefore, FDC based on CCB or TLD and a RAS inhibitor, such as ACEi, should be preferred, together with FDC of lipid-lowering drugs, such as statin/ezetimibe, according to the very high CV risk of these patients. Furthermore, the use of a polypill containing also aspirin would be desirable after an ischemic cerebral event. 90
Another cerebral condition related to high BP is cognitive impairment, especially vascular dementia, 97 a common condition in older patients. Although previous studies have often shown inconsistent results, CCB and ARB likely had larger benefits than other antihypertensive drug classes on prevention of cognitive decline in meta-analysis of RCT and prospective cohort studies.98–100
Hypertension in patients with CKD
Hypertension with renal damage is a very common patient phenotype, especially among older patients and those with T2DM, in whom CKD is highly prevalent. Achieving BP control in CKD may be difficult and a combination of antihypertensive drugs is usually required, together with careful lifestyle modification (i.e. sodium restriction). A well-known marker of microvascular damage is albuminuria that is also a marker of accelerated renal damage. ACEi or ARB are more effective in reducing albuminuria than other antihypertensive agents and are indicated in hypertensive patients in the presence of microalbuminuria or overt proteinuria, 15 as also emphasized by the recent KDIGO (Kidney Disease Improving Global Outcomes) guidelines. 101 The combination of a RAS blocker with a CCB or a diuretic is recommended as first-line therapy and FDC of two (or three) drugs are helpful in improving adherence.15,102 An adequate BP control is essential to slow down the progression of CKD and lower mortality, and RAS blockers in patients with advanced nephropathy and proteinuria showed additional protection from progression of renal damage.103,104 The use of ACEi or ARB in CKD is very often accompanied by an initial increase of creatinine levels, as a result of a reduction in glomerular filtration rate. This is expected because of the reduction of systemic BP as well as reduction in the vasoconstriction of efferent arterioles with consequent fall in glomerular filtration pressure. 75 Nevertheless, RAS inhibitors are the best chance to protect residual nephrons and they just show the residual renal function at normal pressure without hyperfiltration in the residual glomeruli. 105 An elevated intake of sodium not corrected by lifestyle changes, as often happens, requires diuretic therapy to eliminate the excess of sodium/volume overload and TLD (indapamide and chlorthalidone) are preferred even when glomerular filtration rate is around 30 ml/min, whereas loop diuretics (torasemide better than furosemide, thanks to its longer half-life) are required for even lower glomerular filtration rates.106–108
How to choose the single-pill FDC according to age
Hypertension in older adults
Nearly 80% of older adults suffer from arterial hypertension. In particular, isolated systolic hypertension (systolic BP ⩾ 140 mmHg and diastolic BP < 90 mmHg) is found in more than 80% of patients aged 80 years and older, linked to the loss of the elastic fibers in large arteries and diffuse arteriosclerosis with increase in collagen in the media and adventitia resulting in increased arterial stiffness.109,110 Physical performance, comorbidities, frailty, and psycho-social factors should be also evaluated before choosing the best therapeutic strategy for older patients. 111 Nevertheless, age per se should not represent an obstacle to hypertension treatment. Diuretics, especially the TLD indapamide, ACEi, ARB, and CCB, have all shown benefit on CVD outcomes in older patients. Unless clinically indicated by comorbidities, BB should not be used as first-line medications in hypertensive patients in general and particularly in older patients, because they may worsen CVD outcomes in those aged 60 years and older. This may be related to the slowing of heart rate and the facilitation of augmentation of central aortic BP, as shown in the Conduit Artery Function Evaluation (CAFE) study, a substudy of the ASCOT. 112 Moreover, the use of alpha-blockers should be avoided due to the increased risk of falls, especially if an orthostatic hypotension has not been properly evaluated by a complete physical examination, unless they are strictly needed for other pathologies, such as dysuria associated with prostate hypertrophy. 113 In older patients, when nonpharmacologic lifestyle interventions fail, some specific monotherapy can be appropriate and successful. The Hypertension in the Very Elderly Trail (HYVET) used indapamide (in a controlled-release formulation of 1.5 mg) in patients aged 80 years and older, even in monotherapy, finding positive results in reducing both BP and CV outcomes, especially HF and stroke. 114 In most older patients, whenever an FDC is administered, it is recommended to start with lower doses. 15 Evidence from RCTs found that antihypertensive therapy reduces significantly both CV morbidity and mortality from all causes even in older patients. In the Systolic Blood Pressure Intervention Trial (SPRINT), intensive treatment (unattended SBP target of less than 120 mmHg) led to significantly reduced risks of death from CV causes and death from any cause in older patients. 76 Moreover, risks and benefits of BP lowering did not appear to be modified by pulse pressure, a BP parameter that increases with age being a marker of increased arterial stiffness.110,115 In the more recent STEP trial (Strategy of Blood Pressure Intervention in the Elderly Hypertensive Patients), lower incidence of CV events was found in older hypertensive patients reaching a more intensive BP control, confirming the data of SPRINT. 116 In the latter, a slightly higher incidence of hypotension was found in the intensive treatment group. 76 In the STEP trial, SBP target was of 110 to less than 130 mmHg in the intensive treatment group versus 130 to less than 150 mmHg in the standard treatment group. 116 The mean number of medications needed to reach these targets was 1.9 in the intensive treatment group and 1.5 in the standard treatment group. Hypotension occurred more frequently in the intensive treatment group than in the standard treatment group, but the incidence of dizziness, syncope, fracture, and the results for renal outcomes did not differ significantly between the two groups. Anyway, during the median follow-up period of 3.34 years, the incidence of stroke, acute coronary syndrome, acute HF, coronary revascularization, atrial fibrillation, or death from CV causes was significantly lower in the intensive treatment group than in the standard treatment group. 116 The Anglo Scandinavian Cardiac Outcomes Trial BP lowering arm (ASCOT-BPLA) showed significant overall mortality benefit in subjects aged 60 years and older, when a combination of CCB and ACEi was given.24,117 According to a randomized, open-label, blinded-endpoint study of morbidity and mortality (Combination of OLMesartan and a CCB or a diuretic in Japanese elderly hypertensive patients – COLM study), olmesartan combined with a CCB (amlodipine or azelnidipine), even though not as FDC, was the therapeutic strategy linked with lower incidence of all adverse events and discontinuation of treatment, compared with olmesartan plus a diuretic in high-risk older hypertensive patients. 118 On the other hand, a diuretic is usually needed when reduced glomerular filtration rate is present, especially below 45 ml/min. TLDs, such as indapamide and chlortalidone, should be preferred over HCT, because they maintain efficacy even below 30 ml/min of estimated glomerular filtration rate, when usually low doses of a loop diuretic, adequately dosed to cover 24 h, may be needed. 106 Many older hypertensive and dyslipidemic patients, especially those affected by T2DM, may have chronic microvascular brain damage responsible for severe consequences such as mild cognitive impairment that can progress to dementia, beyond the macroscopic clinical cerebrovascular events, such as ischemic stroke. In cerebrovascular prevention, BP lowering is essential (BP target < 130/80 mmHg regardless of age). According to the 2018 ESC/ESH Guidelines for the management of arterial hypertension, FDC of an ACEi or ARB and a CCB or a TLD should be the first choice. 15 On the other hand, in the presence of vascular dementia and parkinsonism, a special attention should be given to coexistent dysautonomia, often characterized by orthostatic hypotension, found during daytime activities, and supine hypertension, found during nighttime rest. 119 Orthostatic hypotension can be worsened by dopamine-based therapies, often administered for parkinsonism, and in the postprandial state, while nighttime hypertension requires appropriate treatment, usually with shorter-acting drugs that adequately control nighttime hypertension without worsening daytime standing hypotension. 120 In this scenario, FDC have no role and therapy must be carefully personalized.
Regarding isolated systolic hypertension, in the SPRINT subanalysis on patient aged ⩾75 years, the combination of two or more antihypertensive drugs was taken by the majority of the study population. This treatment regimen in the intensive arm was found to reduce both fatal and nonfatal major CV events and death from any cause, without a significant increased risk of injurious falls. 76 CCB or TLD in association with a RAS inhibitor have demonstrated an important reduction of BP values and CV morbidity also in hypertensive patients with isolated systolic hypertension.114,121–124
Hypertension in younger adults
In Western Europe, the prevalence of hypertension is 15% in men aged 18–39 and 30% in men aged 40–59 and approximately 5% and 30%, respectively, in women of the same age groups. 125 All young individuals with grade 2 or more severe hypertension should receive lifestyle advice and drug treatment, as well as young adults with grade 1 hypertension considered to be at high risk (i.e. presence of HMOD, overt CVD, T2DM, CKD, and those with high overall CV risk, although CV risk may often be underestimated in younger adults in short-term projections, such as those at 10 years). 15 In younger adults with uncomplicated grade 1 hypertension, there is an absence of specific RCTs demonstrating the benefit of antihypertensive treatment. The use of antihypertensive drugs can be considered safe and so are considered FDC in this population.15,126 In addition to the ‘classic’ systolic–diastolic high BP, hypertension in younger adults could be isolated systolic or isolated diastolic. Isolated grade 1 systolic hypertension, typical of smokers, is often associated with a normal central aortic pressure and the benefits of drug treatment in addition to lifestyle changes are still not clearly proven.15,127 In the absence of clinical evidence, if a drug therapy is needed, perhaps in a context of increased central aortic pressure/increased aortic pulse wave velocity, preferred drug choices are ACEi, ARB, CCB, diuretic, or their combinations, according to the characteristics of the patients. 128 On the other hand, isolated diastolic hypertension in young adults is likely associated with increased risk of composite CV events, CV mortality, hemorrhagic stroke. 129 In this scenario, in the absence of specific RCTs on BP lowering, no specific pharmaceutical classes are recommended, although a CCB or combinations including a CCB could be suggested, given their vasodilating activities.128,130
Conclusion
The available single-pill FDC according to patient phenotype are summarized in Figure 1. Choosing the right antihypertensive therapy according to the patient phenotype and to the individual CV risk leads to a better control of hypertension and larger reduction of total CV risk and improves treatment adherence, thus lessening the burden of CV morbidity and mortality. A practical approach includes the appropriate use of single-pill FDC according to the patient characteristics (Figure 2). When BP control alone is unable to adequately reduce the CV risk, patients can benefit from adding a lipid-lowering therapy on top of the antihypertensive therapy, especially using a single-pill FDC containing both antihypertensive and lipid-lowering drugs.

The available single-pill FDC according to patient phenotype.
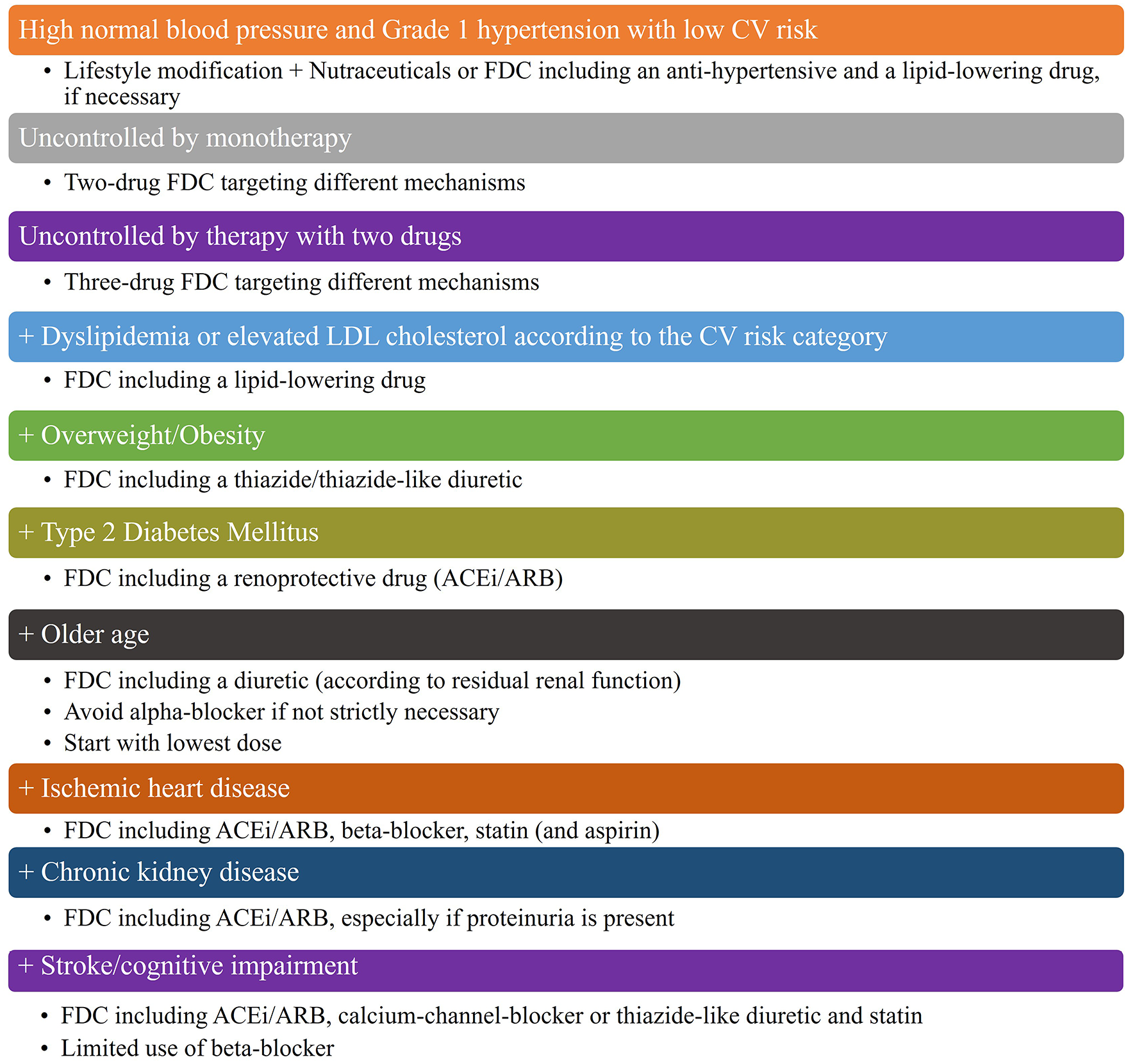
Simplified approach to hypertension (and dyslipidemia) treatment using single-pill FDC, according to patient phenotype.
Footnotes
Acknowledgements
None.
Ethics approval and consent to participate
Not applicable.
Consent for publication
All authors have read and approved the submission and publication of the manuscript.
Author contributions
Availability of data and materials
The authors confirm that the data supporting the findings of this study are available within the article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article. The open access fee for this article was funded by Servier, Italy.
Conflict of interest statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.