
Abstract
Background and aims:
Lung cancer patients suffer from deterioration in their physical and psychological function, which exerts a negative influence on their quality of life (QOL). Telemedicine has been proven to be an effective intervention for patients with several chronic diseases. The aim of this systematic review and meta-analysis was to investigate the efficacy of telemedicine in improving QOL in lung cancer patients.
Methods:
PubMed, Cochrane Library, EMBASE, Web of Science and Scopus databases were searched for randomized controlled trials that investigated the effectiveness of telemedicine in lung cancer patients. Review Manager 5.3 and Stata 15.1 were used to perform data analysis.
Results:
Our meta-analysis included eight clinical trials with a total of 635 lung cancer patients. The results showed that the telemedicine group had significantly higher QOL than the usual care group [standard mean difference (SMD) 0.96, 95% confidence interval (CI) 0.29–1.63, I2 = 91%]. In addition, the telemedicine group had lower anxiety (SMD −0.44, 95% CI −0.66 to −0.23, I2 = 3%) and depression scores (SMD −0.48, 95% CI −0.91 to −0.05, I2 = 66%) than the usual care group. However, no significant differences were found in fatigue and pain outcomes between the two groups.
Conclusion:
Telemedicine may be an effective method of improving QOL in lung cancer patients and the further development and use of telemedicine care is recommended.
Introduction
Lung cancer is one of the most common types of cancers and the leading cause of death from malignancy. At least 2.09 million people were newly diagnosed with lung cancer and the number of cancer-related deaths had reached up to 1.76 million in 2018 worldwide.1,2 The characteristics of tumour cells and certain cancer-related treatments are such that patients with lung cancer endure a high burden of symptoms such as fatigue and anxiety.3,4 As a result, preserving the quality of life (QOL) of patients as they decline has become an urgent concern.5–7
Telemedicine was defined by the World Health Organization (WHO) in 1997 as the delivery of health care services by information and communication technologies (ICTs) at a distance. 8 Recommended as a type of safe, cost-effective and time-saving intervention, it has emerged in the last two decades as a non-invasive surveillance and follow-up method for patients discharged from hospital.9,10 ICTs such as websites, telephone and telemedicine systems have been established to detect and manage patients’ physical and psychological changes in a timely manner, improve communication between health care providers and patients or their families and allow patients to effectively self-manage.11,12 In addition, the value of telemedicine in chronic disease management has been confirmed in meta-analyses examining its use in conditions such as heart failure, chronic obstructive pulmonary disease and asthma.13–15 Telemedicine has been proven to have played an important role in dermatology during the 2019 novel coronavirus disease (COVID-19) pandemic. 16
Few reviews have explored the effectiveness of telehealth in the management of malignant tumours, especially in improving QOL. In the past few years, several clinical trials have been conducted to examine the effectiveness of telemedicine in increasing the QOL of lung cancer patients, and mobile applications have even been developed to monitor their disease status.17–21 On the one hand, patients diagnosed with lung cancer demand an effective intervention to enable them to manage problems under their own initiative on a long-term basis in the follow-up period after initial treatment. On the other hand, interaction between health care providers and lung cancer patients has been a target for improving patients’ QOL. 22 Telemedicine is acknowledged as a promising method for improving QOL by virtue of its unique advantages, and the results of several clinical trials have provided strong evidence for this view.23,24 However, due to high heterogeneity among these studies, the exact effect of telemedicine on the QOL of patients with lung cancer remains unknown. Thus, we conducted this meta-analysis to examine the superiority of telemedicine in lung cancer patients.
Methods
Search strategy
Two investigators (LP and ZL) independently searched for articles in the databases PubMed, Cochrane library, EMBASE, Web of Science and Scopus. Medical Subject Headings (MeSH) and free search terms were both used in the literature search. The search terms included telemedicine, telemonitor, e-health, telehealth, telecommunication, telemanagement, telecare, telephone monitoring, telepathology, remote and short message service, mobile health, telerehabilitation, lung neoplasm, lung neoplasms, lung carcinoma, lung cancer and lung tumour. The search strategy used for PubMed was as follows: (telemedicine OR telemonitor OR e-health OR telehealth OR telecommunication OR telemanagement OR telecare OR telephone monitoring OR telepathology OR remote and short message service OR mobile health OR telerehabilitation) AND (lung neoplasm OR lung neoplasms OR lung carcinoma OR lung cancer OR lung tumour). The final search date was 14 February 2020. In addition, we manually searched the references of the screened articles for further high-quality studies.
Study selection
Two investigators (LP and HL) independently skimmed the identified abstracts and selected articles to fully review. The same two investigators independently undertook full text review (including intensively reading appropriate articles after skimming the references of screened articles). A senior investigator (CC) adjudicated when eligibility could not be agreed.
Inclusion criteria were as follows: (1) patients diagnosed with lung cancer; (2) telemedicine intervention, defined as “the use of telecommunication systems to deliver health care at a distance”; (3) usual care referred to the usual oncology care; (4) reported outcomes including at least one of the following: QOL, anxiety, depression, fatigue or pain; (5) experimental studies, including randomized controlled trials (RCTs) and quasi-RCTs.
The following were excluded: (1) letters or reviews; (2) laboratory studies, case reports or animal experimental studies; (3) studies not published in English language; (4) studies with an absence of key information such as sample size.
Data extraction and outcome definitions
Two investigators (LP and HL) independently extracted data and any disagreements were discussed with the third investigator (ZL) or subsequently resolved via consensus. Extracted data included first author, publication year and country, number of participants and their characteristics (age, sex and disease status), interventions (technology, intervention providers), follow-up time and outcomes. If the necessary data could not be found in the published paper, investigators obtained them by emailing the original authors.
QOL was set as our primary outcome, with anxiety, depression score, fatigue and pain as secondary outcomes.
Risk of bias assessment
Two investigators (LP and HL) independently undertook a risk of bias assessment and any doubts were resolved by the third investigator (ZL).
We evaluated risk of bias of trials according to the Cochrane handbook of systematic reviews of interventions (http://handbook.cochrane.org). In addition, we applied the revised Jadad’s scale to assess the quality of each study.
Statistical analysis
Review Manager 5.3 (Cochrane) and Stata 15.1 were used for statistical analysis. For continuous variables such as QOL, we calculated standardized mean difference (SMD) with 95% confidence interval (CI). For discrete variables, we calculated odds ratio with 95% CI. Heterogeneity was evaluated using the Cochrane Q-statistic and I2 statistic. If the I2 statistic was above 50% and the Cochrane Q-statistic had a p value ⩽ 0.1, a random-effects model was used. However, if no considerable heterogeneity among studies was apparent, a fixed-effect model would be used. Subgroup analysis was conducted to explore high heterogeneity and pre-defined stratification including the follow-up time, type of QOL scale and technologies used. Funnel plots and Egger test were used to assess potential publication bias.
Results
Search process, study characteristics and quality assessment
Based on the search criteria, we found 1742 articles. Of these, 1353 articles remained after removing duplications. We selected 73 of the articles for full consideration after reading the title and abstract. In addition, we manually searched two studies for intensive reading after skimming the references lists of the 73 articles. Finally, eight studies with a total of 635 patients were enrolled to our meta-analysis, all of which were experimental studies (six RCTs and two quasi-RCTs) published between 2014 and 2019.23–30 The process of selecting the included studies is presented in Figure 1.

Flow diagram of the selection of the included studies.
Table 1 shows the basic characteristics of the enrolled articles and the essential information of the participants. The studies were conducted in United States,23,26,27 China,28,30 United Kingdom, 29 France 24 and Turkey. 25 Six23,25–27,29,30 of them had adopted a telephone-based intervention while the remaining studies were Web-based. Follow-up duration ranged from 3 weeks to 8 months. Scales to measure QOL included the WHO-QOL score and the Functional Living Index − Cancer, among others. Revised Jadad’s scale scores of the included studies are also presented in Table 1, and indicate that the studies were of high quality except for two. Figures 2 and 3 demonstrate the methodological quality of the included studies. In the domain of incomplete outcome data and selective reporting, all the included studies were judged as having low risk of bias. However, two studies (quasi-RCTs)23,25 failed to meet the criteria of random sequence generation and allocation concealment. Whether blinding was carried out was unclear in most of the studies.
Characteristics of the included studies and participants.
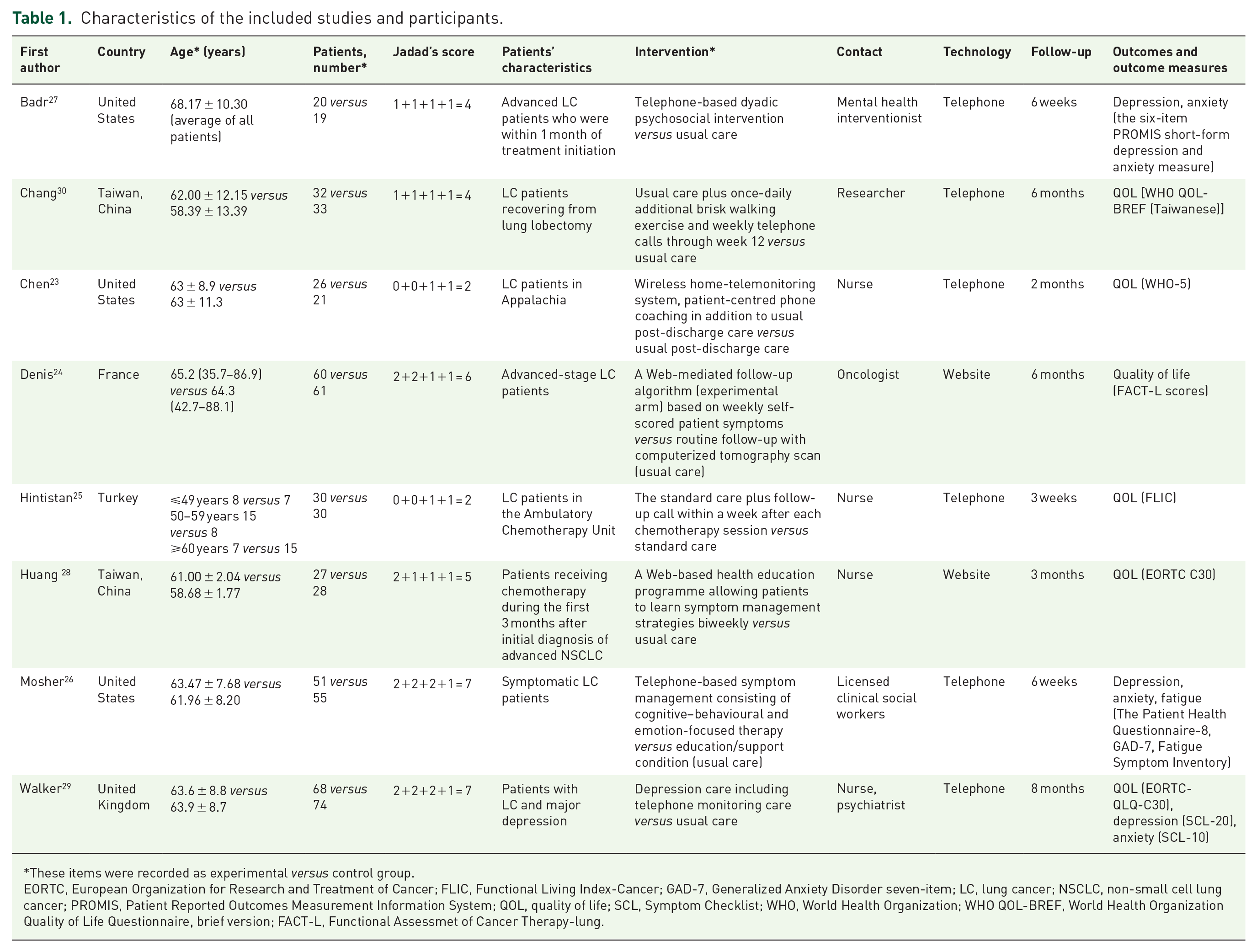
These items were recorded as experimental versus control group.
EORTC, European Organization for Research and Treatment of Cancer; FLIC, Functional Living Index-Cancer; GAD-7, Generalized Anxiety Disorder seven-item; LC, lung cancer; NSCLC, non-small cell lung cancer; PROMIS, Patient Reported Outcomes Measurement Information System; QOL, quality of life; SCL, Symptom Checklist; WHO, World Health Organization; WHO QOL-BREF, World Health Organization Quality of Life Questionnaire, brief version; FACT-L, Functional Assessmet of Cancer Therapy-lung.

Risk of bias graph.

Risk of bias summary.
Quality of life
To compare telemedicine with usual care in the improvement of QOL, we enrolled data from six of the studies23–25,28–30 with a total of 490 patients. The results demonstrated that the telemedicine group reported a significantly higher QOL than the usual care group (SMD 0.96, 95% CI 0.29–1.63). Heterogeneity testing showed that I2 = 91%, indicating high heterogeneity (Figure 4). To address high heterogeneity, we conducted a subgroup analysis grouped by follow-up time (>3 months or not), type of scale (WHO-QOL or not) and type of technology (telephone-based or Web-based).
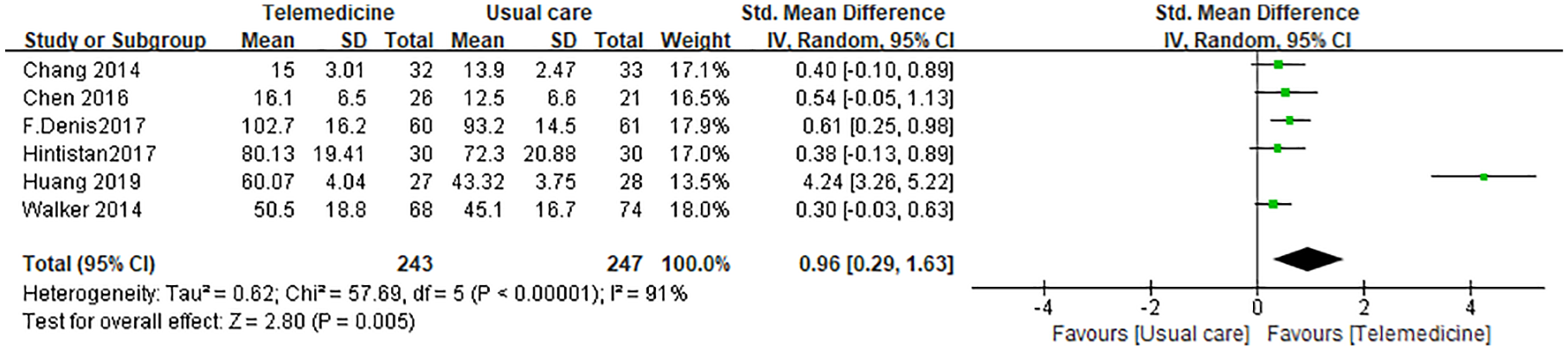
Analysis comparing telemedicine versus usual care for quality of life in lung cancer patients.
The subgroup analysis for follow-up time showed that the telemedicine group had significantly higher QOL than the usual care group for long-term follow-up (SMD 0.43, 95% CI 0.21–0.65, I2 = 0%), whereas no significant difference was observed in short-term follow-up (SMD 1.67, 95%CI −0.23 to 3.57, I2 = 96%; Figure 5).

Subgroup analysis of quality of life comparing telemedicine with usual care grouped by follow-up time.
In the subgroup analysis for type of scale, the telemedicine group had significantly higher QOL than the usual care group both in the WHO-QOL group (SMD 0.46, 95% CI 0.08–0.83, I2 = 0%) and the other types of QOL scale subgroup (SMD 1.26, 95% CI 0.25–2.28, I2 = 95%; Figure 6).

Subgroup analysis of quality of life comparing telemedicine with usual care grouped by type of scale.
In the subgroup analysis stratified by type of technology, the telemedicine group had significantly higher QOL than the usual care group for telephone-based intervention (SMD 0.37, 95% CI 0.15–0.60, I2 = 0%). However, differences between the Web-based and usual care groups were not significant (SMD 2.40, 95%CI −1.15 to 5.95, I2 = 98%; Figure 7).

Subgroup analysis of quality of life comparing telemedicine with usual care grouped by type of technology.
The funnel plot shown in Figure 8 indicates potential publication bias. However, no significant potential publication bias was found using the Egger test (p = 0.072). This inconsistency may be due to the small number of enrolled studies.
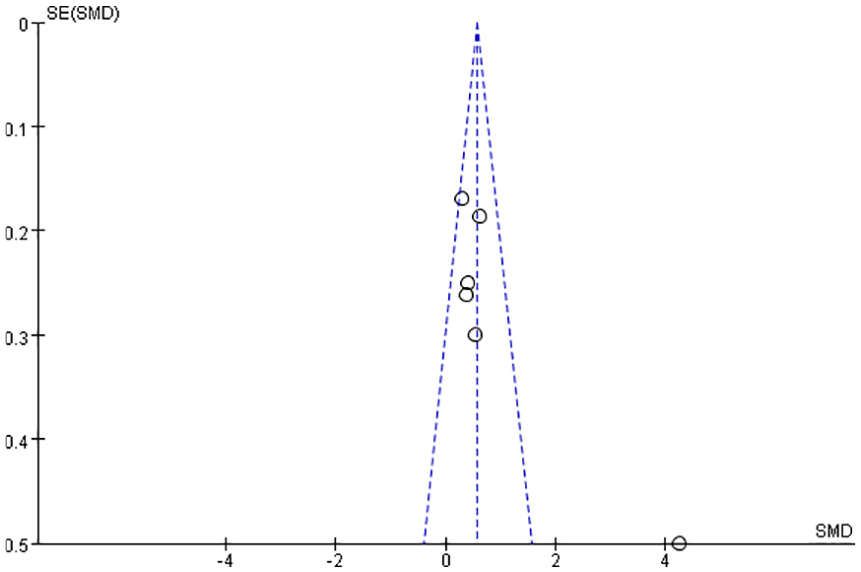
Funnel plot showing publication bias.
Anxiety
To investigate the efficacy of telemedicine in alleviating anxiety compared with usual care, we included four articles25–27,29 with 347 patients. Anxiety scores in the telemedicine group were lower than in the usual care group (SMD −0.44, 95% CI −0.66 to −0.23). Heterogeneity testing showed that I2 = 3%, indicating low heterogeneity (Figure 9).

Analysis comparing telemedicine with usual care for managing anxiety in lung cancer patients.
Depression
Our study enrolled three studies26,27,29 with a total of 287 patients to examine the superiority of telemedicine in easing depression in lung cancer patients. As shown in Figure 9, depression scores were lower in the telemedicine group than in the usual care group (SMD −0.48, 95% CI −0.91 to −0.05). Heterogeneity testing showed that I2 = 66%, indicating high heterogeneity (Figure 10).

Analysis comparing telemedicine with usual care for managing depression in lung cancer patients.
Fatigue
To comparing telemedicine and usual care in relieving fatigue in lung cancer patients, we enrolled three studies25,26,29 with a total of 308 patients. The results indicated no significant difference between telemedicine and usual care group in fatigue (SMD −0.27, 95% CI −0.85 to 0.30). Heterogeneity testing showed that I2 = 83%, indicating high heterogeneity (Figure 11).

Analysis comparing telemedicine with usual care for managing fatigue in lung cancer patients.
Pain
To examine whether telemedicine could alleviate pain in lung cancer patients compared with usual care, we included three studies25,26,29 with a total of 308 patients. These two groups did not have significantly different pain outcomes (SMD −0.18, 95% CI −0.57 to 0.21). Heterogeneity testing showed that I2 = 64%, indicating high heterogeneity (Figure 12).

Analysis comparing telemedicine with usual care for managing pain in lung cancer patients.
Discussion
With the further development of cancer treatment, clinic staff are increasingly focused on not only patients’ lifespan but also their QOL. It is acknowledged that patients with lung cancer experience a greater symptom burden than patients with any other type of cancer.4,7 Previous studies have reported that lung cancer patients have severe symptoms, including anxiety, depression, pain and fatigue.3,7 Moreover, these symptoms have been confirmed to exert a negative influence on their QOL. 31 Several studies have investigated the excellent capability of non-invasive intervention to improve their QOL and alleviate their psychological burden.32–34 A meta-analysis conducted by Chen et al. 35 demonstrated that telehealth care had advantages over usual care in improving QOL in breast cancer patients, proving the positive effects of e-health technologies in the management of malignancy.
Our study explored the effectiveness of telemedicine on the management of patients with lung cancer. We showed that a telemedicine group had a significantly better QOL than a usual care group. Subgroup analysis stratified by type of technology indicated that QOL in the telemedicine group was significantly better than that of the usual care group when telephone-based intervention was used. Moreover, the telemedicine group had a significantly better QOL than the usual care group during long-term follow-up. The telemedicine group also had lower anxiety and depression scores than the usual care group.
One reason for these results about QOL is the unique superiority of telemedicine in overcoming the obstacle of distance between patients and clinic staff. Follow-up time was also subjected to subgroup analysis, with the results suggesting that telemedicine might be more effective than usual care in the long-term management of patients. This implies that the advantages of telehealth intervention over usual care need a relatively long time to be observed. Compared with website-based technology, lung cancer patients were more likely to benefit from telephone-based interventions. As the lung cancer patient population is mostly elderly, the assumption is that they may be more familiar with telephone technology than with the internet.
Lung cancer patients who undergo surgery spend a lot of time recovering from trauma and with deteriorated pulmonary function. 36 Patients unfit for surgery may experience considerable discomfort and distress during chemotherapy or radiotherapy.37,38 Instant and ongoing feedback from their physicians about their suffering may provide them with significant comfort and support. Consequently, e-health web systems and applications have been devised to ensure that clinic staff and patients can contact each other conveniently, potentially contributing to improving patients’ QOL.18,19 Nevertheless, one RCT has reported that symptom telemonitoring combined with active feedback from patients was not superior to the relatively passive method of symptom telemonitoring only in maintaining the well-being of lung cancer patients. 39 This suggests further investigation and more research are necessary.
In terms of symptom burden, anxiety and depression scales scores were lower in the telemedicine group than those in the usual care group. However, there were no significant differences in fatigue and pain outcomes between the two groups. Khue et al. 40 has demonstrated that depression and anxiety pose risks to the QOL of lung cancer patients, which is consistent with our findings. However, a telehealth-based pulmonary rehabilitation intervention for advanced lung cancer patients was reported to be capable of alleviating fatigue, depression and anxiety, which was not completely concordant with our results. 20 In addition, an enrolled study conducted by Hintistan et al. 25 did not report the scales used for the assessment of pain and other symptoms.
The use of telemedicine to improve the QOL of lung cancer patients is relatively new and the publication year of all our enrolled studies was 2014 or later. Chang et al. 30 conducted an RCT in 2014 on an early postoperative walking exercise programme in which the intervention was incorporated with a weekly telephone call. Since this, a number of telehealth systems designed to maintain QOL in lung cancer patients have emerged with technologies not limited to telephone but also including websites. Therefore, more high-quality RCTs are encouraged to explore the promising value of telemedicine in the maintenance of QOL in patients with lung cancer.
Our study had some limitations. First, the number of enrolled articles and participants was small, with recent clinical studies still underway. However, this study was, to our knowledge, the first meta-analysis to investigate the efficacy of telehealth care in lung cancer patients. Second, two of the enrolled studies were quasi-RCTs that did not implement random sequence generation, impairing the quality of this meta-analysis. Moreover, interventions in the telemedicine group were not limited to only telephone or internet, but also incorporated other types of non-invasive interventions, such as exercise programmes and depression care. Finally, the form of interventions varied considerably among studies in terms of follow-up time, technology medium and the intervention providers with whom patients were in contact, leading to the high heterogeneity of the enrolled studies.
Conclusion
Overall, telemedicine has an advantage in improving the QOL and psychological outcomes (including reported anxiety and depression) in patients with lung cancer. Telemedicine may be an effective intervention in managing the well-being of lung cancer patients. We suggest that more resources are put into the development of telehealth care and more high-quality RCTs are conducted to explore the value of telemedicine in the management of lung cancer patients.
Footnotes
Acknowledgements
We acknowledge all the contributed authors. We also acknowledge Dr Fabrice Denis and Dr Yea-Jyh Chen for their kindness to provide the necessary data in their studies.
Author contributions
QZ, CC designed the study. LP designed the search strategy. LP and ZL performed the search. LP and HL performed the abstract screening, full text screening, data extraction, and risk of bias assessment. ZL, SL, ZL helped in the revision process. All the authors drafted and revised the manuscript.
Availability of data and materials
The datasets used in this study are available from the corresponding author upon request. All data generated or analysed in this study are included in the published articles or obtained from the authors who published the enrolled articles.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Consent for publication
All the contributed authors have agreed to the publication of this manuscript.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.