
Abstract
The internet and digital technology have become an important resource for patients with cancer. Mobile health strategies permit patients and clinicians to interact via different tools to enrich the supplements to routine hospital visits or out-patient attendance. In this work, we have reviewed different mobile health platforms to support lung cancer patients in different areas: pre-surgery; post-surgery and on systemic treatment. We have also reviewed different digital tools used by long-term lung cancer survivors as well as the impact of these tools on the quality of life, and we tried to analyse according to literature the potential efficiency of these platforms in health system administration.
Introduction
Lung cancer (LC) is one of the most prevalent cancers worldwide and has significant mortality rates. 1
Tobacco is the main cause of LC; however, the diagnosis of LC among non-smoking patients is not unusual and is associated with different driver mutations, such as EGFR mutations, translocations in ALK and ROS1, as well as other molecular findings. LC patients suffer from various symptoms, including cough, dyspnoea, pain, fatigue and nausea, as well as emotional disease and social concerns, all of which require health support in many occasions. 2 Advanced LC treatment is based on a systemic therapy consisting of a drug combination (platinum-based chemotherapy and immunotherapy (IT)), IT in monotherapy, or targeted drugs in those patients who carry any targeted molecular alteration (EGFR, ALK, ROS1, etc.). These treatments are associated with a moderate level of toxicity, especially in fragile and highly symptomatic patients. 3
Therefore, having stricter control of their clinical situations as well as other parameters that are closely related to quality of life (QoL) and cancer outcome (diet, physical activity, sleep, emotional status, medication adherence, social and family support, etc.) could improve patients’ outcomes.
The internet and digital technology have become an important resource for patients and professionals within the oncology community in recent years. The World Health Organization (WHO) defines telemedicine as the delivery of healthcare services, at a distance, via information and communication technologies. 4
Telemedicine strategies permit patients and clinicians to adopt new interactive tools that supplement routine hospital visits or out-patient attendance, involving several challenges in the setting of LC treatment and surveillance. 5
Self-management could be defined as ‘the individual’s ability to manage the symptoms, treatment, physical and psychosocial consequences guided by specific professionals’ recommendations targeted to modify lifestyle or complementary treatments’. To this aim, self-management interventions supported by telehealth platforms can help patients and their caregivers manage their symptoms. 6
In the COVID era, telemedicine in cancer settings experienced a considerable development. Fragile patients, like LC patients with the highest mortality rate among cancer patients infected with SARS-Cov2, were encouraged to avoid hospital visits. 7
In this review, we aim to examine the evidence of several telemedicine tools in LC patients in different settings: advanced disease, resected patients, long-term survivors, and so on. We will try to analyse the strategy’s impact on LC patients’ outcomes, mainly in their QoL and prognosis.
Telemedicine for cancer care
Telemedicine includes multiple modalities and devices like electronic health (e-Health) and mobile health (m-Health), computers, tablets, wearables, websites, and so on. 8
The WHO has defined telemedicine as a remote healthcare service by professionals in the field, using information and communication technologies to exchange data that can be used for diagnosing, treating and preventing disease and injuries.
Telehealth studies are heterogeneous. There are various platforms and systems of monitoring, as well as variables that include diverse aims and target populations. The integration of these m-Health systems in hospital electronic reports is one of the most interesting challenges to implement in routine practice.
Notably, the costs of attending cancer patients are increasing every year: patients live longer, have more expensive treatments, are treated with more than one treatment line, and so on. With the healthcare system’s saturation, telemedicine is an interesting strategy to optimise efficiency in professionals’ integral attendance. Medical economic studies are needed to guide the authorities’ decision. Investment in telemedicine strategies could be cost-effective and could optimise medical attendance. Recently, many Applications for remote follow-up have been developed, but there is limited data showing their cost-effectiveness. Still, a few studies have shown that the usage of telehealth cuts cost and could potentially end the threat of an unaffordable healthcare system.9,10
Recent technological innovations and internet access allow communication between different devices as they can exchange data between each other. The internet of things (IoT) is a new concept that enables users to connect various sensors and smart devices in order to gather information from the environment in real time. The main objective of technology is to expand internet benefits with remote control capability, data sharing, continuous communication and so on. 11
The health of many people worldwide could improve with the right access to hospitals and health monitoring. Thanks to the latest advances in technology, patients can be monitored remotely, thereby reducing physical hospital Appointments. 12
In countries where access to healthcare is limited, telemedicine can help circumvent this problem, particularly in vulnerable groups. It can help in an era of increased needs and limited resources. The interest in telemedicine has grown worldwide in the last few decades owing to the fact there are many advantages. Probably the most known characteristic of telemedicine is that it can overcome geographic distance, allowing people to receive medical care even if they live in rural areas.13,14
Cancer follow-up is usually settled in international clinical guidelines. However, there is heterogeneity among different specialists, health facilities and countries. In addition, in the private sphere, insurance companies can sometimes limit surveillance exams for financial reasons. Telemedicine could help oncologists by enabling a remote, non-invasive and more personalised monitoring of the patient which could improve the detection of recurrence, progression or supportive care needs.
The unsustainability of healthcare systems, together with increasing demand for self-management tools, triggers the growth of m-Health technologies. The thriving m-Health technology enhances the patient’s empowerment, helps support clinical decision-making and strengthens the process of data generation by collecting data from different sources and linking together stakeholders in the healthcare sector. By giving the professionals more information and useful resources, they can arrive at more well-founded diagnoses/decisions.15,16
Telemedicine is a wide concept used to describe different strategies to Apply telecommunication technology to medicine, where mobile Apps and IoT are several examples. Having explained the importance of telemedicine, IoT and the inclusion of technology in daily life, it is worth presenting some real examples of how this has been Applied to medicine in the last few years. So many Applications or devices have been developed in the LC setting. Some of them can help patients in different aspects, but only the few that focus on monitoring and/or management of LC patients will be mentioned in this review.
m-Health Applications used in patients with LC
As we previously mentioned, physical and psychological symptoms are common in LC patients. The lack of control over their symptoms is a factor leading to poor adherence, impaired well-being and health-related QoL, and an increase of health service use and mortality. Late reporting of symptoms, owing to uncertainty of the severity and difficulty of establishing contact with health professionals, delays and hinders the correct assessment of symptoms in different scenarios in common clinical practice. 17
In this section, we will describe different scenarios that involve experience m-Health systems. Table 1 lists all the studies analysed in this work, focused on patients with LC and in which m-Health platforms are used. On the other hand, Figure 1 shows the main functionalities and characteristics of digital health tools Applied in LC.
An exhaustive collection of all studies in different LC scenarios using several Apps.
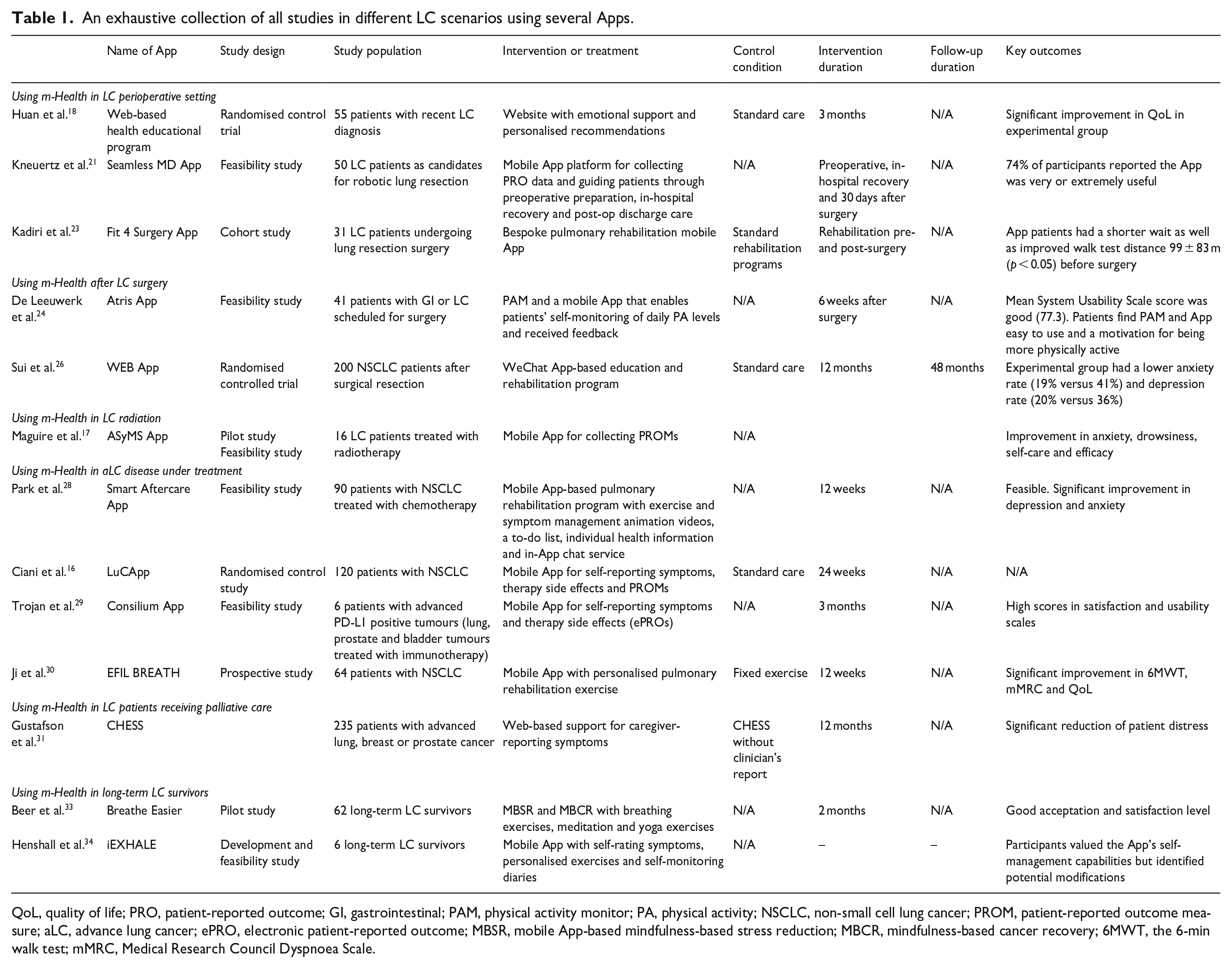
QoL, quality of life; PRO, patient-reported outcome; GI, gastrointestinal; PAM, physical activity monitor; PA, physical activity; NSCLC, non-small cell lung cancer; PROM, patient-reported outcome measure; aLC, advance lung cancer; ePRO, electronic patient-reported outcome; MBSR, mobile App-based mindfulness-based stress reduction; MBCR, mindfulness-based cancer recovery; 6MWT, the 6-min walk test; mMRC, Medical Research Council Dyspnoea Scale.
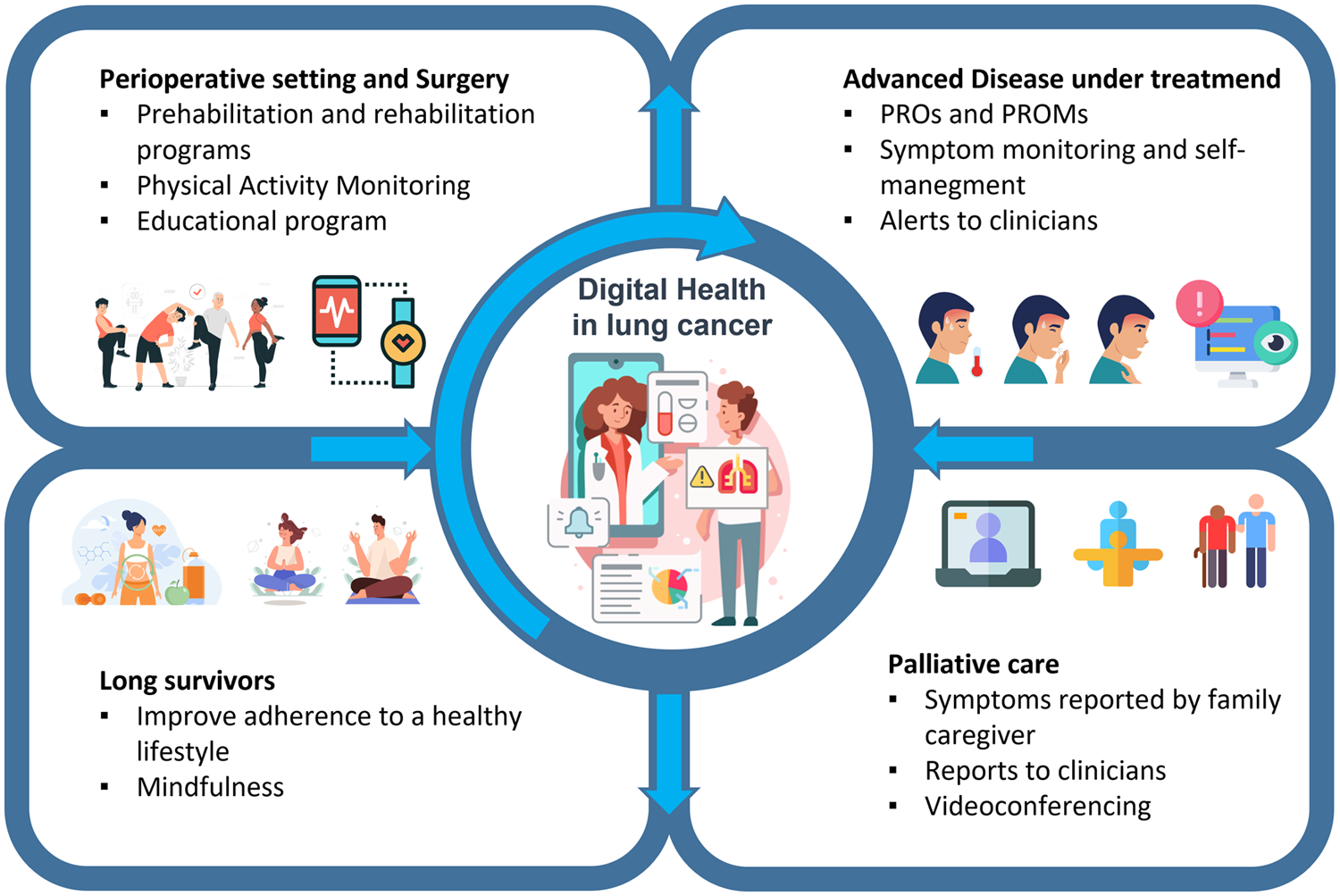
Common functionalities in digital health Applied to lung cancer patients.
m-Health in perioperative setting
Anxiety and distress are frequently associated with early lung cancer (eLC). Several authors have designed a web-based health education program to monitor symptom distress for those patients with a recent LC diagnosis. Huang et al. 18 selected 55 participants with eLC, randomly assigning them to an experimental group (with a web-based health education program, emotional support and personalised recommendations to improve QoL) and a control group. Patients in the experimental group had significantly greater global QoL and emotional function, but no benefits with respect to physical, social and cognitive functions.
An optimisation of the physical condition before and after surgery has been related to a better outcome for those patients undergoing oncological resections. 19
Prehabilitation, or multimodality patient optimisation before major treatment, has demonstrated meaningful improvements in patients’ outcomes after LC-related surgery. 20
According to this, implementing patient-reported outcomes (PROs) programme in surgery may help reduce surgical morbidities. Telemedicine is an interesting tool to control all these PROs as well as enhance personalised lifestyle aspects in perioperative care that could be useful in surgery results. Kneuertz et al. analysed the utility of a mobile Application in patients who were candidates for thoracic surgery. Fifty patients participated in the study, completing preoperative compliance surveys. In-patient questionnaires were also provided regarding compliance with incentive spirometer use and addressing patients’ concerns about self-care after discharge. Postoperative health checks focused on patient-reported symptoms 30 days after surgery (pain and anxiety) were also defined. Authors could demonstrate a significant decrease in maximum pain level (p = 0.002) and anxiety scores (p < 0.001) described over 74% of patients who considered the App very useful in each of the preoperative, in-patient and post-discharge settings. 21
The European Society of Thoracic Surgeons developed a multicentre study with 12 LC-related surgeries and validated questions from the European Organization for Research and Treatment of Cancer Item Bank. An App with this questionnaire was preinstalled in the patients’ tablets. They had to fill out the questions before and after surgery (days 1, 7, 14, 21 and 28). This included 103 patients and the compliance rates were between 90% and 96%. The patients observed a decrease in QoL after surgery. However, a good early compliance with the App by the patients suggested that monitoring symptoms remotely could result in less hospital Appointments. 22
The Fit 4 Surgery App was also designed for patients undergoing lung resections. This mobile App included 10 exercises for 3 min each and contact with health professionals (surgeons, pneumologists and nurses). These results were compared to data from a contemporaneous group of surgery patients included in a standard prehabilitation programme for obstructive lung disease. Authors reported preliminary results with a shorter wait before surgery compared to patients attending rehabilitation, as well as improved walk test distance by 99 ± 83 metres (p < 0.05) before surgery. 23
m-Health after LC surgery
The postoperative setting has a very interesting scope for using Apps to improve outcomes of lung resections, mainly in QoL during the early postoperative period. Different authors have designed several m-Health devices to connect health professionals’ services with patients. The main tool is to get a closer report of symptoms that could be relevant in surgery outcome and could induce a QoL deterioration. De Leeuwerk et al. developed a system of self-monitoring physical activity using an accelerometer in 41 patients who underwent gastrointestinal or LC surgery (mainly lobectomies and segmentectomies). The patients received an ankle-worn accelerometer and the corresponding m-Health App for up to 6 weeks after surgery, and 63% of the participants completed the study with an acceptable System Usability Scale score (77.3) and a favourable perception about their increase in physical activity motivation. 24
Healthcare providers strongly advise that patients who have undergone LC resection engage in physical activity after surgery. Ji et al. recruited 14 participants who underwent LC resection to participate in a 4-week, home-based walking exercise intervention after discharge consisting of one-on-one interviews and the registration of duration and intensity exercise using a sport watch App. They concluded that these programs were feasible and acceptable (12/14 participants reached the goal for exercise duration and intensity), and patients perceived the benefits and motivation to proceed with their exercise plans. 25
The WeChat App-based education and rehabilitation program (WERP) is an integral m-Health App focused on the follow-up of different settings from patients who have undergone non-small cell lung cancer (NSCLC) surgery. This includes assessing things like anxiety, depression, QoL, as well as oncologist surveillance. Two hundred NSCLC patients were randomly assigned to either the WERP group or control group with 48 months of follow-up. The WERP group had lower anxiety (19.0% versus 41.0%) and depression rates (20.0% versus 36.0%) when compared with the control group. The QLQ-C30 scores, a well-known QoL questionnaire, were higher in the WERP group, while the QLQ-C30 symptom score was similar in the WERP group. The authors concluded that WERP is an effective tool for improving QoL after LC surgery. 26
Different studies in the chemotherapy adjuvant setting have been developed monitoring toxicity. The Advanced Symptom Management System (ASyMS) is a mobile App designed to provide real-time, 24-h monitoring and management of chemotherapy toxicity, including a self-reported questionnaire (Daily Chemotherapy Toxicity Self-Assessment Questionnaire) with 10 primary symptoms (nausea, vomiting, diarrhoea, constipation, mucositis, paraesthesia, sore hands/feet, flu-like symptoms/infection, tiredness and pain) and up to six additional symptoms. eSMART is a randomised study focused in evaluating the benefit of the ASyMS in patients with different tumours, including LC, versus standard care in monitoring the impact of burdens of toxicity symptoms on QoL, supportive care needs, anxiety, self-efficacy and work limitations after four to six chemotherapy courses. They found a significant reduction in symptom burden in the ASyMS arm compared to standard care, concluding that this remote strategy will be crucial in the future to optimise symptoms’ burden control. 27
m-Health and LC radiation
Radiation is an alternative treatment for patients with LC. This therapy is associated with different and variable symptoms like dyspnoea, dysphagia, cough, fever, and so on. A recent study explored the feasibility and acceptability in clinical practice of a mobile phone-based, symptoms monitoring system among patients with LC who are receiving radiotherapy and their oncologists. In this study, a significant improvement in anxiety, drowsiness, self-care and self-efficacy were also observed, with a favourable perception from clinicians about how this phone-based symptom of monitoring could contribute to clinical care. 17
m-Health in advanced disease under oncological treatment
Advanced lung cancer (aLC) is associated with a symptomatic disease involving a QoL deficit as well as the deterioration of the patient’s physical condition.
Different treatments in this setting have been related to a high toxicity, mainly chemotherapy regimens, and other combinations associated with poor tolerability. Pulmonary rehabilitation in these patients has been related to QoL improvement as well as symptoms management. A smartphone App based on a 12-week pulmonary rehabilitation program has been tested in 90 patients with advanced NSCLC. In addition to exercise capacity, this App included QoL, symptoms and distress scales. Authors confirmed that this smartphone App-based program was effective, feasible and related to a significant improvement in depression and anxiety, but they did not find a significant change in QoL or pain intensity. 28
The Lung Cancer App (LuCApp) is an ongoing, Italian, randomised study. It included 120 patients with small and NSCLC who received pharmacological treatments for 24 weeks. They were randomised in App monitoring versus standard follow-up. The experimental arm was based on a mobile App (LuCApp). The App had daily monitoring and grading of different symptoms, which triggered predefined alerts to the physician with a specific attention level compared to a control arm based on the standard of care. The primary aim is the change in the score of the Trial Outcome Index in the Functional Assessment of Cancer Therapy Lung Questionnaire from baseline to 12 weeks. 16
IT is a new treatment option for different tumours. In LC, over the last few years, it has become one of the most common therapeutic options, in monotherapy or in combination with chemotherapy. Trojan et al. analysed, in six patients, the usability and acceptance of a smartphone App for monitoring electronically captured PROMs in patients with different primary, PD-L1 positive tumours (lung, prostate and bladder) who have undergone IT (checkpoint inhibitors). In this App, patients reported symptoms and therapy side effects over the course of 3 months. They registered 1279 symptom entries (2.4 per patient/day), with 7.8 being severe, and triggered alerts in four patients; they concluded that those patients using App had high scores in satisfaction and usability scales. 29
Personalised pulmonary rehabilitation in patients with aLC is another scenario to explore the role of an App (EFIL BREATH). It is focused on replacing presential rehabilitation for a new mobile App with real-time information. Patient’s mobiles capture health data in different exercises consisting of individual or group rehabilitation. Health professionals received this information and made adequate recommendations optimising the exercise’s programme. They observed that this m-Health system was feasible for improving symptoms that pertained to QoL. 30
Palliative care in m-Health and LC
Controlling symptom distress has been one of the most frequent aims in e-Health platforms. Family caregivers have the potential to help patients with symptoms management, mainly in their end of life. e-Health systems could be useful in this setting. Gustafson et al. developed a pooled analysis from two randomised clinical trials including the Comprehensive Health Enhancement Support System (CHESS), an electronic tool to help families and patients who are in home palliative care. These studies compared CHESS versus CHESS adding to clinician reports involving and automatic alerts system attending by clinicians. They observed that an e-Health tool that was able to produce alerts and clinicians’ interventions significantly reduced patient distress. 31
Chua et al. designed a multicentre comparative study between two modalities of early palliative care. They compared early palliative care through a telehealth strategy versus in-person treatment for patients and caregivers focused on treating aLC. The authors hypothesise that both modalities would be equivalent for improving patient QoL and avoiding patients’ hospice attendances. However, this is an ongoing, ambitious study with potentially more than 1000 patients. 32
m-Health and long-term LC survivors
The number of long-term LC survivors has increased in recent years since new therapies have been included in clinical practice. Oncologists and primary care doctors provide different recommendations for improving patients’ lifestyles as well as optimising their health condition; however, the adherence to this advice is low in this population. Some m-Health Apps, like Breathe Easier, are oriented towards mindfulness strategies and have been tested in long-term LC survivors and their families with a good acceptance rate and satisfaction level. 33
iEXHALE is an exercise App for LC survivors that aims to increase exercise activity and improve patients’ symptoms. The aim is to know whether this App is usable and could provide physical, psychosocial and emotional relief to patients. 34
Impact of m-Health Apps on QoL
QoL is related to multiple domains of health and is one of the most important factors to consider in these patients. Meta-analysis studies and systematic reviews have estimated the impact using e-Health and m-Health has on the QoL of cancer patients.35–39
The most widely used QoL assessment questionnaires are those from the European Organization for Research and Treatment (EORTC) and the Functional Assessment of Cancer Therapy (FACT). Different interventions were associated with improvements in health status scores pertaining to physical, functional and cognitive functions. A study using wearables and a mobile App that included a rehabilitation exercise program and disease information with 102 colorectal cancer patients receiving chemotherapy after 12 weeks showed improvements in EORTC fatigue symptoms. 40
Another study in patients with LC found that, where the physical rehabilitation program was also administered through a mobile Application, there were improved scores on the subscales of emotional and social functioning, fatigue and other symptoms of the ERTC-QLQ-C30. 28
In a randomised study of a m-Health App that provided treatment recommendations and information for patients with different types of cancer, at their 4-week follow-up, the patients in the experimental group had significantly higher scores in the emotional, cognitive and social domains of the EORTC QLQ-C30. 41
As relates to the dimensions of the emotional and general well-being FACT-G, studies have evaluated the psychosocial intervention administered using Apps on mobile devices, with significant improvement in reducing anxiety and levels of depression in patients with advanced cancer and in active control. 42
In most of the discussed studies, the evidence supports the assertion that e-Health interventions such as m-Health hold promise for improving the QoL of cancer patients. However, studies with a larger sample size and longer follow-up periods are needed in order to reinforce the clinical results. Ideally, m-Health interventions should be tailored to individual patient needs based on cancer progression and treatment side effects.
m-Health and cost-effectiveness
A recent debate about potential cost reductions in medical assistance through e-health tools is very exciting, mainly in regard to a geometrical increase in cancer costs: more treatments and cancer prevalence increase. In several chronic diseases, like nephropathy, heart disease, rheumatological illness, mental disorders, and so on, significant cost reductions have been demonstrated.43,44
In the LC setting, a reduction in hospital visits, patients’ controlling of symptoms, alerts to secondary professional actions, and so on are some of the strategies favoured by these tools that could optimise costs management. In a French multicentre, randomised clinical trial of the overall survival benefit of a web involved in PRO-based surveillance for LC patients was compared to a conventional surveillance. This medical economic analysis found a €362/per patient lower annual cost in the e-health arm (€941/year/patient) compared to the control group (€1304/year/patient). 9
The postoperative cancer setting is also a potential scenario where telemedicine could be more cost efficient compared to routine practice. Recent research focused on patients undergoing surgery (cancer surgery was also included) who were randomised to an interventional arm with a video telemedicine follow-up visit in their home versus the standard face-to-face visit in the 90 days following surgery. Different economics parameters were analysed (cost of travel, accommodations, meals and missed work), and they concluded that those patients who utilised video telemedicine rather than face-to-face clinic time had better cost efficacy parameters. In addition, face-to-face interviews showed a higher satisfaction level of video telemedicine, postoperative, follow-up visits during the 6-year period of study. 45
A Dutch, multicentre, randomised controlled study based on a nurse-led, stepped-care, e-health intervention with 12 month follow-up was designed to enhance the return to work of patients with cancer. Patients were randomised to either the nurse-led, stepped-care, e-health intervention (Cancer@Work) or standard care with a primary outcome. This division was based on the proportion of patients who had a sustainable return to work as well as direct and indirect cost reductions with the intervention. Protocol is already reported, but results are pending. 46
m-Health and LC prognosis
As has been previously described, e-health tools are fashionable and potentially useful in cancer, including in treating LC patients. However, solid evidence about their impact on prognosis is not yet available. Many studies have investigated the determinants of limited digital health literacy, the association between frailty factors and prognosis that has never been assessed. No specific LC studies analysed the impact of these tools on survival; the majority of the studies are focused on different types of cancer.
A retrospective, non-interventional study with more than 15,000 adults with cancer were analysed in a French hospital. They had a limited e-health literacy (absence of an email address in the electronic patient record). They found that those patients with email address showed a significantly better overall survival (p < 0.001) in univariate and multivariate analyses when compared to those without one. 47
Basch et al., several years ago, carried out a prospective randomised study where participants diagnosed with cancer and in active treatment were assigned to either the standard care group or to the PRO group (an interventional arm with self-reporting of 12 common symptoms from the National Cancer Institute’s Common Terminology Criteria for Adverse Events) with visits via a web-based PRO platform. If the PRO group reported a severe or worsening symptom, an email alert was triggered to a clinical nurse, generating clinic visits with the oncologist, whereas the control arm received the standard procedure for monitoring symptoms. They found that the median overall survival time was 31.2 months (95% confidence interval (CI), 24.5–39.6) in the PRO group and 26.0 months (95% CI, 22.1–30.9) in the standard group (difference, 5 months; p = 0.03). In the multivariable model, there was a trend to remain statistically significant with a hazard ratio of 0.83 (95% CI, 0.70–0.99; p = 0.04). 48
More authors, like Denis et al., also demonstrated a correlation between e-Health strategies and survival. They found that an intensive follow-up of patients’ symptoms could help detect recurrences and clinical complications via a web-based App (MoovcareTM, CORIA UMR 6614-Normandie université, CNRS - université et INSA de Rouen, campus universitaire du Madrillet, F-76800 Saint-Étienne du Rouvray, France). In nearly 300 patients in four prospective studies, including one pilot trial, they showed a 27% survival rate at 1 year. Later, a randomised phase 3 trial demonstrated a 26% 1-year survival improvement as compared to a conventional follow-up. 49
Finally, a French study also found a survival benefit in patients with LC, including in a protocol (Sentinel online system) to self-report their symptoms. They compared this strategy to the traditional manner and found a significant benefit in survival: 19 months versus 12 months, in favour of the self-reporting system.
Furthermore, by using this new type of surveillance, the costs were reduced as well. 50
One of the most important limitations for this review is the variability of quality of the studies reported: centre experiences, usability and feasibility studies, pilot studies, case–cohort studies and a very few number of clinical trials have been reported. The lack of solid evidence about the real impact of these type of tools on clinical practice is a limitation as well.
Conclusions
In recent years, telemedicine – mainly m-Health tools – have experienced an increasing interest in LC patients’ care in different settings: perioperative, oncological treatment and surveillance. Real-time remote PROMs control as well as bi-directional interaction between patients and health professionals could have a positive impact on QoL, optimising symptom detection and control, reducing ER visits and hospitalisations and promoting healthy lifestyle habits. One of the most important limitations in m-Health is the challenge of the integration of all e-Health systems in routine electronic medical reports. Efforts in this regard are a major need in completing the incorporation of telemedicine into routine clinical practice.
Footnotes
Author contributions
MS has involved in analysis, investigation, methodology and resources, total supervision, writing, review and editing of the final manuscript. JMI-C has involved in analysis, investigation, writing, image preparation, review and editing the final manuscript. BG-R has involved in analysis, investigation, writing, table preparation, review and editing of the manuscript. EJG has involved in supervision of the technical context and review of the final manuscript. ECS has involved in supervision of the clinical context and review of the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work has been supported by the ALIBIRD2020-CM programme (S2018/BAA-4343): ‘Precision Nutrition Therapeutic Formulas for Cancer’ which has been funded by the DG for Research and Innovation of the Community of Madrid (DGII) and co-financed with EU Structural Funds.