
Abstract
Objective:
Mediastinoscopy as diagnostic procedure for evaluation of mediastinum in patients with non-small-cell lung cancer has long been considered the reference standard. However, less invasive method has occurred. Endobronchial ultrasound–guided transbronchial needle aspiration came into widespread use and has resulted in controversy as to whether it is a good replacement for mediastinoscopy. We chose to demonstrate the usefulness of endobronchial ultrasound–guided transbronchial needle aspiration in evaluating the mediastinum in patients with non-small-cell lung cancer.
Material and methods:
Over a 48-month period, 1841 patients underwent endobronchial ultrasound–guided transbronchial needle aspiration at our healthcare centre. In all patients, 2964 biopsies from the lymph node group N2 and 783 from group N1 were taken. The mean short axis of the lymph nodes biopsied was 2.0 (range: 0.6–2.6). The mean number of lymph node stations biopsied per patient was 2.6. Patients with a negative result of endobronchial ultrasound–guided transbronchial needle aspiration underwent mediastinoscopy. All patients with a negative result in endobronchial ultrasound–guided transbronchial needle aspiration and mediastinoscopy underwent surgical resection with lymph node sampling.
Results:
The metastases to lymph nodes N2/N3 and N1 were found in 1111 (60.3%) and 199 (9.3%), respectively. Mediastinoscopy was performed in 730 patients with a positive result in 83 (11.4%) patients. In the group of operated patients, metastatic N1 disease was found in 264 (14.1%). In the group of the operated patients, mediastinal involvement of disease (N2) was found in 30 patients (4.5%). The sensitivity, negative predictive value and diagnostic accuracy for hilar lymph node staging for endobronchial ultrasound–guided transbronchial needle aspiration were 57%, 96% and 96%, respectively. The sensitivity, negative predictive value and diagnostic accuracy per patient for mediastinal lymph node staging for endobronchial ultrasound–guided transbronchial needle aspiration and mediastinoscopy were 91%, 85%, 93% and 73%, 95.5%, 97%, respectively. The specificity and positive predictive value of both tests were 100%.
Conclusion:
The clinical usefulness of endobronchial ultrasound–guided transbronchial needle aspiration is undeniable according to diagnostic performance data. Endobronchial ultrasound–guided transbronchial needle aspiration should be considered complementary to mediastinoscopy in the evaluation of patients with radiographically abnormal mediastinum.
Keywords
Background
Non-small-cell lung cancer (NSCLC) frequently metastasizes to the mediastinal lymph nodes, representing a process that affects the tumour stage and the treatment strategy. Staging of lung cancer is defined by TNM classification. 1 Usually, patients are considered surgical candidates when there is no mediastinal involvement (N2–3) or distant metastasis. Sometimes, surgery may also cure the disease when metastases are limited to ipsilateral lymph node (N2). Surgery is contraindicated when there is an extensive (bulky) N2 or N3 or metastatic disease. In those cases, patients are directed to oncologist for chemotherapy or chemo-radiotherapy. Positron emission tomography (PET)–computed tomography (CT) used in screening for mediastinal lymph node metastases with its high sensitivity (60%–85%), specificity up to 94% and an accuracy of 78%–96% is the most effective, non-invasive method of staging of lung cancer.2–4 If the presence of metastatic disease is suspected in radiological findings, confirmation by biopsy or further diagnostic imaging modalities is required.5,6 Mediastinoscopy is regarded as the gold standard for the diagnosis of lymph node metastasis in patients with NSCLC. 7 As demonstrated by large single-institution study, mediastinoscopy with its sensitivity of 86%–93%, diagnostic accuracy 93%–96% and negative predictive value (NPV; 80%–99%) 8 is characterized by small amount of complications. Its morbidity rate reaches 0.6%–1.1% and mortality rate is 0.05%–0.2%. An alternative option for mediastinoscopy is endobronchial ultrasound–guided transbronchial needle aspiration (EBUS-TBNA) that can be performed under local anaesthesia. In some studies, the effectiveness of EBUS-TBNA is comparable to that of invasive diagnostic modalities and was shown to reach the level of 85%–100%, specificity of 100% and accuracy of more than 96%. 9 Some authors suggest mediastinoscopy replacement with EBUS-TBNA and introduced the term ‘medical’ mediastinoscopy. 10 In this study, we performed a retrospective chart review to clarify the usefulness of EBUS-TBNA in lymph node staging of NSCLC.
Material and method
Ethical approval
Due to the fact that this study was based on standard procedures performed at our institution, Ethics Committee of National Research Institute of Chest Diseases, Warsaw, Poland, waived the need for ethic approval for the study. All patients were fully informed about potential risk and advantages of our study. The Informed Consent Form for participation in the study including bronchoscopy and biopsy was signed by all the subjects.
Population
Over a 48-month period, 1841 patients with suspected or proved NSCLC underwent EBUS-TBNA for lymph node staging. Standard bronchoscopy was performed in all patients with a biopsy of the affected part of the lung. All patients had CT examination before invasive procedures. Patients with lymph nodes equal or more than 10 mm in diameter in CT scan were qualified to EBUS-TBNA. Before the biopsy, radiologists assessed the diameter and the structural pattern of the enlarged lymph nodes to assess probability of lymph node metastasis. Some patients had PET–CT scan examination (36%). It was not a standard procedure. All lymph nodes positive in PET–CT were biopsied. Diagnostic accuracy, sensitivity, specificity, positive predictive value (PPV) and NPV were calculated in the group of patients who had a diagnostic EBUS-TBNA cytology (positive or negative) and available reference pathologic testing. Almost all patients with negative results of EBUS-TBNA were directed for mediastinoscopy. Everyone with negative results in EBUS-TBNA and mediastinoscopy underwent surgical resection with lymphadenectomy. Only a small subgroup of patients (n = 21) with negative results in EBUS-TBNA had the surgical resection without previous mediastinoscopy. Pathological examination of the lymph nodes taken during surgery was compared with the results of endobronchial ultrasound biopsies to assess the effectiveness of EBUS-TBNA.
Lymph node sampling
The equipment included Pentax ultrasonic bronchoscope EB 1970UK, EPK-1000 video processor, EBUS Hitachi HI Vision-5500 processor and convex probe linear array endobronchial ultrasound bronchoscope (Olympus XBF- UC260F-OL8; Olympus Ltd, Tokyo, Japan). A dedicated 22-gauge needle was used for lymph node sampling. Needle aspiration of the largest accessible lymph nodes was performed during the ultrasound examination. Biopsy concerned only those lymph nodes that were considered abnormal in CT scan or PET–CT (targeted biopsy), not routinely performed biopsies of normal mediastinal lymph nodes in patients with confirmed radiologically stage N1 of disease. The internal stylet was removed after the initial puncture, and negative pressure was applied with a syringe. Using this method, histologic cores as well as cytologic specimens could be obtained. The aspirated material was smeared onto glass slides, and smears were fixed in 95% alcohol. Furthermore, Papanicolaou staining and light microscopy were performed by an independent cytopathologist. Histologic cores were fixed with formalin and stained with haematoxylin and eosin. Immunohistochemistry was also performed, if necessary.
Mediastinoscopy
Standard cervical mediastinoscopy was performed after previous negative EBUS-TBNA biopsy except in 21 patients. It was done in the operating room under general anaesthesia. Sometimes, mediastinoscopy was performed as a separate procedure or sometimes just before thoracotomy. Biopsies from station 4R, 7 and 4L were routinely obtained. Biopsies were also obtained from other locations when lymph nodes were identified.
Thoracotomy
If there was no evidence of N2 or N3 disease on the mediastinoscopy after previous negative EBUS-TBNA biopsy, patients underwent surgical resection of the tumour at the same anaesthetic time. Pulmonary resection and systematic nodal dissection were performed in every patient by a thoracotomy or video-assisted thoracic surgery. The results of the surgical pathology were subsequently correlated with the results from the EBUS-TBNA and mediastinoscopy.
Statistical methods
Sensitivity, specificity and accuracy were calculated using the standard definitions. The NPV was calculated using the following formula: number of true negatives/(number of true negatives + number of false negatives). The resulting NPV was expressed at 95% confidence interval.
Results
Over a 48-month period, 1841 patients underwent EBUS-TBNA at our healthcare centre. The male-to-female ratio was 1.6:1 and the median age was 65 years, ranging from 32 to 87 years. Adenocarcinoma was diagnosed in 1100 patients (59.8%) and squamous cell carcinoma in 652 patients (35.4%). Other types of cancer were diagnosed in 89 patients (4.8%). PET–CT was performed in only 644 (35%) patients, with suggestion of lymph node metastasis in 179 (27.7%) cases. The average standardized uptake value (SUV) of 18-fluorodeoxyglucose was 3.6 (range: 2.3–5.8). The mean short axis of the lymph nodes biopsied was 2.0 (range: 0.6–2.6). In all patients, 2964 biopsies from lymph node group N2/N3 and 783 from group N1 were taken. The mean number of mediastinal and hilar lymph node stations biopsied per patient was 2.6 (range: 2–6). The most often biopsied groups of mediastinal lymph nodes were 7 and 4R.
In the group of 1841 patients who underwent EBUS-TBNA, metastases to lymph nodes N2/N3 were found in 1111 (60.3%) patients. This group included 157 patients (8.5%) with centrally located tumour end enlarged lymph node group N1 where CT and PET–CT showed no enlarged mediastinal lymph nodes. In all cases, biopsy was performed on lymph node group N2 on the side of the tumour. In 21 cases (13.4%), the presence of metastases was confirmed (Table 1).
Number of LN biopsied in EBUS-TBNA and the results.

LN: lymph node; EBUS-TBNA: endobronchial ultrasound–guided transbronchial needle aspiration.
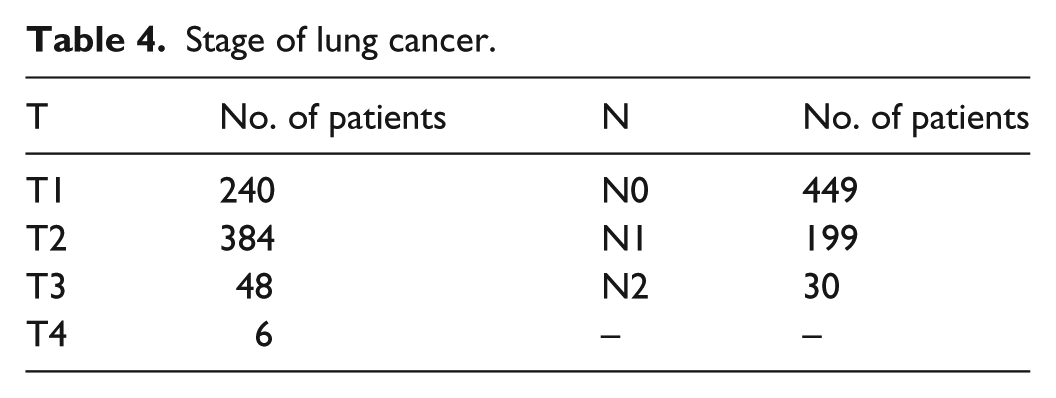
Mediastinoscopy was performed in 730 patients with a negative result in EBUS-TBNA and a positive result in 83 (11.4%) patients (Table 2). A total of 647 patients (35.1%) had a negative result of mediastinoscopy and were qualified to surgery. Only a small subgroup of patients (n = 21) had a resection after a negative result of EBUS-TBNA without previous mediastinoscopy. Overall, 668 patients (36.3%) had a surgical resection (561 lobectomy, 53 bilobectomy, 34 pneumonectomy, 21 wedge resection and 8 segmentectomy) (Tables 3 and 4). In the group of the operated patients, mediastinal involvement of disease (N2) was found in 30 patients (4.5%). The sensitivity, NPV and diagnostic accuracy per patient for mediastinal lymph node staging for EBUS-TBNA and mediastinoscopy were 91%, 85%, 93% and 73%, 95.5%, 97%, respectively. The specificity and PPV of both tests were 100% (Tables 5 and 6). There were no major complications of EBUS-TBNA. In more than half of patients, minor complications occurred, including extensive cough and mild haemoptysis during 24-h period after examination.
Comparison of the results of EBUS-TBNA and mediastinoscopy.
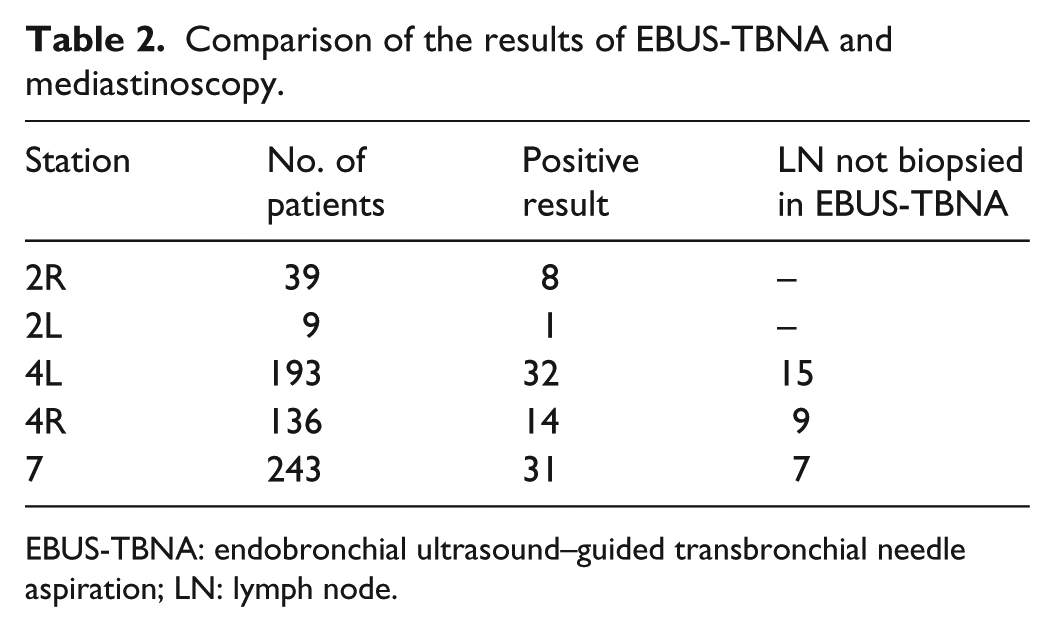
EBUS-TBNA: endobronchial ultrasound–guided transbronchial needle aspiration; LN: lymph node.
Type of resections.

Stage of lung cancer.
N1 disease found in postoperative results.

LN: lymph node; EBUS-TBNA: endobronchial ultrasound–guided transbronchial needle aspiration.
N2/N3 disease in postoperative results.
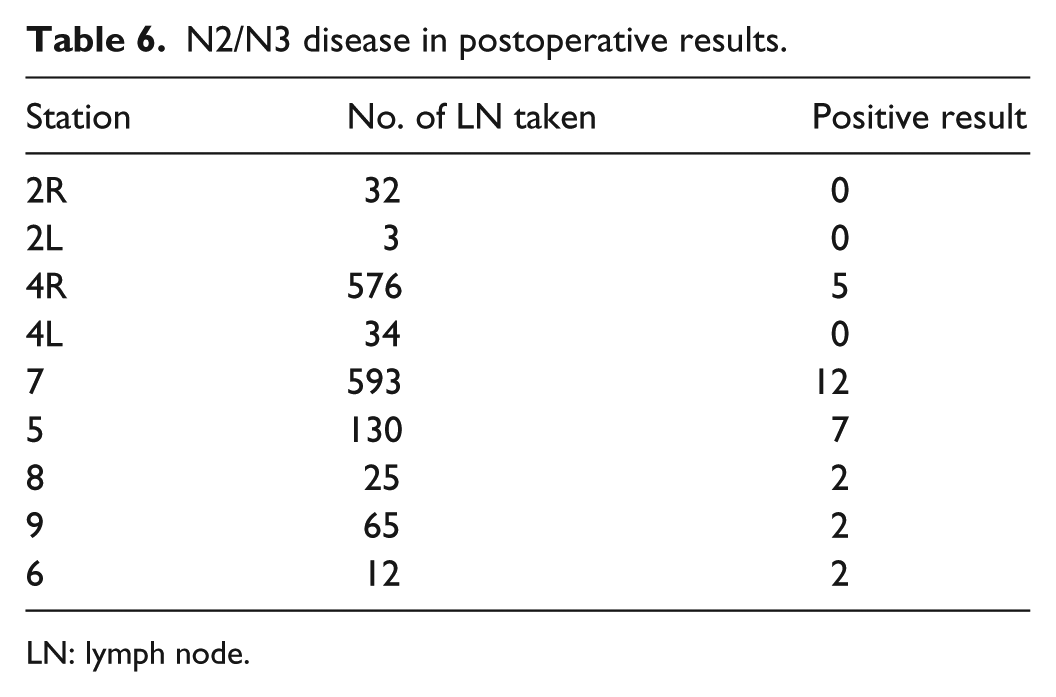
LN: lymph node.
Discussion
Treatment of lung cancer is entirely dependent on the stage. An important element of lung cancer staging is the presence of metastases to the mediastinal lymph nodes. Determination of the presence of metastases to the mediastinum is usually a contraindication for a radical surgery. Considerable progress in the staging, including CT scans and PET–CT scans, significantly improved the accuracy of invasive diagnostic procedures. The data analysis indicates that the sensitivity and specificity of both CT and PET–CT in the evaluation of metastases to mediastinal lymph nodes are relatively low and reached 74% and 69% and 74% and 84%, respectively. 5 Moreover, in N1-positive and N2-negative patients, metastases to N2 lymph nodes were found in PET–CT in 16% of cases. 6 In a prospective comparative study of 102 NSCLC patients, EBUS-fine-needle aspiration (FNA) had superior sensitivity, specificity and diagnostic accuracy as compared with either CT or standalone PET–CT. 11 In this material, a PET–CT was not performed as a standard procedure in all patients, and the rate of the subjects was only 35%. Especially at the beginning of the study, this rate was low due to poor accessibility of this examination. According to the current guidelines, the diagnostic value of EBUS-TBNA following PET/CT scanning is superior comparing to EBUS-TBNA alone. Similarly, as in the literature, adenocarcinoma was a predominant histological type (59.8%). The correlation between sensitivity of EBUS-TBNA and histological type of tumour was not assessed. Rapid on-site evaluation was not available; however, occasional samples were immediately sent to pathology. Most authorities in the field of thoracic diseases are of the opinion that patients with enlarged lymph nodes on CT or suspected in PET–CT and patients with centrally located tumours should undergo invasive staging. 1 To achieve this, mediastinoscopy has been the traditional approach; however, various less invasive methods including transbronchial needle aspiration, endoscopic ultrasound (EUS), EBUS and the combination of EUS and EBUS have emerged as potential alternatives. Vincent et al. 9 reported that surgical staging procedures were avoided in 43% of patients who underwent EBUS-TBNA. In this study, the authors showed that up to 56.3% patients were staged successfully with EBUS-TBNA, avoiding more invasive procedures. The effectiveness of EBUS-TBNA is correlated with the number of lymph nodes biopsied. In previous studies, the average number of mediastinal nodes sampled ranged between 1.1 and 2.9. 12 In this study, the mean number of lymph node stations biopsied per patient was 1.6. Some authors suggest that two aspirations per lymph node station can be accepted when at least one tissue core specimen is obtained by the first two aspirations. 13 Endobronchial ultrasound–guided FNA is a safe technique for thoracic malignancy staging and assessing mediastinal adenopathy.12,14 Growing number of studies have now been reported in the literature, all without significant complications. 11 Endobronchial ultrasound–guided FNA is superior to radiographic staging techniques. 15 Comparing studies of several major centres, it is concluded that the sensitivity, specificity and accuracy of EBUS-TBNA range from 88.1% to 99.1%, 100% and 96.3% to 98.7%, respectively. 16 The authors confirm the results of other data presented in the literature. In this study, the sensitivity and diagnostic accuracy per patient for mediastinal lymph node staging for EBUS-TBNA and mediastinoscopy were 91% and 93%, respectively. The specificity and PPV were 100%. Vilmann and Puri 10 presented their findings on a selected group of patients by combining EBUS-TBNA and EUS-FNA to achieve 100% sensitivity and specificity of the method. These results were better than the results for mediastinoscopy. The authors suggest that the combination of EUS-FNA and EBUS-TBNA will replace more invasive methods, such as mediastinoscopy, in diagnosis and staging of lung cancers in the near future. Other authors expressed much less enthusiastic opinions. In the present material, the percentage of positive results mediastinoscopy was only 11.4%. In view of our results presented, mediastinoscopy in patients with negative EBUS-TBNA is controversial. Although in accordance with the recommendations of the European Respiratory Society (ERS)/European Society of Thoracic Surgeons (ESTS) for mediastinal nodal staging in patients with suspected or proven NSCLC with abnormal mediastinal and/or hilar nodes at CT and/or PET, subsequent surgical staging is recommended, when endosonography does not show malignant nodal involvement. 17 Another interesting issue is the importance of EBUS-TBNA and biopsy of mediastinal lymph nodes in patients with centrally located tumours and enlarged nodes of group N1. In our study, positive results of N2 lymph node biopsy were obtained in 13.4% of patients, although this procedure was not performed routinely. This indicates that in these patients, EBUS-TBNA with mediastinal lymph node biopsy should always be performed. If endosonography does not show malignant nodal involvement, mediastinoscopy should be considered. This observation is identical to the recommendation of the ERS/ESTS.
An important indicator of the effectiveness of EBUS-TBNA is the NPV. In the literature, NPV percentage ranges from 14% to 97%. 13 The study of Cerfolio et al., 18 the percentage NPV for EBUS-TBNA for node groups 4R/4L and 7 was 79% and for EUS-FNA 80%. However, this percentage value was much higher for mediastinoscopy and reached 88%. The authors concluded that mediastinoscopy is still required for patients with suspicious nodal disease in these stations. Although the percentage of NPV was 85% in this study, we found that only 11.5% patients with negative result of EBUS-TBNA had positive result in mediastinoscopy. Despite the use of EBUS-TBNA and invasive methods, the rate of unexpected N2 disease still remains the problem. De Leyn et al. 8 showed unexpected N2 rate of 14.5% at thoracotomy in patients who underwent mediastinoscopy alone. However, using EBUS-TBNA and mediastinoscopy for staging, the percentage of unexpected N2 may still be relatively high, reaching 10%. 19 In our study, the percentage of unexpected N2 was relatively low and reached up to 4.5%. The only rational explanation for this fact is the large proportion of patients with confirmed N2 using EBUS-TBNA (60.3%), despite the fact that targeted biopsies were performed only in abnormal lymph nodes in the CT studies and/or PET–CT.
As explained by Cerfolio et al., 18 it depends on the endoscopist’s experience, patient selection and completeness of mediastinal nodes removed during thoracotomy. In most centres, CT is the initial method for assessing mediastinal nodes, and lymph nodes with a short axis diameter >10 mm are considered abnormal. Herth et al.20,21 found metastases in 9 of 97 patients who underwent EBUS-TBNA with lymph nodes less than 10 mm in diameter and negative PET–CT. The authors of this study suggest that patients with normal CT and PET–CT findings of the mediastinum can be primarily evaluated and staged during diagnostic bronchoscopy with EBUS-TBNA of all nodes >5 mm, especially if it is known to be adenocarcinoma. This confirms that the now commonly used criteria for EBUS-TBNA were insufficient. With no doubt, with the increase in effectiveness of PET–CT and experience of staff in the endoscopy, the rate of unrevealed N2 will decrease. The completeness of lymphadenectomy during thoracotomy should be the highest. Apart from the undeniable advantages, EBUS-TBNA also has its limitations, most notably the inability to biopsy the node stations 5, 6 and the lower mediastinum. This disadvantage can be excluded if EBUS-TBNA and EUS-FNA are combined. In conclusion, EBUS-TBNA is a useful modality for the diagnosis of mediastinal or hilar lymph node metastasis in patients with NSCLC, and it is therefore useful in making treatment decisions. We believe that accurate evaluation of mediastinal and hilar lymph nodes by EBUS-TBNA enables appropriate selection of surgical candidates and clarifies the significance of surgical treatment for NSCLC.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.