
Abstract
A substantial percentage (8%) of all newly diagnosed cancer cases are in patients with previous tumours, with a similar trend in lung cancer. Cases of multiple primary lung cancer (MPLC) are increasing worldwide, due to improved diagnostic and surveillance mechanisms and the ageing population. Diagnosis of MPLC is complicated by difficulties in distinguishing it from lung cancer metastasis. Clinicopathological assessment, diagnosis and management have evolved, but remain severely limited by the lack of robust and dependable molecular markers for the differential diagnosis of metastasis and MPLC. This systematic review evaluates diagnostic criteria for MPLC, and the subsequent management and success rates. The incorporation of molecular biology techniques into the diagnostic process for MPLC is also discussed.
Introduction
Lung cancer is the leading cause of cancer death worldwide in both sexes, 1 with an estimated 1.4 million deaths each year. 2 An estimated 1.6 million new cases of lung cancer were diagnosed worldwide in 2008, accounting for about 13% of total cancer diagnoses in that year. 1 In Europe, lung cancer represents 12% of an estimated 3.2 million cancer cases. 3 The expected incidence of lung cancer in the USA in 2011 was 221 130, accounting for 14% of all cancer diagnoses. 4 The alarming nature of these numbers is highlighted by the fact that rate of death from lung cancer is greater than the next three most common cancers combined (colon, breast and prostate cancer); the 5-year survival rate for lung cancer is ∼15%. 5
Approximately 8% of all newly diagnosed cancers are in patients with a prior personal history of primary cancer, 6 representing around 900 000 new multiple cancer cases globally (8% of 10.9 million cases). 7 The numbers of such cancers are increasing, mainly due to the ageing population: only 5–12% of cancer patients aged 50–64 years were previously diagnosed with cancer, versus 12–26% of those aged > 80 years. 8 Improved treatment strategies and increased cancer awareness and surveillance contribute to this rising prevalence. The resultant healthcare burden of this trend is profound, 9 and multiple primary cancer has assumed great importance in policy decisions, as well as in epidemiological and clinical research.
Lung cancer has two main types: small cell lung cancer (SCLC; or oat cell cancer), which accounts for 20% of all lung cancer cases; 10 and nonsmall cell lung cancer (NSCLC; 80% of cases). 10 The less-common SCLC is highly tumourigenic and metastatic in the primary and secondary bronchi, and is classically correlated with smoking and neuroendocrine factors. 6 NSCLC is classified into three major histological subtypes: (i) squamous cell carcinoma (25%); (ii) adenocarcinoma (40%); (iii) large cell lung carcinoma (15%). 6
The diagnosis of a second primary lung cancer is complex for several reasons. These include: difficulties in differentiating between metastatic and primary lesions if the latter occurs within 2 years of the initial tumour; both the second primary lesion and initial tumour being of a similar histological subtype; the second lesion being located in an area of previous radiotherapy, since changes in the tissue morphology can complicate the differential diagnosis of metastases and primary cancers.
The concept of multiple primary lung cancer (MPLC) was introduced in 1924. 11 Patients with successfully treated NSCLC or SCLC remain at risk of developing a secondary tumour at a distant site through metastasis via the lymphatic or circulatory system. 10 Second primary tumours are either synchronous (detected or resected simultaneously) or metachronous (detected some time after the primary lesion). The incident mechanism determines the subsequent management strategy.7,8
Clinicopathological criteria for differential diagnosis of multiple primary lung cancer (MPLC) from metastatic lung cancer.
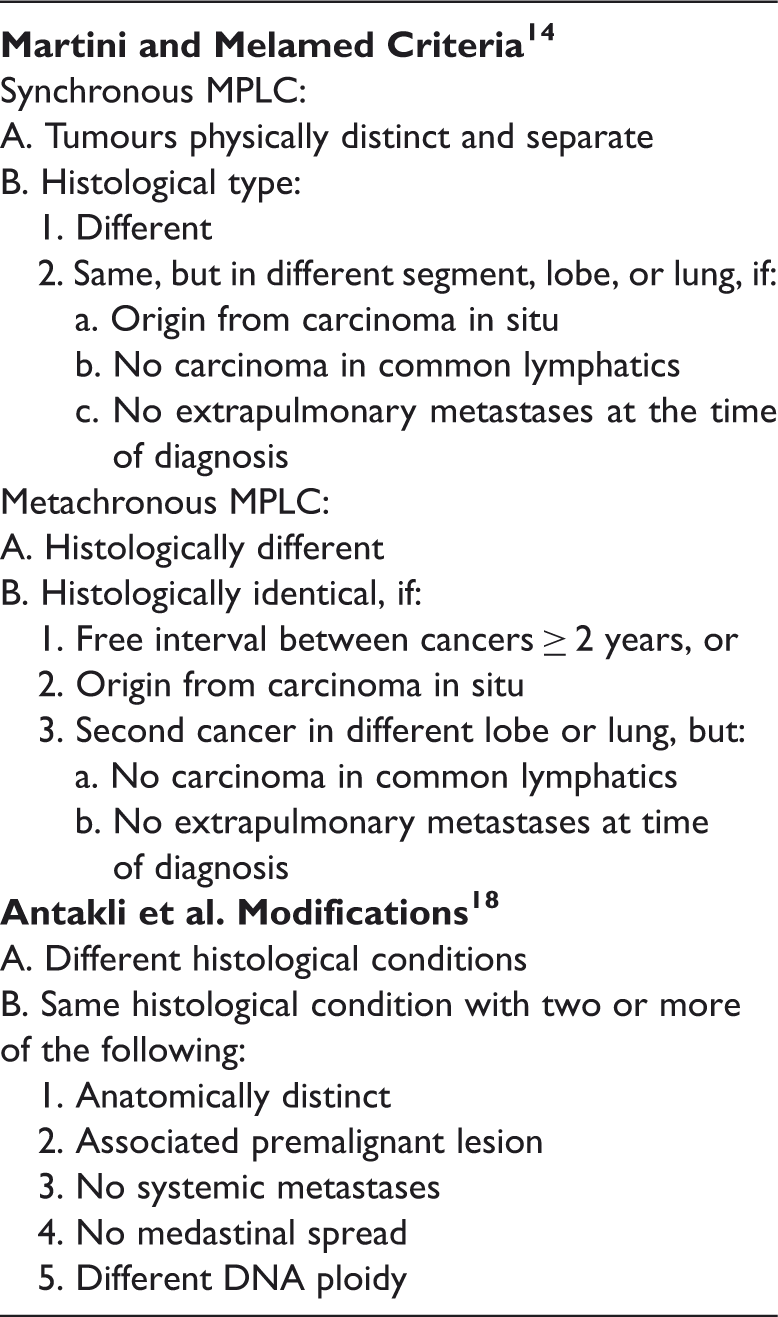
The Martini and Melamed criteria 14 are based on tumour characteristics (inclusive of, but not limited to, morphology, location, presence or absence of carcinoma in situ, vascular invasion and metastasis), but lack the power to differentiate between metastasis and a second primary lung cancer.16,17 Antakli et al. 18 added DNA ploidy testing to the original criteria 14 as an aid to differentiating tumour types (Table 1). Such analysis is time consuming and lacks sensitivity, and is therefore not widely adopted in clinical settings. There remains a need for more robust and straightforward diagnostic tools. Our study of the use of computed tomography (CT) images showed that diagnosis of synchronous MPLC might be delayed or mistaken for intrapulmonary metastasis, and that the malignant characteristics of primary lung cancer lesions may provide valuable diagnostic clues. 19 Although the introduction of more sensitive CT or positron emission tomography scanning and fluorescence endoscopy (together with increased surveillance) have improved the detection of MPLC,15,20–23 there remains a lack of uniform guidelines for MPLC diagnosis.
The current systematic review will discuss the criteria used to differentiate multiple primary NSCLC from metastatic NSCLC at the clinical level, as well as current treatment strategies. The use of novel molecular techniques for distinguishing between MPLC and metastatic tumours will be discussed.
Search strategy
Electronic databases (Ovid Medline®, Ovid Embase®, Scopus® and Cochrane Database) were searched to identify relevant articles, with the date range between January 1975 and December 2011. Database-specific controlled vocabulary and general free-text terms were both used, to maximize retrieval. MeSH terms were “second primary lung cancer”, “multiple primary lung cancer”, “MPLC”, “synchronous lung cancer” and “metachronous lung cancer”. Searches were limited to full-text articles with human participants. Hand searching of key article reference lists was used to locate additional relevant articles. Eligibility assessment and data abstraction were both performed independently, in an unblended standardized manner, by two independent reviewers (X.X. and Y.L.). Results of all searches were combined and duplicate articles were removed. Inclusion criteria were: (i) description of study design; (ii) patient data (number of included patients, mean age, sex); (iii) type of diagnostic criteria and/or intervention strategy used; (iv) timing of determination; (v) diagnosis of NSCLC. Exclusion criteria were: (i) studies reporting patients aged ≤ 21 years; (ii) history of other cancer diagnosis; (iii) initial diagnosis >12 months from study entry date; (iv) history of chemo- or radiotherapy.
Results
The search identified 215 articles, of which 203 were excluded (Figure 1). Basic characteristics of the remaining 12 articles are shown in Table 2.12,14,16,18,24–31
Flow diagram presenting the results of a literature search and study selection process for a systematic analysis of published studies on the diagnosis of multiple primary nonsmall cell lung cancer. Studies included in a systematic review of the literature regarding diagnosis of multiple primary nonsmall cell lung cancer. aCGH, comparative genomic hybridization array. Note: The ‘n’ column contains different numbers, compared with those listed for the specific multiple primary tumour types, because for some studies the entire cohort was analysed, whereas for others a small subcohort of a larger study was analysed. This selection was dictated by the inclusion criteria, as described in the search strategy.

Martini and Melamed 14 used histological differences/similarities, origin from carcinoma in situ, lack of carcinoma in the lymphatics common to both tumours, and absence of extrapulmonary metastases to differentiate between metachronous and synchronous lesions. In addition, being located in separate, physically distinct sites was indicative of synchronous tumours, and a ≥ 2-year time interval between cancers was indicative of metachronous tumours. The majority of tumours included in this study were histologically epidermoid (31 of 50 patients). 14
A single institution’s 28-year experience with MPLC was reported by Antakli et al. 18 Following a total of 1572 curative resections, 54 patients (3.4%) were found to have 65 second primary lesions, of which 39 (60%) were metachronous and 26 (40%) were synchronous. 18 Second primary tumours occurred between 5 and 218 months after initial curative resection. Interestingly, the time between second and third primary tumours was much shorter, at between 5.5 and 51 months. 18 The majority (50.7%) of second primary tumours were of similar histological type to the first primary tumour. There was no evidence to indicate that minimal resection of the first tumour had a causative role in the development of the second tumour. It was established that MPLC occurs in a proportion of long-term survivors who have undergone curative resections. Since most lung cancer deaths occur within 2–3 years of resection, a large proportion of patients at risk of developing MPLC were eliminated in this study. 18
Patients with NSCLC diagnosed between 1990 and 1999 were evaluated for MPLC from medical history or during follow-up. 24 Approximately 25% of the patients had second or further primary tumours during the follow-up period. The time interval between the first and second primary tumours was significantly shorter for patients with NSCLC as both the first and second tumour types. Of these patients, 80% were diagnosed in the first year, indicating for the first time that differences in tumour growth characteristics between patients with and without MPLC may be a potential prognostic marker. 24
A study evaluating the surgical outcomes of 908 patients with NSCLC determined that 57 (6.3%) developed a second primary lung cancer, 25 but the 5-year survival rate of patients with metachronous MPLC (66%) was inconsistent with the literature, being substantially higher than previously reported rates. The 5-year survival was slightly higher for the synchronous cohort (70.3%) than for the metachronous cohort. This was the first study to determine that there were no pathophysiological differences between synchronous and metachronous MPLC, since the classification is based entirely on the timing of diagnosis and not the actual development process. Since 57% of synchronous cancers were detected during preoperative radiography and another 39% at the time of surgery, 25 the authors reported that synchronous tumours should be carefully evaluated before and during surgical resection in order to avoid recurrence. They added that precise staging and an aggressive surgical approach for early stages (together with oncologically sound parenchymal sparing procedures) should be adapted as standard clinical practice, to increase long-term survival in patients with MPLC. 25
A large institutional study (892 patients) evaluating the development of MPLC after primary surgical resection was reported in 2002. 26 Second primary tumours developed in 51 patients (5.7%). The cumulative probability of a cancer-free interval for metachronous tumours was 29% at 3 years, 15% at 5 years, and 2% at 10 years. This study was limited by the fact that it was not possible to perform a similar analysis with the synchronous MPLC cases, however. It was concluded that patients with metachronous MPLC had a worse prognosis than those with synchronous tumours. In addition, the study also found that aggressive assessment and surgical intervention was an efficacious management approach that raised no safety issues in these patients. The authors recommended a long-term follow-up policy at 6-month intervals for ≥ 3–5 years, to improve early detection of the second malignancy. 26
A study published in 2004, reporting data collected over the preceding 30 years, performed outcome measures for postsurgical interventions in bilateral MPLC. 27 Of the 1906 patients undergoing surgical resection in this study, 1.9% developed bilateral primary lung cancer, was is in accordance with rates observed by others.14,27,32 Analysis of synchronous tumours did not reveal any predominant histological subtype, and the second primary tumour was histologically different from the first in only six of 18 patients with metachronous MPLC. The authors concluded that surgical therapy of bilateral MPLC was technically different from that of ipsilateral cases. 27 It should be noted that cases of ipsilateral MPLC are more technically challenging than bilateral MPLC, due to the lung adhesions commonly observed in the ipsilateral form. 25 Overall, aggressive surgical management was recommended, with sparing procedures (such as sleeve resection and limited resection) carefully considered, since maintaining respiratory function is a key factor influencing health-related quality-of-life. 27 An aggressive surgical approach was also recommended by others.16,28
A molecular and clinicopathological analysis of patients with apparent MPLC has been performed. 12 Comparative genomic hybridization array was performed on all tumours in this study, to determine whether the second lesion was an independent occurrence or a metastasis. 12 Genomic profiling was found to contradict the clinicopathological diagnosis in 18% of the tumours. The use of clinicopathological criteria in conjunction with genetic profiling was therefore highly recommended for differentiating between independent and clonal tumours. 12 A follow-up study by the same group aimed to determine the existence of clonal relationships between MPLCs by evaluating EGFR and Kras mutation status. 29 When Martini and Melamed criteria were used, six of seven patients were found to have multiple primary adenocarcinomas and one had metastatic carcinoma. American College of Chest Physicians criteria 32 suggested that only three of the six cases were primary tumours, and the seventh was undetermined.14,32 It was proposed that EGFR/Kras mutational profiling improved discrimination between MPLC and intrapulmonary metastases, comprehensively highlighting the inherent limitations of current clinical guidelines. A further study of comparative mutational profiling revealed that, when standard pathological examination was inconclusive, comparative mutational profiling was capable of differentiating between metastatic tumours and second primary lesions. 30
The importance of the sum value of immunohistochemical differences in p53, p16, p27, and c-erbB2 was assessed in 50 patients with MPLC, 20 patients with intrapulmonary metastasis and 30 reference cases with lymph node metastasis. 31 The lymph node metastatic samples were used as a reference point to calculate the sum values of the MPLC tissue specimens. The sum value did not exceed 90 in any lymph node metastatic tissue sample, therefore this value was used as the cut-off for MPLC diagnosis. In the experimental set of 50 MPLC tissues, 41 (82%) showed a sum value > 90. In comparison, four (20%) patients diagnosed with intrapulmonary metastasis showed a sum value > 90, indicating a low false-negative rate. These findings suggest that these protein markers may be a robust adjunct to the clinicopathological diagnosis and staging of MPLC. Our retrospective study of 10 patients with synchronous MPLC found correlations between squamous cell carcinoma and expression of carcinoembryonic antigen, neuron specific enolase and cytokeratin fragment 21-1 in 20% of cases. 19 It is therefore of paramount importance to identify correctly the molecular markers that are additive to the clinicopathological diagnosis and staging of MPLC.
Discussion
This literature review underscores the necessity for further studies to aid the differentiation between MPLC and metastasis. It is important to note that cancer recurrence represents treatment failure, whereas the development of new primary tumours is suggestive of persistent exposure to aetiological risk factors. The incidence of MPLC is likely to increase in the future,29,30 and studies leading to formal recommendations and guidelines for diagnosis and management of this condition are urgently required.
The cost of gene sequencing has decreased with the advent of whole genome and deep sequencing techniques. This technology will allow us to ask iterative questions regarding the fundamental differences between synchronous/metachronous MPLC and the first primary lung lesion or lung metastasis. Such studies will also help in understanding the selective advantage of exclusive (or combined) use of molecular biology or clinicopathological characteristics to diagnose and predict prognosis in these patients. Multicentre-based health-related quality-of-life assessment is also imperative, given the ever-increasing 5-year survival rate.
A potential limitation of the current systematic review was that it was not presented according to the recommendations of the Cochrane Database of Systematic Reviews, or the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. However, the search methodology and the subsequent analyses of the collected literature was done in much the same comprehensive way as the aforementioned recommendations.
Although MPLC is classified into synchronous and metachronous types, both may have the same pathophysiology. A steadily growing hypothesis, known as field cancerization, suggests that carcinogenic exposure or genetic factors affect tissues or organs, 33 potentiating many cells in the same area to become transformed. It is also thought that these different clonal populations accumulate independent genetic alterations. 34 Research has shown that multicentric involvement could result from a single clone of mutated cells, which spreads and implants. 34 Further research is therefore needed to understand more clearly the differences, if any, between synchronous and metachronous MPLC.
Footnotes
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.