
Abstract
Background:
Although hemophilia A mainly affects males, carriers (defined as females with hemophilia A, as well as symptomatic or asymptomatic hemophilia A carriers) are at risk of excessive bleeding, particularly during trauma or during surgical procedures. Clinical trials have focused on male patients with severe disease, and data for females are limited. Improved, evidence-based treatment guidelines for management of hemophilia A carriers are required.
Objectives and design:
The NuDIMENSION study is a phase IV, prospective, open-label, single-arm study that will evaluate the perioperative efficacy and safety of simoctocog alfa (Nuwiq®), a recombinant factor VIII (FVIII), in women/girls with hemophilia A undergoing major surgery. The study will be conducted at approximately 15 centers worldwide. Women/girls aged ⩾12 years, with mild or moderate hemophilia A (residual FVIII activity (FVIII:C) ⩾1% to <40%) and with no current/past FVIII inhibitors are eligible. All patients must be scheduled to undergo a major surgical procedure during which simoctocog alfa will be administered.
Methods and analysis:
The primary endpoint is overall perioperative hemostatic efficacy (“success” or “failure”) of simoctocog alfa. Hemostatic efficacy will be assessed at the end of surgery and at the end of the postoperative period (i.e., completion of wound healing), with overall adjudication by an Independent Data Monitoring Committee. Safety endpoints will include the incidences of thrombotic events and FVIII inhibitor development. The aim is to recruit 28 patients to achieve 26 evaluable surgeries.
Ethics:
Ethical approval will be received from institutional review boards/independent ethics committees, and the study will be conducted in compliance with the Declaration of Helsinki.
Discussion:
Data from NuDIMENSION will generate much-needed evidence on surgical management of women/girls with hemophilia A, which will help to enable the development of treatment guidelines specific for such patients.
Trial Registration:
CT EU 2022-502061-17-00; NCT05936580
Plain language summary
Hemophilia A is an inherited bleeding disorder caused by an abnormality in the F8 gene that leads to a reduction in clotting factor VIII (FVIII). Females who inherit the abnormal gene can pass on the gene to their children and are known as ‘carriers’. Some carriers have FVIII levels below 40% of normal levels and are classified as having hemophilia A. However, excessive bleeding can also occur in females with FVIII levels greater than 40% of normal. Excessive bleeding may only be evident after injury, during surgery or during childbirth, but can also cause heavy periods, for example.
Replacement therapy with FVIII can be used to treat or prevent bleeds in people with hemophilia A. During surgery higher levels of FVIII may be needed to prevent excessive bleeding. However, information on the use of FVIII comes predominantly from trials in male patients with severe disease. Information on the treatment of carriers is limited, and treatment guidelines for surgical management of carriers are lacking.
Simoctocog alfa (Nuwiq®), a FVIII therapy, is effective at preventing and treating bleeds, including during surgery, in males with severe hemophilia A. NuDIMENSION is a multicenter, international study that will evaluate simoctocog alfa in women and girls with hemophilia A who need major surgery.
The study will include women/girls aged 12 years or older who have mild or moderate hemophilia A and who are planned to have a major surgery. The primary endpoint is overall hemostatic efficacy (“success” or “failure”), that is, how well bleeding is prevented/controlled. This will be assessed at the end of the surgery and at the end of the postoperative period. Up to 28 women and girls will take part in the study. Data from NuDIMENSION will provide important information to help decide how best to treat women/girls with hemophilia A who need surgery.

Introduction
The X-linked recessive inheritance pattern of hemophilia A has historically led to the misconception that females who have a pathogenic variant of the F8 gene 1 (“carriers”) are asymptomatic. 2 However, it is now increasingly recognized that incomplete hemostasis in hemophilia A, which arises due to deficient clotting factor VIII (FVIII), not only occurs in males but can also occur in carriers.2,3
Carriers often experience excessive bleeding associated with menstruation, childbirth, and the postpartum period,1 –4 or following trauma or surgery. 1 Bleeding in carriers negatively impacts their quality of life.2,4 –6 The need for additional hemostatic coverage in carriers is recognized by the World Federation of Hemophilia (WFH) who recommend that carriers with low factor levels are treated and managed the same as males with hemophilia. 1 While guidance exists for overall principles of care for hemophilia carriers, 4 there are few guidance documents which detail their specific management.1,7 Standardized approaches for the management of hemophilia A carriers, informed by clinical trial data, remain lacking.
Hemophilia A severity is classified according to FVIII levels 1 and approximately 30% of carriers have levels <40 IU/dL, 8 thus fulfilling the WFH FVIII level threshold for the disease. 1 Bleed severity in carriers is however poorly correlated with FVIII levels3,9 and even carriers with FVIII levels >40 IU/dL can experience excessive bleeding2,5,10 that may require hemostatic treatments. 11 A nomenclature developed by the International Society on Thrombosis and Haemostasis (ISTH) to improve diagnosis and management of hemophilia A in women/girls acknowledges this, distinguishing five clinically relevant categories of carriers: women/girls with mild, moderate or severe hemophilia A (FVIII >5 and <40 IU/dL, 1–5 IU/dL, and <1 IU/dL, respectively), and symptomatic and asymptomatic hemophilia carriers (FVIII ⩾40 IU/dL with and without a bleeding phenotype, respectively). 2
The majority of women/girls with hemophilia A (FVIII <40 IU/dL) are classified as having mild disease (FVIII: >5 and <40 IU/dL)8,12 and are generally treated on demand in response to trauma or during surgery. 1 Treatment options for women/girls with hemophilia A include antifibrinolytics (e.g., tranexamic acid), hormonal therapies (to manage heavy menstrual bleeding), desmopressin, and FVIII concentrates.1,11 FVIII concentrates may be needed when higher FVIII levels are required for a prolonged period, for example, prior to major surgery and in the postoperative period (POP). 1 Data supporting efficacy of therapies for hemophilia A however predominantly come from male patients with severe disease with a sparsity of data available from patients with mild disease11,13 and for women/girls.2,11
Simoctocog alfa (Nuwiq®, human-cl rhFVIII; Octapharma AG, Switzerland) is a fourth-generation recombinant FVIII concentrate produced in a human cell line 14 and is indicated for the treatment and prophylaxis of bleeding in patients with hemophilia A of any age. 15 Efficacy and safety of simoctocog alfa in the prevention and treatment of bleeding, as well as in surgical prophylaxis, have been demonstrated in clinical trials of male patients with severe hemophilia A.14 –16
The
Methods and analysis
Design
NuDIMENSION is a phase IV, prospective, open-label, single-arm, multicenter study (registration numbers: CT EU 2022-502061-17-00; NCT05936580). The study was initiated at the first study sites in Q4 2023, and patients will be enrolled at approximately 15 sites in 7 countries (France, Finland, Germany, Italy, Serbia, Spain, and the United Kingdom). Professor Johannes Oldenburg (University Clinic Bonn, Germany) is the coordinating investigator for the study. A maximum of 28 female patients with mild or moderate hemophilia A will be enrolled in order to document 26 evaluable major surgeries. All patients will be scheduled to undergo a major surgical procedure during which simoctocog alfa will be administered and each patient can have only one surgery during the study. For each patient, the study will start from the time of the screening visit until the final visit which is defined as 30 ± 3 days after the day of the surgical procedure or on the day of discharge (whichever comes later). There should be a minimum of 6 consecutive POP visits or POP observation days. The end of the study is defined as the last visit of the last patient participating in the study.
Simoctocog alfa will be administered intravenously once within 3 h prior to surgery and in accordance with the prescribing information.15,17 Pre- and postoperative FVIII plasma levels are to be maintained between 80 and 100 international units (IU)/dL. Treatment will be repeated as necessary every 8–24 h until adequate wound healing. Simoctocog alfa dosing will continue for at least another 7 days, if required, to maintain FVIII plasma levels of 30–60 IU/dL (Figure 1). Concomitant therapies not interfering with the objectives of the study, and other concomitant medications (including thromboprophylactic medications), are permitted during the study. No FVIII concentrates other than simoctocog alfa will be administered (except for emergency situations). If patients switch permanently to another FVIII product, they will be assessed as treatment failures in the efficacy analyses.

NuDIMENSION study design.
Patients may withdraw from the study at any time for any reason, without any resulting detriment and without the need to justify their decision. Patients may also be withdrawn at the investigator’s discretion for safety, compliance, or other reasons.
An Independent Data Monitoring Committee (IDMC) has been established for the study by the sponsor and will provide independent advice to the sponsor. The IDMC is composed of three recognized experts in the field of hematology who are not actively recruiting patients (Roger J. Lewis (Harbor-UCLA Medical Center, USA)—Chair, Craig M. Kessler (Lombardi Cancer Center, USA), Robert Klamroth (Vivantes Klinikum im Friedrichshain, Germany)), and a biostatistician (Volker Schoder (Metronomia Clinical Research GmbH, Germany)). The IDMC will adjudicate the overall hemostatic efficacy assessment of the perioperative prophylaxis with simoctocog alfa and will review and monitor adverse event(s) (AEs) during the study. They will also provide guidance on: the protection of participants during the study; the proper conduct and interpretation of the efficacy and safety data during the study and at the end of the study; and the ongoing scientific validity, integrity, and clinical and scientific relevance of the study. The IDMC will review relevant data periodically during the study and will give advice on the continuation, modification, or termination of the study. The IDMC will report to the sponsor, and its members are free from conflicts of interest with respect to the clinical study, the principal and co-investigators, and the sponsor.
Objectives and endpoints
The objectives of the NuDIMENSION study are summarized in Box 1.
NuDIMENSION study objectives.

FVIII, factor VIII; WFH, World Federation of Hemophilia.
The primary endpoint is the overall perioperative hemostatic efficacy (“success” or “failure”) of simoctocog alfa in women/girls with mild or moderate hemophilia A undergoing major surgery. Hemostatic efficacy will be assessed at the end of surgery (last suture) by the surgeon and at the end of the POP by the investigator (hematologist), both using a four-point ordinal hemostatic efficacy scale (Table 1). The end of the POP will be defined as completion of wound healing (e.g. removal of sutures, cessation of drainage etc.) as defined by the investigator. Overall, hemostatic efficacy will be adjudicated by the IDMC using a predefined algorithm that considers the surgeon’s assessment of intraoperative hemostatic efficacy and the investigator’s assessment of postoperative hemostatic efficacy to classify the overall hemostatic efficacy as success or failure (Table 2).
Four-point ordinal hemostatic efficacy scale.
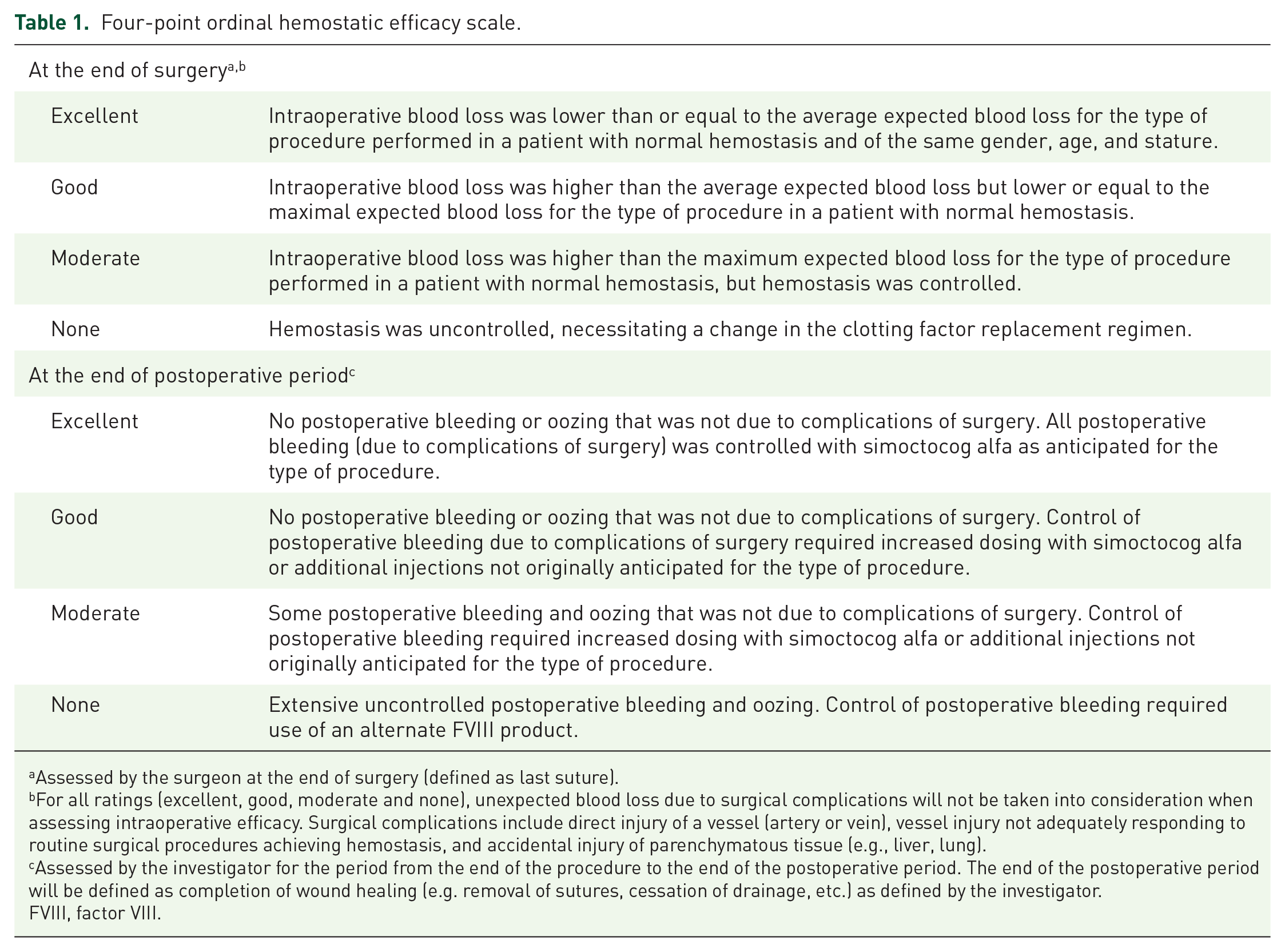
Assessed by the surgeon at the end of surgery (defined as last suture).
For all ratings (excellent, good, moderate and none), unexpected blood loss due to surgical complications will not be taken into consideration when assessing intraoperative efficacy. Surgical complications include direct injury of a vessel (artery or vein), vessel injury not adequately responding to routine surgical procedures achieving hemostasis, and accidental injury of parenchymatous tissue (e.g., liver, lung).
Assessed by the investigator for the period from the end of the procedure to the end of the postoperative period. The end of the postoperative period will be defined as completion of wound healing (e.g. removal of sutures, cessation of drainage, etc.) as defined by the investigator.
FVIII, factor VIII.
Overall assessment (success or failure) derived from assessment of intra- and postoperative hemostatic efficacy.
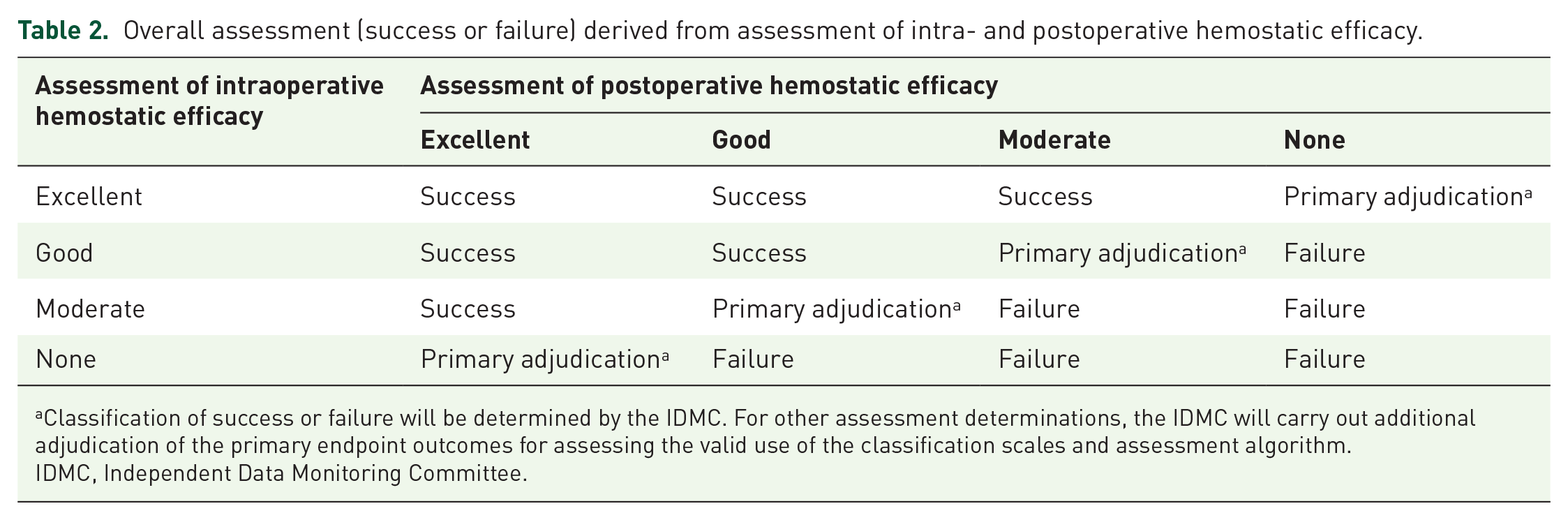
Classification of success or failure will be determined by the IDMC. For other assessment determinations, the IDMC will carry out additional adjudication of the primary endpoint outcomes for assessing the valid use of the classification scales and assessment algorithm.
IDMC, Independent Data Monitoring Committee.
Secondary endpoints of this study are: intra- and postoperative hemostatic efficacy of simoctocog alfa, both using a four-point ordinal hemostatic efficacy scale; number of perioperative allogeneic blood products (red blood cells, platelets and other blood products) transfused; perioperative FVIII plasma levels immediately before (⩽30 min) and after (15–30 min) simoctocog alfa injections; perioperative hemostatic efficacy of simoctocog alfa assessed using the four-point scale recommended by the WFH 1 ; incidence of AEs; incidence of thrombotic events; and incidence of FVIII inhibitor formation.
Patient eligibility and recruitment
Women/girls ⩾12 years of age with mild or moderate hemophilia A (residual FVIII activity (FVIII:C) ⩾1% to <40%) scheduled to undergo major elective surgery, and with no current or past FVIII inhibitors will be eligible for the study. Patients must meet all inclusion criteria and none of the exclusion criteria. For full patient eligibility criteria see Table 3.
Patient eligibility criteria.

Surgeries are defined as major if any of the following criteria are met: requiring general or spinal anesthesia; requiring opening into the great body cavities; orthopedic interventions involving joints (ankle, knee, hip, wrist, elbow, shoulder); surgeries/conditions in which the patient’s life is at stake.
ALT, alanine aminotransferase; AST, aspartate aminotransferase; BU, Bethesda units; FVIII, factor VIII; FVIII:C, factor VIII activity.
Data collection and analysis
Data will be recorded for each patient via an electronic case report form. Demographic and baseline characteristics (gender, age, ethnic origin, blood group, height, weight, body mass index) will be recorded at the screening visit, along with the patient’s medical and prior treatment history which will be obtained by interviewing the patient and/or obtaining medical records. Blood samples will be drawn for F8 genotype analysis preferably at the screening visit, or alternatively at any time during the study.
Blood sampling will be performed for the following assessments at various times during the study at central and/or local laboratories: FVIII inhibitors, FVIII plasma levels (chromogenic and one-stage assays), and routine chemistry and hematology. A negative result for inhibitors (<0.6 BU/mL) must be confirmed at the screening visit. F8 genotype will be determined once during the study at a central laboratory.
Safety
Perioperative safety of simoctocog alfa will be assessed by monitoring for AEs and treatment-related AEs. These include thrombotic events, FVIII inhibitor formation, and other AEs or serious adverse events temporally associated with the injection of simoctocog alfa. All suspected treatment-related AEs and other safety information (any drug overdose, interaction, medication error or lack of efficacy) will be documented and reported. Any unexpected treatment-related AEs will be reported to the Independent Ethics Committees (IECs)/Institutional Review Boards (IRBs). Vital signs will be monitored, and routine chemistry and hematology performed at various times during the study. As pregnancy is an exclusion criterion for the study (Table 3), pregnancy tests will be conducted in patients of child-bearing potential at the screening visit and their pregnancy status checked again at the preoperative stage.
Statistical methods
The primary aim of the study is to prove that overall perioperative hemostatic efficacy is achieved with simoctocog alfa (defined as an overall efficacy rating of “success” by the IDMC) with a probability of >60% in major surgeries. Assuming a true success rate of 85% and employing a one-sided binomial test at a one-sided significance level of 2.5%, a total sample size of 26 surgeries was calculated to be needed to achieve a statistical power of >80%.
For primary statistical analysis, an exact one-sided binomial test will be employed, and a two-sided exact 95% confidence interval will be given. A similar analysis will be performed for assessments of intraoperative hemostatic efficacy, postoperative hemostatic efficacy, and overall hemostatic efficacy (surgeon and investigator combined (IDMC adjudicated)). In addition, secondary efficacy and safety endpoints will be analyzed descriptively.
Ethics
NuDIMENSION will be conducted in accordance with ethical principles of international guidelines including the Declaration of Helsinki and the International Council for Harmonisation (ICH) Guideline for Good Clinical Practice (GCP) and applicable regulatory requirements. The study protocol (and amended protocols, if necessary), and a sample of patient information and informed consent form, and other relevant documents will be submitted to the IECs/IRBs and regulatory authorities. Any amended protocols will require IRB/IEC approval before implementation. The investigator will obtain freely given written consent for each patient or the patient’s parent(s)/legal representative(s).
The results are planned to be published in a peer-reviewed journal and presented at scientific meetings. The sponsor and investigators will ensure patient confidentiality is preserved through appropriate technical and organizational measures.
Discussion
Clinical trials in hemophila A have to date mostly focused on male patients with severe disease (FVIII <1 IU/dL 1 ), with female patients usually ineligible for inclusion. 11 However, despite females being more often classified as having milder disease compared to males,8,12,18 the negative impact of the disease on quality-of-life in females is evident across the range of disease severities.6,11 Evidence-based specific treatment guidelines for hemophilia A carriers are therefore much needed, including recommendations for perioperative hemostasis in females with mild or moderate disease.
Carriers undergoing surgical procedures can experience increased bleeding1,10 and for mild hemophilia patients, occurrence of trauma or surgery may be the first time that this abnormal/excessive bleeding manifests. 1 The WFH guidelines for the management of hemophilia state that hemophilia A patients undergoing surgery require additional hemostatic coverage. 1 However, extrapolating current standard of care for surgery from male hemophilia A patients to females is complicated by the lack of correlation between FVIII levels and bleeding severity in carriers.3,9
Although desmopressin is indicated as a hemostatic treatment during surgery in patients with mild hemophilia A who show a good response to the drug presurgery, due to tachyphylaxis it is recognized to not be suitable for major surgery where adequate hemostasis is required for a longer period. 1 In these situations, FVIII concentrates are the preferred hemostatic treatment with a treatment duration of at least 7–10 days. 1 FVIII replacement therapy is a well-established approach for the management of patients with severe hemophilia A, for prevention and treatment of bleeding episodes as well as surgical prophylaxis. 1 However, clinical data on its efficacy and safety in patients with mild/moderate disease and in women/girls with hemophilia A, including during surgery, are limited. In a retrospective chart review of 47 women/girls with hemophilia, of the 15 hemophilia A carriers who underwent major surgery (n = 10), minor surgery (n = 3), or a major dental procedure (n = 2), the majority of patients received FVIII concentrates (n = 12 (80%)). 19 Other hemostatic treatments were desmopressin (n = 3 (20%)) and antifibrinolytic (n = 1 (6.7%)). Bleeding control was deemed sufficient (where bleeding level was as normally expected for the procedure) in 13 (86.7%) cases. 19
The efficacy and safety of simoctocog alfa in the prevention and treatment of bleeding, and as surgical prophylaxis, have been extensively demonstrated in clinical trials in male patients with severe hemophilia A.14 –16 In a pooled analysis of seven clinical trials with simoctocog alfa in previously treated male patients, hemostatic efficacy was rated as excellent or good by the surgeon and the hematologist for 24 of 25 major surgeries and as moderate for one surgery. 16 There were no serious treatment-related AEs, and none of the patients developed FVIII inhibitors. 16 The NuDIMENSION study will provide female-specific data by examining the hemostatic efficacy and safety of perioperative FVIII replacement with simoctocog alfa in women/girls diagnosed with mild or moderate hemophilia A undergoing major elective surgery. Women/girls with severe hemophilia A (FVIII:C <1%) will not be eligible for the study. By including patients with mild and moderate hemophilia A, the study aims to create a more homogenous population with respect to prior treatment history and reduce the risk of confounding factors on the interpretation of the results. This will allow the focus to be on females with nonsevere disease who are not sufficiently covered in the treatment guidelines at present.
Conclusion
Despite increasing awareness of the issues faced by carriers of hemophilia A, prospective clinical trial data are lacking. Data from the NuDIMENSION study will contribute to the evidence needed to inform specific treatment guidelines for surgical management of women/girls with mild or moderate hemophilia A.
Footnotes
Acknowledgements
Medical writing assistance was provided by Kat Karolemeas, nspm ltd., Meggen, Switzerland, and funded by Octapharma AG. Submission of the manuscript was undertaken by Kat Karolemeas, Medical Writer from nspm ltd., with prior authorization from the listed authors and their confirmation of all statements and declarations.
Declarations
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.