
Abstract
Introduction:
In early 2021, the European Collaborative Haemophilia Network (ECHN) conducted a survey to determine whether the paradigms of care across the European region have changed with the introduction of novel therapies for people with hemophilia.
Methods:
We conducted a survey in 19 ECHN centers from 17 countries in the European region. The aim was to track recent changes in the hemophilia treatment landscape, determine the impact of these changes on hemophilia treatment centers and comprehensive care centers in the region, and to look into the future of care as applied to people with hemophilia. The survey was structured to include three key areas: demographics and organization; current challenges and opportunities; and future directions.
Discussion:
Our survey provides a snapshot of the current approach to hemophilia treatment that highlights a move toward preventive, rather than reactive care, but that also raises a number of key concerns related to costs and accessibility (particularly as related to novel therapies), time limitations for clinical research, and ongoing issues regarding human resources (particularly in terms of new doctors entering the field) and availability of laboratory resources as the use of novel therapies (some with unique modes of action and unusual adverse events, some with specialized monitoring requirements) becomes commonplace.
Conclusion:
While our survey suggests that specialized care will continue to play a central role in the management of hemophilia, the standards and protocols, as well as the centers themselves, will have to continue to evolve if they are to continue to provide the highest level of care. To meet this requirement, there is a clear need for engaging, ongoing education programs for healthcare professionals working in the field of hemophilia that can be adjusted to the changing landscape of hemophilia therapy and monitoring.
Keywords
Introduction
In early 2021, the European Collaborative Haemophilia Network (ECHN) conducted a survey to determine whether the paradigms of care across the European region have changed with the introduction of innovative therapies for people with hemophilia with and without inhibitors.1–3 The aim was to track recent changes in the hemophilia treatment landscape, determine the impact of these changes on hemophilia treatment centers (HTCs) and comprehensive care centers (CCCs) in the European region, and to anticipate future changes in our approach to hemophilia therapy with the advent of further novel treatment options such as antitissue factor pathway inhibitors, small interfering RNA therapeutics targeting antithrombin, and gene therapy.4–7 The implementation of these innovative approaches will necessitate further changes in treatment practices in the form of new laboratory tests, monitoring for new adverse events, and new strategies regarding the role of immune tolerance induction (ITI).
Methods
We conducted a survey in 19 ECHN centers from 17 countries in the European region (Figure 1). Centers were selected by the ECHN steering committee on the basis of their being national coordinating centers, and as such can be considered representative of the general approach of larger, more specialized centers in each country. ECHN centers can also be considered representative of each country in terms of the availability of products, access to treatment, involvement in coordination of care and/or research and innovation at the national level. Surveys were sent by email to all ECHN members; each recipient was responsible for completion of the survey based on data from hemophilia treatment centers in their respective country, with data-collection assistance provided by centers as required. The study was conducted without industry influence or involvement. Our study did not require an ethical board approval because any data on patient populations was requested from the survey respondents in aggregated form only.

Countries included in the ECHN survey 2021.
Survey reporting was conducted in accordance with SQUIRE 2.0 guidelines for consensus reporting. 8 In the survey, the terms nonfactor replacement therapy (NFRT) referred to emicizumab and nonreplacement therapy (NRT) referred to anti-tissue factor pathway inhibitor (TFPI) antibodies and fitusiran. The results were analyzed by the working group developing this manuscript. Surveys were completed in early 2021; meetings were held to collate survey data for the purpose of analysis. The complete survey is included as Supplemental Appendix 1.
The survey was structured to include three key areas:
Demographics and organization, including number of patients, center location and accreditation status, funding, staffing, and collaboration.
Current challenges and opportunities as they relate to assessment tools utilized [including pharmacokinetic (PK) measures for personalization of treatment], laboratory practice, hemostatic agent procurement, involvement in clinical trials, protocols/procedures, and database practices.
Future directions, which focused on resourcing, and the perceived ability for innovation as we move toward new protocols and treatment practices.
For the purpose of analysis, we have combined ‘Current challenges and opportunities’ and ‘Future directions’ into a single section herein.
Results and discussion
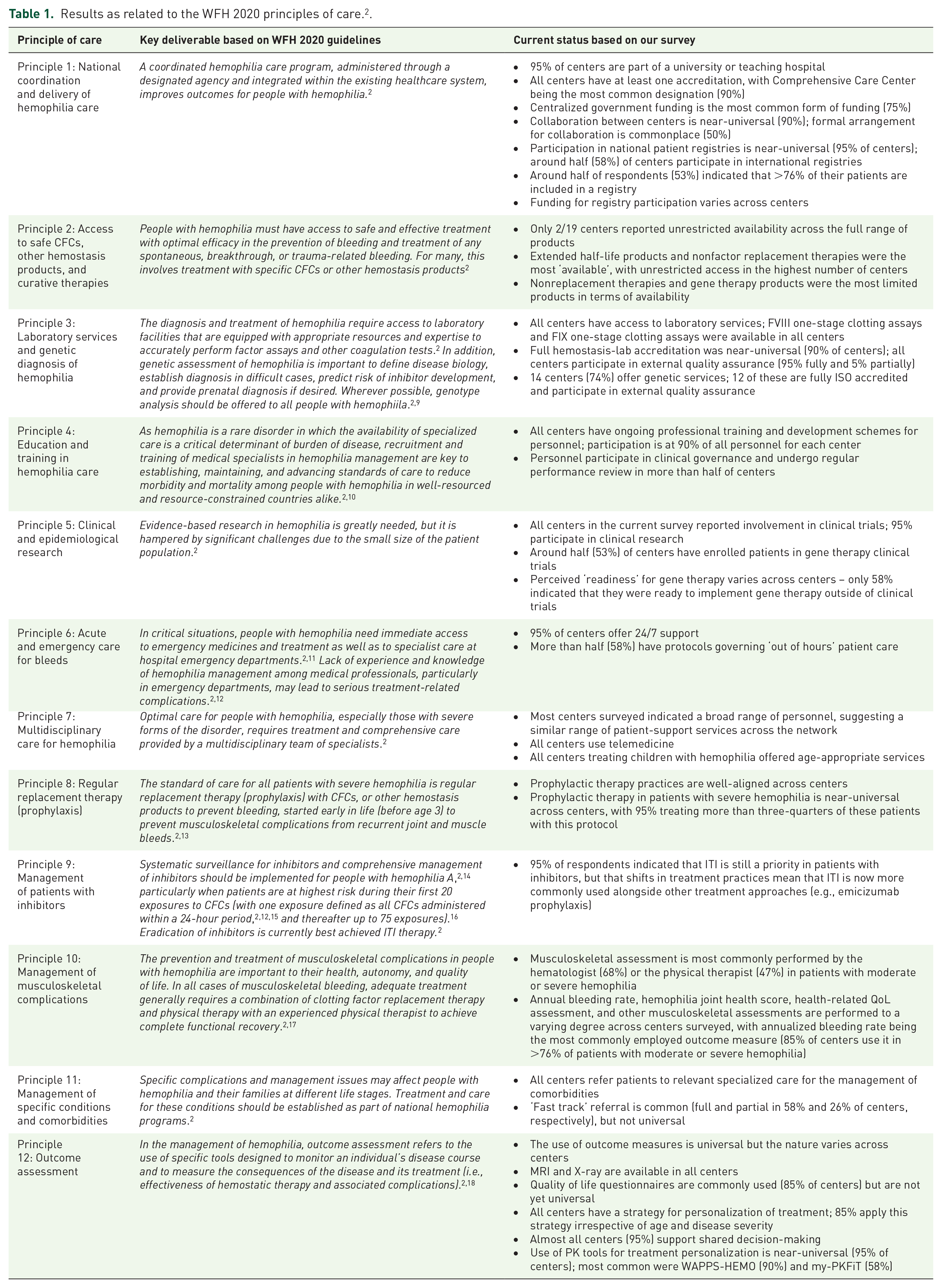
The key findings of the current survey as they relate to the recent principles of care as issued by the World Federation of Hemophilia (WFH) 2 are outlined in Table 1. The results from the full survey are included as Supplemental Appendix 2.
Results as related to the WFH 2020 principles of care. 2 .
Demographics and organization
Patient demographics
The current survey represents the treatment experience of 19 respondents from centers treating a total of 4710 people with hemophilia A (1792 patients with mild, 655 with moderate, and 2263 with severe disease), 1067 people with hemophilia B (417 patients with mild, 217 with moderate, and 433 with severe disease), and 1569 hemophilia carriers. Patients were categorized for hemophilia severity or carrier status according to the most recent WFH guidelines. 2 Most centers [13 of the 19 surveyed (68%)] treated both adults and children; 4 centers (21%) treated adults only and 2 centers (11%) treated children only. The most common age group being treated across both hemophilia A and B and across all disease severities was age 19–60 years.
Organization and funding
The vast majority (95%) of centers surveyed were part of a university or teaching hospital; all centers had at least one accreditation, the most common being that of comprehensive care center (90% of centers). Centralized government funding was the most common form of funding (74%); local government and insurance-company funding was reported by 42% and 32% of centers, respectively.
Current challenges and opportunities and future directions
Current network of hemophilia treatment centers and involvement in patient registries
While collaboration between centers is near-universal in our survey (90% of centers surveyed indicated being involved in some form of collaboration with other specialized centers), the specific nature of this collaboration differs across the network of centers – collaboration in the form of shared treatment protocols/guidelines, for example, was indicated by ~65% of centers, while liaison between centers concerning patient referral and general shared patient care were reported by around half of all centers surveyed.
Collaboration in the form of registry participation is also near-universal in our survey, with 18 of the 19 centers participating in national and 11 in international registries. While this appears positive, and numbers suggest increased engagement when compared with earlier surveys (which indicate that only around half of centers (57%) participated in a central patient registry in 2012),18,19 this remains an area in which caution must be exercised when interpreting results and making inferences: several respondents indicated involvement in multiple patient registries, which highlights possible concerns regarding standardization of data reporting, and a possible need for alignment across national and international registries to ensure that data collected offers a robust overview of the state of treatment and adherence to principles of care.
So, while involvement in registries is undeniably a key element of hemophilia care, there are risks associated with ‘over involvement’. If we have too many registries, is it the same as having none at all? Future success is likely to come in the form of standardization of protocols and procedures. This is of particular relevance in a rare condition such as hemophilia, which benefits from interchangeability of data and standardized protocols. Further research is warranted in this area to determine whether regional challenges or regulations are leading national centers to take different approaches to data collection.
An encouraging finding of this survey is that collaboration between centers (either direct collaboration or through patient registries) is commonplace, with all centers surveyed indicating a level of involvement with other centers in their region. In addition, almost half of the centers surveyed indicated a level of shared patient care and almost 65% have an official system in place for the implementation of shared protocols and guidelines. This is encouraging and could help to circumvent any regional political involvement that influences at the national level.
However, despite almost all being involved in a network, more than one-third of centers (37%) report an optimal network of centers in their country as an ongoing concern, with a higher number still (58%) indicating that availability of online patient-data registries remained a concern (Figure 2) – this most likely reflects concern related to time required for involvement, adequate resources, and general access, but this conclusion is not explicitly supported by our data.

What resources are currently lacking in your center?
Access to and availability of therapies
Availability of treatment options varies across countries and centers and, in the case of products that are not yet licensed, is limited to use in a clinical trial setting. Extended half-life products and NFRTs were the most ‘available’, with unrestricted access in the highest number of centers (14/19 and 12/19 centers, respectively). Nonfactor replacement therapies and extended half-life products were most commonly available free of charge, either as a standard therapy or as part of a clinical trial. A breakdown of availability of specific products and reimbursement status by country as reported by the survey respondents is presented in Table 2.
Availability of products by licensing and reimbursement status across centers surveyed.
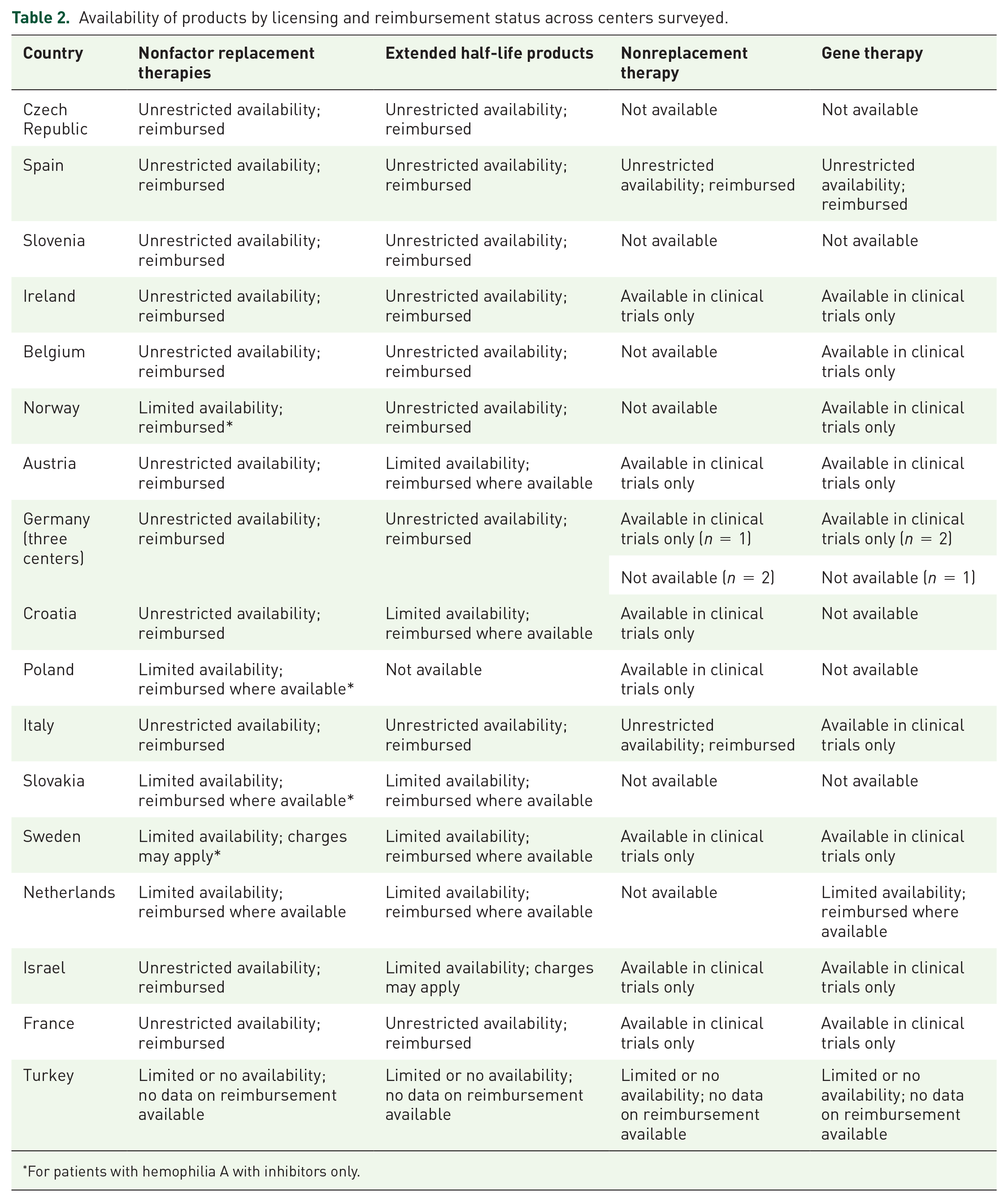
For patients with hemophilia A with inhibitors only.
Despite including only centers in higher resource countries, with the majority (74%) being funded at the centralized government level and supplementing care with external support (e.g. local funding, insurance company funding, and industry support), our survey clearly indicates that economic/cost considerations remain a very real part of hemophilia management. More than half of respondents (63%) indicated that costs impact access to NFRTs, and just under half (48%) indicated costs impact access to extended half-life therapies.
Despite the availability of novel products in many centers, concerns related to the increasing cost of therapies overall was near-universal among our respondents (95%; Figure 3). Around 85% of centers indicated that there is cooperation between patient associations and pharmaceutical companies in their country and around three-quarters (79%) of all centers surveyed indicated that patient organizations had some influence [either formal (58%) or informal (21%)] on access to treatment; 32% of respondents thought patient organizations had limited involvement in decisions related to the availability of specific products.
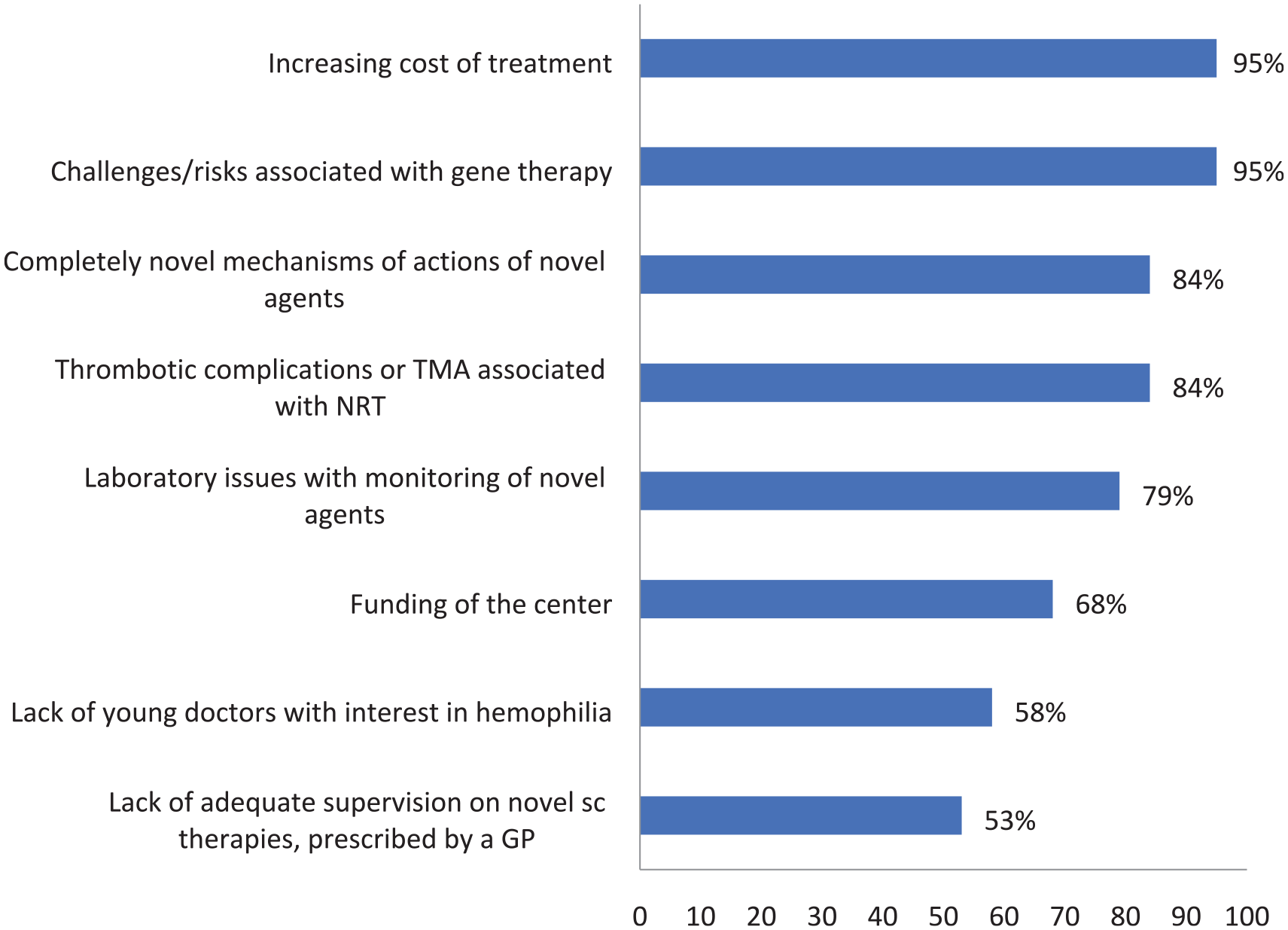
What challenges do you see with the innovations mentioned in this questionnaire?
Overall, the majority of centers (89%) indicated that resourcing solutions are currently in place that would allow access to all patients all available therapies, but a deeper dive into this data indicates that access is far from universal, with access/availability being limited by economic/cost considerations (Figure 2), regulatory conditions, and limitations related to clinical trial context and laboratory resources, as well as general resourcing as related to staff and training (Figure 3).
All centers surveyed use telemedicine (phone calls, email, etc.) if required in place of personal visits for people with hemophilia.
Laboratory services and genetic testing
At the diagnostic/monitoring level, our survey paints a favorable picture of the laboratory services available across the hemophilia centers surveyed – one that is supportive of an increasing reliance on novel therapies with sometimes unique monitoring requirements. Provision of genetic services was also high – almost three-quarters (74%) of centers have an integrated genetics lab; full ISO 15189 accreditation was near-universal (90%) across these centers, as was involvement in external quality assurance schemes (95% participated fully; 5% participated partially). This could be cautiously interpreted as representative of the perceived importance of integration of laboratory data and clinical phenotype, which could become increasingly important in the era of more detailed genetic sequencing.
Despite this positive impression of the laboratory side of hemophilia management, access to laboratory services remains a cause of concern for many of our respondents – 15 of the 19 centers surveyed (79%) indicated that issues related to monitoring of novel agents were likely to present a challenge as these protocols became more commonplace in the treatment of people with hemophilia (Figure 3).
Education and training
All centers indicated the availability of ongoing professional training and development programs for personnel, with almost 90% of respondents indicating that personnel engaged with these programs. Personnel participated in clinical governance in more than 60% of centers, and in more than half of the centers (53%) personnel underwent regular performance review. All centers indicated staff involvement in teaching activities, which is to be expected as the vast majority of centers surveyed (95%) are part of an accredited university or teaching hospital.
Although some countries have been successful in attracting trainees to specific research and training posts in hemostasis, once again, a deeper dive into the available data shows possible cause for concern – of the 19 centers surveyed, 11 indicated that they had general concerns regarding the number of young doctors entering the field of hemophilia management. Novel subcutaneous therapies that can be administered by Primary Care Physicians outside of the specialist centers were also highlighted as an area in which education and training was lacking, with more than half of respondents specifically indicating this as an area of concern (Figure 3).
Clinical trials and research
Clinical trial and research involvement has emerged as a key area of engagement across all the centers surveyed, with gene therapy presenting itself as an area of particular interest for almost 90% of our centers. Possible reasons for this high level of engagement include the fact that many of these trials are industry-driven, with the sponsor providing a level of support (both financial and regulatory) in navigating an environment with increasingly complex requirements relating to data, or that participation in clinical trials – especially of advanced therapeutics – translates into access when the treatment options become available outside of the trial setting.
Despite this high level of engagement, our survey suggests that gene therapy should still be considered a developing area of hemophilia treatment. Gene therapy represents a class of therapy that, due to being available exclusively in the context of clinical trials, has either limited or no availability in many of the centers surveyed; while just above half of all centers (53%) indicated that their center participated in clinical trials for gene therapy, available data indicates that the patient population was low (<10% of the total for the participating centers) in most cases.
Overall, a high majority (95%) of the centers surveyed expressed ongoing, general concerns related to the challenges surrounding gene therapy (Figure 3), and many of centers (>50%) indicated ongoing concern regarding their ‘readiness’ to implement gene therapy outside of clinical trials.
Survey data related to clinical trials and research in areas other than gene therapy followed a similar pattern, with around half of centers (52.6%) surveyed indicating that they had less than 10% of their patients enrolled in clinical trials for factor concentrates, and 68.5% indicating that they had less than 10% of their patients enrolled in clinical trials for NRTs. Just three centers indicated that they had more than 25% of their patient population enrolled in a clinical trial of any kind (two in factor concentrates, one in NRTs), and no center surveyed indicated having enrolled more than 50% of their patients in clinical trials of any kind.
In addition, more than half of respondents (13 of 19 centers surveyed; 68%) indicated that available time to dedicate to research was a concern, and a little more than half (10 centers; 53%) that the general infrastructure as related to clinical trials was generally lacking (Figure 2).
Acute and emergency care
Almost all centers (95%) offered 24/7 support from consultant hemophilia staff, and more than half of centers surveyed (58%) have protocols in place governing ‘out of hours’ patient review and care.
Multidisciplinary care for hemophilia
In our current survey, dedicated hemophilia personnel numbers vary across centers, with type of center (e.g. separate entity versus department of a greater hematology unit), accreditation status, and location within the surrounding care framework seeming not to influence personnel numbers. Most centers surveyed indicated a broad range of personnel (specialized nurses, pediatricians, physiotherapists, etc.) suggesting a similar range of patient-support services across the network.
In all 15 centers that reported treating children with hemophilia, age-appropriate services were available. These include services related to outcomes monitoring in pediatric patients using prophylaxis, and transitional arrangements for the transfer of adolescent to adult services in 12 of the 15 centers. A physiotherapist with age-appropriate training and a consultant pediatric hematologist was available in 11 of the 15 centers.
Despite this encouraging profile, more than half of our respondents (11 of 19 centers surveyed; 58%) indicated that adequate staffing was an area of concern (Figure 2), and that, as reported previously, there was specific concern regarding to the number of young doctors entering the field (Figure 3) and availability of staff to conduct clinical trials (Figure 2).
Prophylactic therapy for hemophilia
In terms of the provision of care that embraces preventive rather than reactive approaches, 95% of respondents indicated that > 76% of patients with severe hemophilia in their center are currently treated with prophylaxis. In addition, most of our respondents reported prescribing prophylactic treatment in <10% of their patients with mild hemophilia; in patients with moderate disease, an almost equal number of respondents indicated treating <10%, 11%–25%, 26%–50%, and 51%–75% of their patients with prophylaxis (Figure 4). The range of responses to patients with moderate disease likely speaks more of the number of disease phenotypes that can be categorized as ‘moderate’ than a specific lack of care provision, with only some patients requiring prophylactic treatment as standard of care (e.g. those with moderate hemophilia with severe phenotype, or those at higher risk due to age, joint status, individual PK, lifestyle, etc.).

Estimated percentage of patients currently using prophylactic treatment for mild, moderate, severe hemophilia.
Of those respondents treating patients with prophylaxis, only 5% reported an annualized bleeding rate of zero in >76% of their patients with severe hemophilia. A higher percentage (32%) reported an annualized bleeding rate of zero in >76% of their patients with moderate hemophilia, and two-thirds (68%) reported an annualized bleeding rate of zero in >76% of their patients with mild hemophilia (Figure 5).

Estimated percentage of patients on prophylaxis with an annualized spontaneous bleeding rate of 0.
Management of patients with inhibitors
The majority of centers (95%) indicated that ITI is still a priority in patients with inhibitors, but that shifts in treatment practices mean that ITI is now more commonly used alongside other treatment approaches (e.g. emicizumab prophylaxis). Despite this high number of respondents indicating ITI as a continued priority, its role as a primary means of disease management in the field appears to be increasingly subject to interpretation, with factors including previous success/failure of ITI, efficacy of any current therapy (or therapies), venous access, quality of life (QoL; as related to injection-burden associated with ITI), and availability of alternative or combination therapies commonly being used to guide treatment decisions.
Management of musculoskeletal complications
Musculoskeletal assessment in patients with moderate or severe hemophilia is most commonly performed by the hematologist (68%) or the physical therapist (47%). The annual bleeding rate, hemophilia joint health score, health-related quality-of-life (QoL) assessment, and other musculoskeletal assessments are performed to a varying degree across centers surveyed, with annualized bleeding rate being the most commonly employed outcome measure (used in >76% of patients with moderate or severe hemophilia in 85% of centers).
Management of specific conditions and comorbidities
All of centers refer patients to relevant specialized care for the management of comorbidities. A fast track for referral is common (full and partial in 58% and 26% of centers, respectively), but not universal.
Outcome assessment
The use of outcome measures is universal in centers surveyed, but the specific tools utilized vary across centers. Magnetic resonance imaging (MRI) and X-ray are available in all centers; QoL questionnaire use is common (85% of centers) but not yet universal.
All centers have a strategy for personalization of treatment; most (85% of centers) apply this strategy irrespective of age and disease severity, and almost all centers (95%) support shared decision-making. Most centers extended this to allowing some [5 of the 19 centers surveyed (26%)] or all [14 of the 19 centers surveyed (74%)] patients to choose between products, although sometimes the range was limited or restricted.
Use of PK tools for treatment personalization is near-universal (95% of centers); most used tools were WAPPS-HEMO (90%) and my-PKFiT (58%); these were reported as a valuable innovation by 66% of our respondents (www.wapps-hemo.org/ and www.advate.com/mypkfit) . A similar level of value was placed on patient e-diaries, which were indicated as being a valuable innovation by 61% of respondents; however, around half of our respondents reported that as a resource, patient e-diaries were still lacking in their center (Figure 2).
In addition, around half of our respondents indicated that audits, patient satisfaction surveys, and focus groups were held, but limited survey data prevents further assessment or inference into the value of these activities.
Conclusion
Comparing the results of this survey to those of an earlier survey, conducted in 2012 and including a similar patient population across a similar range of countries and centers, we see a clear evolution in the ways both people with hemophilia and the disease itself are managed. At that time, centralized care was not available for all patients, and some aspects of the way national care was organized (use of registries and local aspects, such as physiotherapy coverage, formal pediatric care, and laboratory services) were lacking. In terms of national coordination and delivery of hemophilia care, for example, just five of the 14 countries surveyed in 2012 had formal mechanisms in place to ensure networking/collaboration, and just eight had a central patient registry. 19
In 2022, we have started to see to the tangible benefits of developments in protocols of care that have been driven by efforts of the hemophilia community over the past decade – efforts that are bringing real-world practices into close alignment with the Principles of Care for people with hemophilia as outlined by the WFH (see Table 1). 2
All centers surveyed have at least one accreditation (with many having more than one), and collaboration between centers and participation in national patient registries is near-universal. All centers surveyed have access to laboratory services (a fully accredited hemostasis lab in many cases), and many offer genetic services supported by external quality assurance. In terms of patient management, 24/7 support is commonplace, as is the use of telemedicine. Age-appropriate approach care is also the norm in centers where children are treated.
The use of prophylactic treatment is well-aligned across all centers surveyed and is near-universal in patients with severe hemophilia; centers are also aligned where the use of ITI is concerned, echoing industry and academic shifts toward a combined approach that is centered on preventive care guided by the patient condition (e.g. prophylaxis with emicizumab) rather than reactive care.
The use of specialist- and patient-reported outcomes assessment approaches is also encouraging, with musculoskeletal and annualized bleeding rate assessment measures, QoL surveys, and PK tools being regularly utilized to guide personalization of treatment in most centers surveyed. Participation in staff development and training is also near-universal across centers (with performance review and clinical governance being undertaken in more than half of centers surveyed), as is involvement in clinical trials and research (although patient enrollment is generally low across all centers).
Although our survey provides a valuable and generally positive snapshot of the current approach to hemophilia treatment, reflecting a clear evolution in our approach to all people with hemophilia, it should not be considered a universal view. Even with a focus on centers in higher-resource countries, such as is presented here, a number of concerns can be seen to persist – the key concerns revealed by our survey being costs and accessibility as related to novel therapies, time limitations (as related to research in particular), and human resources (in terms of new doctors entering the field). It would be remiss not to address the limitations of our survey – namely, that the focus is on a limited number of larger centers in countries that are generally accepted as being able to offer a higher level of hemophilia care in a region marked by disparities across the range of subjects under discussion.
However, and despite these limitations, we are still able to present a valuable overview of the way hemophilia is currently managed in many countries in the region, and, perhaps mostly importantly, our data clearly indicate that specialized hemophilia treatment centers will continue to play a central role in the management of hemophilia: hemophilia is a rare disease, and progress of its management includes the use of highly advanced and specific therapies which must not be supervised solely by Primary Care Physicians. However, standards and protocols, as well as the hemophilia treatment centers themselves, will have to continue to evolve if they are to provide the highest level of care. To meet this requirement, there is a clear need for engaging, ongoing educational programs for healthcare professionals working in the field of hemophilia which can be adjusted to the changing landscape of hemophilia therapy. A good example is gene therapy, which represents an area where implementation has been perceived as a great challenge by most respondents to this survey. It seems that participation in clinical trials of innovative therapies may serve as a good path to increase expertise of teams working in hemophilia treatment centers.
Another important finding of our survey is the increasing role of the hemostasis lab in the management of people with hemophilia. With the advent of extended half-life products, NRTs, NFRTs, gene therapy, and, in the near future, further ‘breakthrough’ therapies, the role of the hemostasis lab in the monitoring of hemophilia therapy will be even more significant. Therefore, close collaboration between clinics and laboratories (including, in some cases, better integration between the clinical and laboratory services), and collaborative participation in educational programs, should be considered a key element of any initiatives.
The life expectancy of people with hemophilia today (including those with severe hemophilia) is close to that of those without hemophilia, meaning a significant proportion of people with hemophilia also suffer from severe concomitant diseases associated with aging (e.g. malignancies and cardiovascular disorders). One of the critical tasks hemophilia treatment centers face is to secure an adequate ‘fast track’ to other specialists; as we learned from this survey, this is not always available. One should keep in mind that, in contrast to replacement therapy, management of people with hemophilia treated with novel therapies (particularly those requiring invasive procedures or antineoplastic or antithrombotic therapies) may be even more challenging, and therefore a closer collaboration with other specialists will be necessary.
Finally, our survey demonstrates that cost considerations remain a very real part of hemophilia management, and that as more new and highly innovative products enter the market, each bringing a unique set of monitoring and patient-management requirements, far-reaching initiatives and intraregional and extraregional collaborations will need to be enacted if all centers – not just those in higher resource countries – are to offer the most advanced level of care. Finding adequate solutions that will allow this level of universal access to hemophilia treatment might prove to be the greatest challenge of all.
Supplemental Material
sj-docx-1-tah-10.1177_20406207221088462 – Supplemental material for Changing paradigms of hemophilia care across larger specialized treatment centers in the European region
Supplemental material, sj-docx-1-tah-10.1177_20406207221088462 for Changing paradigms of hemophilia care across larger specialized treatment centers in the European region by Jerzy Windyga, Ana Boban, Irena Zupan, Niamh O’Connell and Cedric Hermans in Therapeutic Advances in Hematology
Supplemental Material
sj-docx-2-tah-10.1177_20406207221088462 – Supplemental material for Changing paradigms of hemophilia care across larger specialized treatment centers in the European region
Supplemental material, sj-docx-2-tah-10.1177_20406207221088462 for Changing paradigms of hemophilia care across larger specialized treatment centers in the European region by Jerzy Windyga, Ana Boban, Irena Zupan, Niamh O’Connell and Cedric Hermans in Therapeutic Advances in Hematology
Footnotes
Acknowledgements
All authors worked on designing the survey, analyzed the data, and contributed to the writing of the paper. The authors thank the ECHN group members who participated in the research by filling out the survey: Jan Blatný and Jan Máchal (Czech Republic); Victor Jiménez-Yuste (Spain); Irena Preloznik Zupan (Slovenia); Niamh O’Connell (Ireland); Cedric Hermans (Belgium); Pål Andre Holme (Norway); Christoph Male (Austria); Ana Boban (Croatia); Jerzy Windyga (Poland); Maria Elisa Mancuso (Italy); Angelika Batorova (Slovakia); Katharina Holstein, Robert Klamroth and Christoph Königs (Germany); Jan Astermark (Sweden); Karin Fijnvandraat (Netherlands); Gili Kenet (Israel); Sandra Le Quellec (France); Kaan Kavakli (Turkey). Medical writing assistance was provided by Daniel Guns, MSc, and Kim Grootscholten, MSc, from COR2ED, Basel, Switzerland.
Author contributions
Conflict of interest statement
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: J.W. receives grant/research support and lectures honoraria from Alnylam, Bayer, CSL Behring, Kedrion, LFB, Novo Nordisk, Octapharma, Rigel, Roche, Sanofi, Siemens, Sobi, Takeda, and Werfen. A.B. has received honoraria or consultation fees from Bayer, Sobi, Takeda, Roche, Octapharma; and speaker bureau fees from Bayer, CSL Behring, Novo Nordisk, Pfizer, Takeda, Sobi, and Roche. I.Z. has received consulting or speaker fees from Novo Nordisk, Bayer, Roche, Takeda, Octapharma, Pfizer and Sobi. She has no relevant conflict of interest regarding this work. N.O’C. has received research support or served as PI for Sobi, Takeda, UniQure and Freeline; and has received speaker fees or served on advisory boards for Novo Nordisk, Pfizer, Roche, Bayer, Sobi, and Freeline. C.H. has received grants/research support from Bayer, CAF-DCF, CSL-Behring, Novo Nordisk, Pfizer, and Sobi; honoraria or consultation fees from: Bayer, Biomarin, CAF-DCF, CSL-Behring, Kedrion, LFB, Novo Nordisk, Octapharma, Pfizer, Sanofi, Sobi, and Uniqure; and speaker bureau fees from Bayer, Biomarin, CAF-DCF, CSL-Behring, LFB, Novo Nordisk, Pfizer, and Sobi.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This article was written on behalf the European Collaborative Hemophilia Network (ECHN). ECHN was supported by an Independent Educational Grant from Takeda.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.