
Abstract
Myelofibrosis is one of the Philadelphia chromosome (Ph)-negative myeloproliferative neoplasms with heterogeneous clinical course. Though many treatment options, including Janus kinase (JAK) inhibitors, have provided clinical benefits and improved survival, allogeneic hematopoietic stem-cell transplantation (AHSCT) remains the only potentially curative therapy. Considering the significant transplant-related morbidity and mortality, it is crucial to decide who to proceed to AHSCT, and when. In this review, we discuss recent updates in patient selection, prior splenectomy, conditioning regimen, donor type, molecular mutation, and other factors affecting AHSCT outcomes. Relapse is a major cause of treatment failure; we also describe recent data on minimal residual disease monitoring and management of relapse. In addition, emerging studies have reported pretransplant therapy with ruxolitinib for myelofibrosis showing favorable results, and further research is needed to explore its use in the post-transplant setting.
Introduction
Myelofibrosis (MF) is a Philadelphia chromosome (Ph)-negative myeloproliferative neoplasm, characterized by bone marrow fibrosis, leukoerythroblastosis in blood, extramedullary hematopoiesis, splenomegaly, constitutional symptoms, and an increased risk of transformation to acute myeloid leukemia (AML). The disease can arise de novo as primary MF (PMF) or evolve from polycythemia vera (post PV-MF), or essential thrombocythemia (post ET-MF). It primarily affects the elderly, with a median age at diagnosis of 67 years. 1 Though Janus kinase (JAK) inhibitors have broadened the treatment options in MF, allogeneic hematopoietic stem-cell transplantation (AHSCT) remains the only known curative therapy. In this review, we describe the available data and summary current recommendations on transplantation for myelofibrosis.
Prognosis and risk stratification
The clinical course of MF is heterogeneous, ranging from an indolent course persisting for decades to rapidly progressive disease with a survival of a few months. Prognosis is currently assessed by the International Prognostic Scoring System (IPSS) at diagnosis, which incorporates the following five risk factors: age (>65 years), anemia (hemoglobin <10 g/dl), leukocyte count (>25 × 109/l), circulating blasts (⩾1%), and constitutional symptoms. 2 The presence of 0, 1, 2, and ⩾3 factors are categorized as low, intermediate-1, intermediate-2, and high-risk disease, with median survival of 135, 95, 48, and 27 months, respectively. The Dynamic International Prognostic Scoring System (DIPSS) uses the same risk factors as the IPSS, but more weight is assigned to anemia, and it allows for prognostic prediction at any time during the disease course. 3 DIPSS was later refined as DIPSS-plus with inclusion of three additional risk factors: transfusion dependence, platelet count <100 × 109/l, and unfavorable karyotype. 4 For patients with post-PV/ET MF, the MF secondary to PV, and ET prognostic model (MYSEC-PM) has been defined and validated for risk stratification.5–7 This new score assigns 2 points to hemoglobin level <11 g/dl, circulating blasts ⩾3% and CALR-unmutated genotype, 1 point to platelet count <150 × 109/l and constitutional symptoms, and 0.15 points to any year of age. Patients are allocated into four risk categories with different survival: low (median survival not reached), intermediate-1 (9.3 years), intermediate-2 (4.4 years), and high (2 years) risk. Very recently, a large study confirmed that the MYSEC-PM allowed a more accurate prediction of survival after AHSCT than the DIPSS for post-PV/ET MF. 8
Molecular risk stratification
JAK2, CALR, and MPL are considered mutually exclusive driver mutations in MF. In general, CALR mutated patients are of younger age, with higher platelet counts and lower leukocyte counts, and have a favorable overall survival (OS).9,10 MPL does not seem to be prognostically relevant. 11 The prognosis impact of JAK2V617F in MF remains controversial. Some studies found JAK2 mutated patients had inferior survival 12 and a higher risk of leukemic transformation (LT) 13 ; however, others did not observe such an impact.14,15 Besides, about 10% of MF patients have JAK2/CALR/MPL triple-negative disease,16,17 and usually have the worst prognosis.9,10
In addition, several researchers found ASXL1, EZH2, SRSF2, or IDH1/2 mutations predicted poor outcomes.18–21 In a study of 879 patients with PMF, Vannucchi and colleagues showed that ASXL1, SRSF2, and EZH2 mutations were associated with shorter OS, and mutations in IDH1 and SRSF2 with LT. 21 Moreover, the detrimental effects of these mutations were additive.22,23 With incorporation of molecular mutations, the mutation-enhanced IPSS (MIPSS70) for transplant-age patients have been described, 24 which highlights the importance of mutational profiling on refining patient risk.
Patient selection and optimal timing of AHSCT
According to the IPSS, DIPSS, and DIPSS-plus scores, patients with intermediate-2 and high-risk disease have median survival of less than 5 years,2–4 and should be considered potential candidates for AHSCT. 25 A large retrospective study determined outcomes in 438 PMF patients who received AHSCT (n = 190) or conventional therapies (n = 248). 26 The results showed that patients with intermediate-2 or high-risk, according to the DIPSS model, clearly benefited from AHSCT, with relative risk (RR) of death of 0.55 and 0.37, respectively. Patients at low risk benefited from nontransplant therapy (RR = 5.6), whereas individual counseling was indicated for those at intermediate-1 risk (RR = 1.6, p = 0.19). In a consensus publication by the European Blood and Marrow Transplantation group and the European LeukmiaNet (EBMT/ELN), 25 patients with intermediate-1 risk disease up to age 65 years should also be considered candidates for AHSCT if they have either refractory, transfusion-dependent anemia, a percentage of blasts in peripheral blood (PB) >2%, or adverse cytogenetics (as defined by the DIPSS-plus classification). Besides, as mentioned above, JAK2/CALR/MPL triple-negative or ASXL1 mutation predicts poor outcomes, intermediate-1 risk patients with these molecular mutations are also suggested AHSCT if a suitable donor is available. 25
The optimal timing of AHSCT for MF is controversial, especially in the era of JAK inhibitors. Though not curative, the first JAK1/2 inhibitor Ruxolitinib has shown clinical benefits in patients with intermediate-2 and high-risk MF, including spleen size reduction and improvement of constitutional symptoms and also survival benefit.27–29 A major dilemma is when to proceed to AHSCT in a patient who responds well to JAK inhibitor. Early AHSCT may lead to significant morbidity and mortality, while delaying AHSCT may lead to a worse outcome due to advanced-stage disease, increasing age or LT. Some authors suggested that patients whose therapeutic goal was cure should still be referred for AHSCT, 30 even if they are responding to JAK1/2 inhibitors. This approach is not contradictory because there is a sound rationale for combining JAK1/2 inhibitor therapy with AHSCT, which we will discuss later.
Pretransplant splenectomy
Splenomegaly reflects an expansion of the underlying malignant clone in MF, and many reports have shown poor transplant outcomes in patients with splenomegaly.31,32 However, the role of splenectomy before AHSCT remains controversial. Some data observed faster engraftment in splenectomized patients.33–36 A retrospective study included 26 patients with MF, of them 11 patients had undergone splenectomy and they had faster granulocyte recovery than nonsplenectomized patients (18 days versus 23 days, p = 0.04). 33 In contrast, other researchers did not observe any difference in transplantation outcomes between patients who underwent splenectomy or not.37,38 A study assessed the impact of spleen status on transplant outcome in 9683 patients with myeloid malignancy, including MF (472 splenectomy, 300 splenic irradiation; 1471 with splenomegaly). Despite the facilitation of engraftment after splenectomy, the OS was similar among groups. 39 Kroger and colleagues even found that prior splenectomy was associated with an increased incidence of relapse. 40 Taken together, the data of favorable outcome with splenectomy are not sufficient, and the procedure of splenectomy is associated with significant risk of perioperative complications (27.7%) and mortality (6.7%) 41 ; hence, routine pretransplant splenectomy is not recommended. Moreover, as JAK inhibitors have shown clinical benefit in reducing spleen size,27–29 they may serve as an alternative to splenectomy in patients with significant splenomegaly.
Conditioning regimens
Many retrospective studies have demonstrated the curative potential of myeloablative conditioning (MAC) AHSCT in MF patients, with an OS of 30–60% and event-free survival (EFS) of 25–50%.34,42–47 However, the transplant-related mortality (TRM) is rather high, ranging from 30% to 48% at 1 year, which limits its applicability to young patients with good performance status (PS). The introduction of reduced intensity conditioning (RIC) has expanded the scope of AHSCT to older patients, or patients with significant comorbid conditions. Over the past decades, many studies have reported encouraging results of RIC AHSCT in patients with MF.42,48–53 In a prospective multicenter study, 103 patients received fludarabine/busulfan (FB)-based RIC regiment followed by AHSCT. The cumulative incidence of nonrelapse mortality (NRM) at 1 year was 16%, relapse at 3 years was 22%, and 5-year OS was 67%. 40
Among many available RIC regimens, FB or fludarabine/melphalan (FM) are most commonly used for MF.31,40,44,49,51,54 One study compared FB and FM regimens, and a total of 160 MF patients (FB group, n = 105; FM group, n = 55) were included. Multivariable analyses revealed no significant differences in progression-free survival (PFS) between the two groups (52% versus 33%, p = 0.89); however, the relapse rate was significantly lower in the FM group (HR = 9.21; p = 0.008), and a trend toward reduced NRM was seen in the FB group (HR = 0.51; p = 0.068). 52 This study concluded that both regimens were efficient, the FM regimen appeared more toxic but with augmented control of disease. Recently, a retrospective study analyzed outcomes of 61 patients with MF who underwent AHSCT with the following three RIC regimens: FB, FM or Fludarabine Bischlorethyl-nitroso-urea/carmustine Melphalan (FBM). OS, acute graft-versus-host disease (GVHD) and relapse were not different in the three groups; however, 100% donor chimerism was seen in more frequently at day +30 and day +100 in patients who received FBM or FM than FB. 53
There is no prospective randomized trial comparing MAC with RIC, and all results were based on retrospective comparisons. Most studies found that patients who performed with RIC had similar outcomes to patients with MAC though they were older or with poor PS.36,45,54–56 However, a very large long-term study by Robin and colleagues observed poor results in patients with RIC AHSCT. 57 The study analyzed outcome in 1055 patients with MF undergoing transplant between 1995 and 2014, of which 645 patients received a RIC regimen. The 10-year OS, disease free survival (DFS), and relapse for 2-year survivors were 74%, 64%, and 21%, respectively. RIC was associated significantly with lower DFS and higher relapse. The consensus of the EBMT/ELN is that patients with older age or comorbidities should select a lower intensity regimen, while for patients with advanced disease and good PS a more intensive regimen is more appropriate. 25
Factors affecting AHSCT outcomes
Patient-related factors
Though older age has been considered as an independent risk factor for inferior transplant outcomes,40,42,58–60 it should not be a limiting factor, especially with the increasing use of RIC regimens. Samuelson and colleagues reported encouraging results of AHSCT in 30 patients aged 60–78 (median 65) years, with PMF or post-PV/ET MF. Conditioning regimens varied from very low intensity (fludarabine plus 2 Gy total body irradiation) to high dose (busulfan plus cyclophosphamide). Their 100-day mortality was 13%, 3-year OS and PFS were 45% and 40%, respectively. 61 In addition, a few studies identified no influence of age on post-transplant outcomes,38,50,62 what counted more were patient’s comorbidities and PS. Scott and colleagues showed in their study that higher Hematopoietic Cell Transplantation Comorbidity Index (HCT-CI) scores was associated with increased overall mortality and NRM. 38 In another study, PS was evaluable in 70 PMF patients, and PS ⩾2 (versus PS 0–1) predicted a higher NRM and lower OS. 63
Molecular mutations
Molecular mutations have prognostic value not only in the nontransplant setting, but also in the AHSCT setting. The presence of CALR mutations predicts a better post-transplant outcome for MF.59,64 A German group evaluated the impact of CALR mutations in 133 patients with MF who underwent AHSCT, 59 of whom 28 (21%) had mutated CALR. Compared with wild-type CALR patients, patients with mutated CALR had a significant higher 4-year OS (82% versus 56%, p = 0.043) and lower 4-year NRM (7% versus 31%, p = 0.024) after AHSCT. The role of JAK2V617F status after transplant remains controversial. Some data indicated that patients with wild-type JAK2V617F had inferior outcome after AHSCT.58,60 In a series of 162 patients with MF who receive AHSCT, JAK2V617F status was available in 139 patients, of whom 95 were JAK2V617F-positive and 44 were JAK2V617 wild-type. Deaths occurred more frequently in the JAK2-wt group (50% versus 25%), and this group had a worse 5-year OS (44% versus 70%) and DFS (32% versus 50%) than JAK2V617F mutated patients. 58 However, there were also studies identified no influence of JAK2V671F mutation status on post-transplant outcome.38,51,65 Therefore, further research is needed to assess the prognostic impact of JAK2 mutation for MF patients after AHSCT.
Degree of bone marrow fibrosis
Bone marrow fibrosis (BMF) has been demonstrated not to be a barrier to AHSCT, and several reports have shown a complete reversal of fibrosis between 6 and 12 months after transplantation.66,67 In a series of 24 patients with MF who underwent RIC AHSCT, all had advanced fibrosis MF-2 (n = 13) or MF-3 (n = 11) before allografting. After transplantation, a complete (MF-0) or nearly complete (MF-1) regression of BMF was seen in 59% at day +100, in 90% at day +180, and in 100% at day +360. 67 Some data found that a prior higher degree of fibrosis was associated with poor outcomes after AHSCT,34,60 and rapid BMF regression predicted a favorable survival. Kröger and colleagues correlated regression of BMF on day 30 and 100 with post-transplant survival in 57 patients with MF. Before AHSCT, 41 patients were classified as MF-3, and 16 were classified as MF-2. On day +30, 21% of the patients were MF-0/-1, and on day +100, 54% were MF-0/-1. Patients with MF-0/-1 at day +100 were related to a lower risk of TRM and relapse, which resulted in a significantly higher 5-year OS (96% versus 57%, p = 0.04). 68
Donor type
Some reports found similar outcomes between patients who received HLA-matched sibling donor (MSD) and unrelated donor (MUD) AHSCT for MF.38,40,42,43 Conversely, a prospective phase II clinical trial found poor survival in patients with MUD AHSCT. 51 In this study, 32 patients with sibling donors received FM conditioning regimen, and 34 patients with unrelated donors received FM plus antithymocyte globulin conditioning regimen. NRM was 22% in siblings and 59% in unrelated AHSCT. With a median follow-up of 25 months, the OS was 75% in the sibling group and only 32% in the unrelated group.
For patients who lack MSD or MUD, mismatched related donors (MMRD) provide an attractive donor source due to widespread availability. Bregante and colleagues conducted a retrospective analysis of 95 patients with MF who were allografted between 2001 and 2014, and they found haploidentical donor transplantations improved significantly with years. 69 Patients were studied in two time intervals: 2000–2010 (n = 58) and 2011–2014 (n = 37). More family haploidentical donors (54% versus 5%, p < 0.0001) were seen in the most recent group. TRM at 3 years in the 2011–2014 period versus 2000 to 2010 period was 16% versus 32% (p = 0.10), the relapse rate 16% versus 40% (p = 0.06), and actuarial survival 70% versus 39% (p = 0.08). Improved survival was most pronounced in alternative donor grafts (69% versus 21%, p = 0.02), compared with matched sibling grafts (72% versus 45%, p = 0.40). A recent study reported outcomes of 56 MF patients transplanted from MMRD between 2009 and 2015. At 2 years, the cumulative incidence of primary graft failure was 9% and secondary graft failure was 13%. The cumulative incidence of acute GVHD grades II to IV and III to IV was 28% and 9% at 100 days, chronic GVHD at 1 year was 45%. With a median follow up of 32 months, the 2-year OS, PFS and NRM was 56%, 43%, 38%, respectively. 70 It was the largest study of patients with MF undergoing MMRD AHSCT. The acceptable levels of GVHD and encouraging PFS and OS rates demonstrated its feasibility. However, strategies to enable sustained engraftment and reduce NRM will require further research.
Stem cell source
Published studies failed to show significant difference in outcomes of bone marrow (BM) and peripheral blood stem-cell (PBSC) grafts in patients with MF.35,38,44,63,71 However, PBSC had favorable impact on engraftment in some reports. A study by Robin and colleagues evaluated transplant outcomes in 147 patients with MF, 35 with 39 patients received BM source of stem cell and the others received PBSC. The probability of engraftment was higher in PBSC group than in BM group (93% versus 82%, p = 0.008). Two other studies found BM was a risk factor for delayed engraftment or failure of sustained engraftment for MF patients.34,36 Considering these factors, PB is the most appropriate stem cell source.
Due to its high graft failure, there are little data on the use of umbilical cord blood (UCB) in MF patients. A study from Japan included 224 patients to evaluated different donor sources for PMF, including 29 patients with unrelated UCB. Compared with MSD BM transplantation, the incidence of neutrophil and platelet recovery after unrelated UCB transplantation were significantly lower, and NRM at 1 year was higher (41% versus 16%, p = 0.046). 72 Therefore, careful management is required for patients who proceed to UCB AHSCT, especially in the early period.
Leukemic transformation
LT is observed in approximately 20% of patients with MF and the prognosis is dismal, with a median survival of less than 3 months.73,74 Risk factors for LT were unfavorable karyotype, thrombocytopenia, and increased circulating blasts.75,76 Molecular abnormalities such as IDH-1/2, SRSF2, EZH2, or ASXL1 also predicted higher risk of LT. 77 Patients with LT may achieve long-term remission after induction chemotherapy and AHSCT. Alchalby and colleagues conducted a study of 46 patients who received AHSCT for AML evolving from MF. Before AHSCT, 42 patients received induction chemotherapy, while only 9 achieved complete remission (CR), 10 achieved a minor or partial remission, and 19 were refractory or had progressive disease at the time of AHSCT. The 3-year PFS, OS, and relapse rates were 26%, 33%, and 47%, respectively, and the only significant factor for survival was CR before transplantation. 77 Hence, AHSCT after chemotherapy is associated with a potential survival benefit, especially for patients with CR before transplantation.
Role of JAK inhibitors
Ruxolitinib is the first JAK inhibitor approved by the US Food and Drug Administration for patients with intermediate- or high-risk MF and in Europe for symptomatic MF patients with splenomegaly, irrespective of disease status. The results of COMFORT-I and COMFORT-II showed that ruxolitinib rapidly reduced splenomegaly and improved MF-related symptoms and quality of life.27,28 Several studies78–83 suggested pretreatment with ruxolitinib was well tolerated and might improve outcome after AHSCT (Table 1). Besides, two studies found patients who responded well to ruxolitinib had better transplant results.79,80 In one study, 100 patients with MF were stratified into five groups based on clinical status and response to JAK1/2 inhibitors at the time of AHSCT. OS at 2 years was 61%, and this was 91% for those who experienced clinical improvement, while only 32% for those who developed LT on JAK1/2 inhibitors. 79
Major studies of ruxolitinib therapy prior to AHSCT for myelofibrosis.
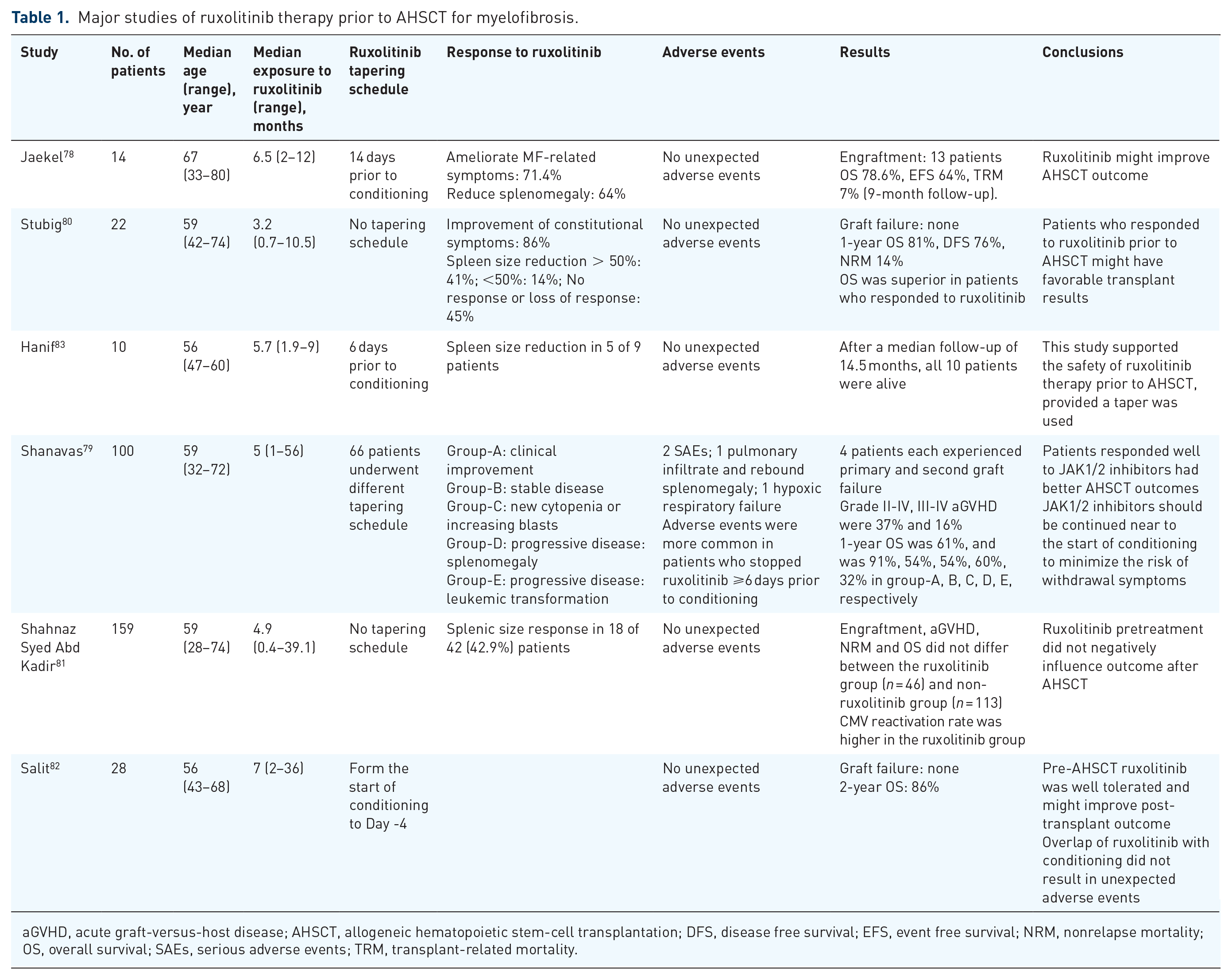
aGVHD, acute graft-versus-host disease; AHSCT, allogeneic hematopoietic stem-cell transplantation; DFS, disease free survival; EFS, event free survival; NRM, nonrelapse mortality; OS, overall survival; SAEs, serious adverse events; TRM, transplant-related mortality.
Adverse events associated with ruxolitinib in pretransplant setting including ruxolitinib withdrawal syndrome and increased risk for infections. Preliminary results of a prospective research from France reported unusual serious adverse effects such as tumor lysis syndrome, cardiogenic shock, and sepsis. 84 Of note, a large retrospective study observed two serious adverse events in MF patients who stopped JAK inhibitor ⩾6 days prior to conditioning therapy. 79 Rates of adverse symptoms were very low in patients who continued JAK inhibitor near to transplant conditioning therapy. Hanif and colleagues reported 10 patients who underwent AHSCT for MF and all patients were pretreated with ruxolitinib. 83 The steady state dose of ruxolitinib was 20 mg BID, and a standard tape schedule was employed starting 6 days prior to conditioning. At 6 days, 96 h, 72 h, 48 h, and 24 h prior to conditioning, ruxolitinib was reduced to 15 mg BID, 10 mg BID, 5 mg BID, 5 mg Daily, and None, respectively. No unexpected adverse events were observed upon ruxolitinib withdrawal. Therefore, it is recommended that the drug be initiated at least 2 months before transplant, and weaning start 5–7 days prior to conditioning, with the drug stopping the day before conditioning. 25 Ruxolitinib has been shown to inhibit in vitro and in vivo dendritic cell activation, migration, and antigen-specific T-cell response,85,86 resulting in an increased risk for infection, particularly viruses. In a small study of 12 patients with MF who were treated with ruxolitinib and underwent AHSCT, ruxolitinib was continued until stable engraftment. The authors demonstrated a higher incidence (41%) of cytomegalovirus reactivation and the onset was earlier compared with a historical group. 87 In summary, careful attention should be paid to these adverse events when received ruxolitinib prior to AHSCT.
There is little indication for JAK1/2 inhibitors after AHSCT for MF. However, they could be considered in patients who relapse to decrease the symptom burden. They may be also effective in the treatment of steroid-refractory GVHD by suppressing the production of pro-inflammatory cytokines, which needs prospective trials to validate it.
Post-transplant management
Graft failure
Graft failure is one of the major complications in patients with MF who undergo AHSCT, especially after RIC regimen, with the incidence ranging from 2% to 24%.40,51,88 Factors associated with engraftment are: donor type,51,71 stem cell source,35,89 intensity of conditioning regimen,44,90 spleen size,33,88 and age. 88 A study from Netherlands assessed the effect of conditioning regimens on graft failure in MF, and 53 patients with RIC or nonmyeloablative (NMA) regimens were included. The cumulative incidence of graft failure within 60 days was 28%, and this was higher in patients who received NMA conditioning (44% versus 16%, p = 0.03). 90 Data from a study of 100 patients with MF who received AHSCT showed the incidence of poor graft function was 17%, and persistence of splenomegaly at +30 day was a significant factor for poor graft function. 88 The EBMT/ELN experts recommend that in patients with poor graft function with full donor chimerism and absence of acute GVHD, myelosuppressive agents (ganciclovir, trimethoprim-sulfamethoxazole, and mycophenolate mofetil) should be removed, while with late decline of graft function, CD34-selected stem cell boost is suggested. In patients with graft failure and no autologous reconstitution, the only available option is a second transplant. 25
Monitoring of residual disease and treatment of relapse
Relapse is a major cause of treatment failure for MF patients after AHSCT, with an incidence of 10–20% with MAC regimens and 29–43% with RIC regimens.40,42,43,50 As the three driver mutations, JAK2, MPL, and CALR, are detectable in approximately 90% of patients with MF, they can be used to monitor minimal residual disease (MRD) after AHSCT. Wolschke and colleagues screened 136 MF patients who underwent AHSCT for MRD for JAKV617F (n = 101), MPL (n = 4), or CALR (n = 31) mutation. The cumulative incidence of relapse at 5 years was 26%, and patients with detectable mutation at day +100 or at day +180 had a significant higher risk of clinical relapse than molecular-negative patients (62% versus 10%, p < 0.001 and 70% versus 10%, p < 0.001, respectively). 91 Two other studies found higher JAK2V617F allele burden early after AHSCT indicted an increased incidence of relapse.92,93 One of them applied allele-specific quantitative polymerase chain reaction (PCR) to detect JAK2V617F, by 6 months post-transplant, the JAK2V617F allele burden was 43-fold higher in relapse/refractory disease patients than in those in CR. 93 In patients lacking JAK2V617F mutation, specific and sensitive assays to detect MPL or CALR mutation to monitor MRD had also been reported, though these studies were relatively small.94–97
For patients with evidence of MRD or clinical relapse, discontinuation of immune-suppressive drugs, donor lymphocyte infusions (DLIs) or a second AHSCT are treatment strategies of choice. Klyuchnikov and colleagues reported their multicenter experience on the use of DLIs and a second RIC AHSCT in 30 patients with MF who relapsed (n = 27) or experienced graft failure after AHSCT. 98 A total of 26 patients received a median number of three DLIs, and 10 patients achieved CR to DLIs; 13 nonresponders and 4 patients who did not receive DLI underwent a second AHSCT. Overall responses after second AHSCT were seen in 12/15 patients. After a median follow-up of 27 months, the 2-year OS and PFS for all 30 patients was 70% and 67%, respectively. This showed that a two-step salvage strategy was an effective approach in relapsed MF. In addition, an earlier study reported on 17 patients with MF who received DLI either for clinical relapse (salvage DLI; n = 9) or residual disease monitored by JAK2 mutation (preemptive DLI; n = 8). 99 In contrast to salvage DLI, patients who received preemptive DLI had higher complete molecular remission rate (100% versus 44%, p = 0.04), and none of these patients developed grade II–IV acute GVHD. The authors concluded that preemptive DLI seemed to be more effective and less toxic than salvage DLI, which highlighted the importance of MRD monitoring with driver mutations.
Conclusion
AHSCT remains the only curative therapy for patients with MF. The optimal conditioning regimen has not been defined and should be based on patient age, comorbidity, and PS. MSD and MUD are preferred, mismatched related donor provides an attractive alternative donor source. JAK inhibitors have proved clinical benefits for MF patients, and further researches are needed to explore the safety and effectiveness of pretransplant therapy with ruxolitinib. Molecular mutations not only have prognostic value but also serve as MRD markers to predict early relapse. For patients with relapse, reduction of immune-suppressive drugs, DLIs, or a second AHSCT are effective treatment choices.
Footnotes
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and publication of this article: This work was supported by grant from the National Megaproject on Key Infectious Diseases (grant number 2017ZX10202102); the CAMS Initiative for Innovative Medicine (grant number 2016-I2M-1-017), Tianjin Municipal Natural Science Foundation (grant number 18JCZDJC34400) and the Nonprofit Central Research Institute Fund of Chinese Academy of Medical Sciences (grant number 2018PT32034).
Conflict of interest statement
The author(s) declare that there is no conflict of interest.