
Abstract
Allogeneic hematopoietic stem-cell transplantation (HSCT) is the most effective approach for many patients with hematologic malignancies. Unfortunately, relapse remains the most common cause of death after allogeneic HSCT, and the prognosis of relapsed disease is poor for most patients. Induction of a graft-versus-leukemia (GVL), or graft-versus-tumor, effect through the use of donor leukocyte infusion (DLI), or donor lymphocyte infusion, has been remarkably successful for relapsed chronic myelogenous leukemia. Unfortunately, response to DLI in other hematologic malignancies is much less common and depends on many factors including histology, pace and extent of relapse, and time from HSCT to relapse. Furthermore, graft-versus-host disease (GVHD) is common after DLI and often limits successful immunotherapy. Ultimately, manipulations to minimize GVHD while preserving or enhancing GVL are necessary to improve outcomes for relapse after allogeneic HSCT.
Introduction
Allogeneic hematopoietic stem-cell transplantation (HSCT) is the most effective, if not the only, curative therapy for many patients with hematologic malignancies. In addition to the intensive conditioning regimen, the antileukemic property of the graft itself is critical for successful transplantation. This graft-versus-leukemia (GVL) effect was first demonstrated in animal models [Barnes et al. 1956] and later through retrospective clinical observations that showed graft-versus-host disease (GVHD) was associated with a lower risk of relapse [Sullivan et al. 1989a, 1989b; Weiden et al. 1981]. Ultimately, GVL was directly demonstrated in human transplantation when donor leukocyte infusions (DLI) effectively restored remission for relapsed chronic myelogenous leukemia (CML) [Porter et al. 1994b; Kolb et al. 1990] Since then, there have been many efforts to harness and maximize the GVL effect in the treatment of hematologic malignancies while minimizing GVHD. We review the use of allogeneic cellular adoptive immunotherapy following HSCT to treat relapsed disease as well as to treat nonrelapse complications such as posttransplantation lymphoproliferative disorder and infections. In order to further enhance this powerful antitumor effect and improve the safety of immunotherapy, novel strategies to define and manipulate both target antigens and effector cells are necessary.
Treatment of relapsed disease
Relapsed disease is the most common cause of death following allogeneic HSCT [Pasquini and Wang, 2010]. Surprisingly, there are limited data regarding the natural history of relapse [Pavletic et al. 2010]. In addition, treatment of relapse has been disappointing for most diseases other than CML [Porter et al. 2011]. The major strategy for treating relapse after allogeneic HSCT has largely been immunotherapy, by withdrawal of immune suppression, or with a second allogeneic transplantation, or with DLI. Withdrawal of immune suppression has been successful in limited case studies [Collins et al. 1992; Higano et al. 1990; Sullivan and Shulman, 1989], although is rarely effective when used alone. Second allogeneic transplantation remains an option for relapse, but is accompanied by significant treatment-related morbidity and mortality, particularly with myeloablative conditioning. In an analysis performed by the Center for International Blood and Marrow Transplant Research (CIBMTR), overall survival following a second allogeneic HSCT for acute or chronic leukemia was dependent on age and time to relapse after the first transplant. Five-year survival was 51% for young patients who relapsed more than 6 months after their first transplant but only 3% for patients over 20 years old who relapsed within 6 months. The cumulative incidence of treatment-related mortality was quite high at 30% [Eapen et al. 2004]. Given these poor options, the use of DLI has become a common therapy for recurrence after allogeneic HSCT, although GVL activity is quite disease dependent.
Disease-specific outcomes using donor leukocyte infusion to treat relapse
Chronic myelogenous leukemia
GVL induction with DLI has been dramatically effective for relapsed CML and can induce sustained long-term molecular remission in most patients who relapse with chronic phase disease [Bacigalupo et al. 1997; Kolb et al. 1990; Pavletic et al.; Porter et al. 1994b; Mackinnon et al. 1995; Van Rhee et al. 1994]. Overall, 76–79% of patients achieve a complete remission (CR) [Collins et al. 1997; Kolb et al. 1995] and most remissions are durable; recurrence rates following DLI-induced remission for chronic phase CML have been approximately 6–9% [Dazzi et al. 2000; Porter et al. 1999].
Treatment of accelerated phase or blast crisis CML with DLI contrasts sharply with that of chronic phase CML, with CR achieved in only 12–28% of patients with accelerated phase or blast crisis CML [Collins et al. 1997; Kolb et al. 1995]. In those patients who do respond, remissions frequently lack durability, with relapse rates greater than 40% [Porter et al. 1999]. Both advanced phase relapse and remission duration following HSCT <9 months were risk factors for poor response [Dazzi et al. 2000].
Tyrosine kinase inhibitors (TKIs) have been given concurrently with DLI for the treatment of relapsed CML in small numbers of patients. Although one retrospective study reports a more rapid achievement of a molecular response with this approach in both chronic and accelerated phase relapses [Savani et al. 2005], other data provide reasons for concern. For instance, TKIs may take CML precursor cells out of the active cell cycle, making them less susceptible to T-cell-mediated cytotoxicity [Jedema et al. 2009]. Furthermore, in vitro, TKIs can inhibit T-cell function and induce apoptosis of activated T cells, activities that could interfere with the cellular immune response and ultimate cure [Seggewiss et al. 2005]. In addition, many patients undergo transplantation only if they are resistant to TKI therapy and therefore it would offer an unclear benefit at the time of relapse. Prospective randomized trials would be necessary to definitively assess the safety and efficacy of concurrent TKIs and DLI. However, these studies will be difficult to perform since so few patients with CML undergo allogeneic HSCT in the modern era.
Acute leukemia and myelodysplasia
Allogeneic HSCT is performed for acute myelogenous leukemia (AML) more than any other disease in North America [Pasquini and Wang, 2010]. Relapse rates remain high, and there is an immediate need for more effective treatment of recurrent disease. Given the limited effective options, GVL induction with DLI is the most common treatment for relapsed AML. Unfortunately, the activity of DLI is disappointing in AML when compared with CML. Large retrospective analyses have reported CR rates to DLI given without chemotherapy of 15–29% [Collins et al. 1997; Kolb et al. 1995]. Patients with a CR, though small in number, can attain durable remissions [Schmid et al. 2007; Porter et al. 1999].
In many cases rapid proliferation of AML and high disease burden cannot be managed with GVL induction alone, which can take weeks to fully develop [Baurmann et al. 1998; Rapanotti et al. 1997]. One strategy to enhance the response rate to DLI in AML is to treat patients with cytoreductive chemotherapy before infusion. The role of pre-DLI chemotherapy was prospectively studied by treating 57 patients, most with relapsed AML following allogeneic HSCT. Induction chemotherapy was followed by DLI mobilized by granulocyte colony-stimulating factor (G-CSF) [Levine et al. 2002]; 27 patients (41%) achieved a CR, and in those who responded, 51% were alive at 1 year and 41% at 2 years. Survival in those who failed to respond to DLI was only 5% overall. In multivariate analysis, time to relapse following HSCT was most predictive of response to DLI (Figure 1). Remission was 3.7 times more likely in patients who relapsed >6 months following transplantation than in those who relapsed within 6 months of transplantation. Similar results were seen in a smaller group of patients with AML treated with chemotherapy followed by G-CSF-mobilized DLI, which confirmed the prognostic value of a remission of >6months following initial HSCT [Choi et al. 2004]. Therefore, for patients with a late relapse following HSCT there is a potent and potentially durable response to DLI plus chemotherapy.
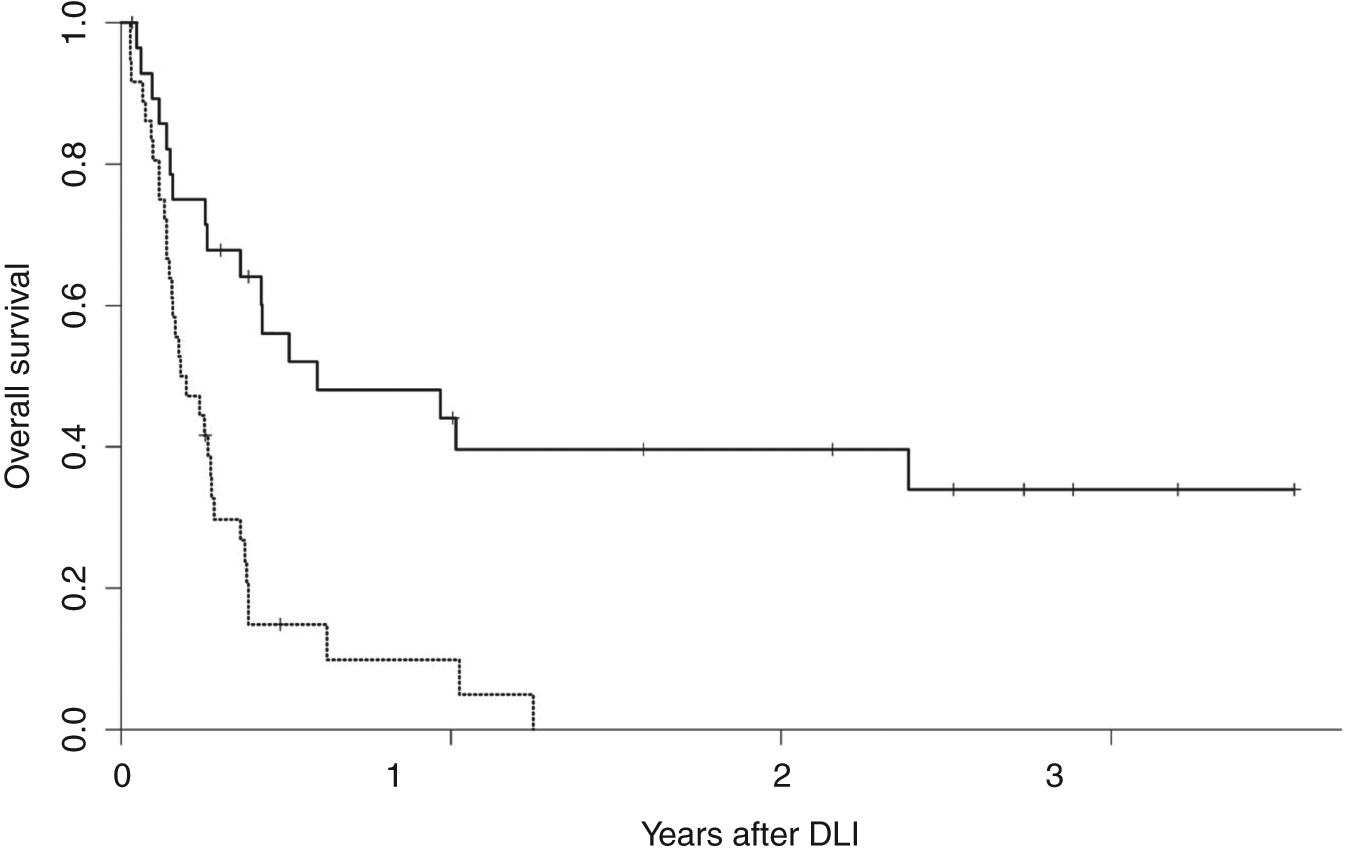
Overall survival after donor leukocyte infusion for relapsed acute myelogenous leukemia following allogeneic hematopoietic stem-cell transplantation (HSCT). Dashed lines, overall survival following relapse within 6 months of HSCT; solid lines, overall survival following relapse beyond 6 months after HSCT. (Reprinted with permission from Levine et al. [2002]).
Most studies on relapse therapy for AML have included only small numbers of patients. However, the European Group for Blood and Marrow Transplantation (EBMT) recently retrospectively analyzed the outcomes of nearly 400 patients with AML, comparing patients who did and did not receive DLI for treatment of relapsed disease following allogeneic HSCT [Schmid et al. 2007]. An improved outcome was seen in those patients who had received DLI (21% overall survival at 2 years) compared with those who did not (9% overall survival at 2 years). In multivariate analysis, factors associated with improved survival in DLI recipients were a lower tumor burden at relapse (<35% bone marrow blasts), remission at time of DLI, favorable cytogenetics, and female sex. Comparing patients who were in remission at the time of DLI or those with favorable cytogenetics with patients with aplasia or active disease at the time of DLI revealed a dramatic difference in 2-year overall survival: 56% versus 9–21%, respectively (Figure 2). It is not clear if this survival benefit represents selection of patients most likely to respond to DLI or if reducing the disease burden of leukemic cells improves the success of DLI; however, it does highlight that DLI can be successful in a select group of patients with AML. Manipulations of DLI are needed to improve its efficacy, together with other new treatment strategies, particularly for high-risk patients.
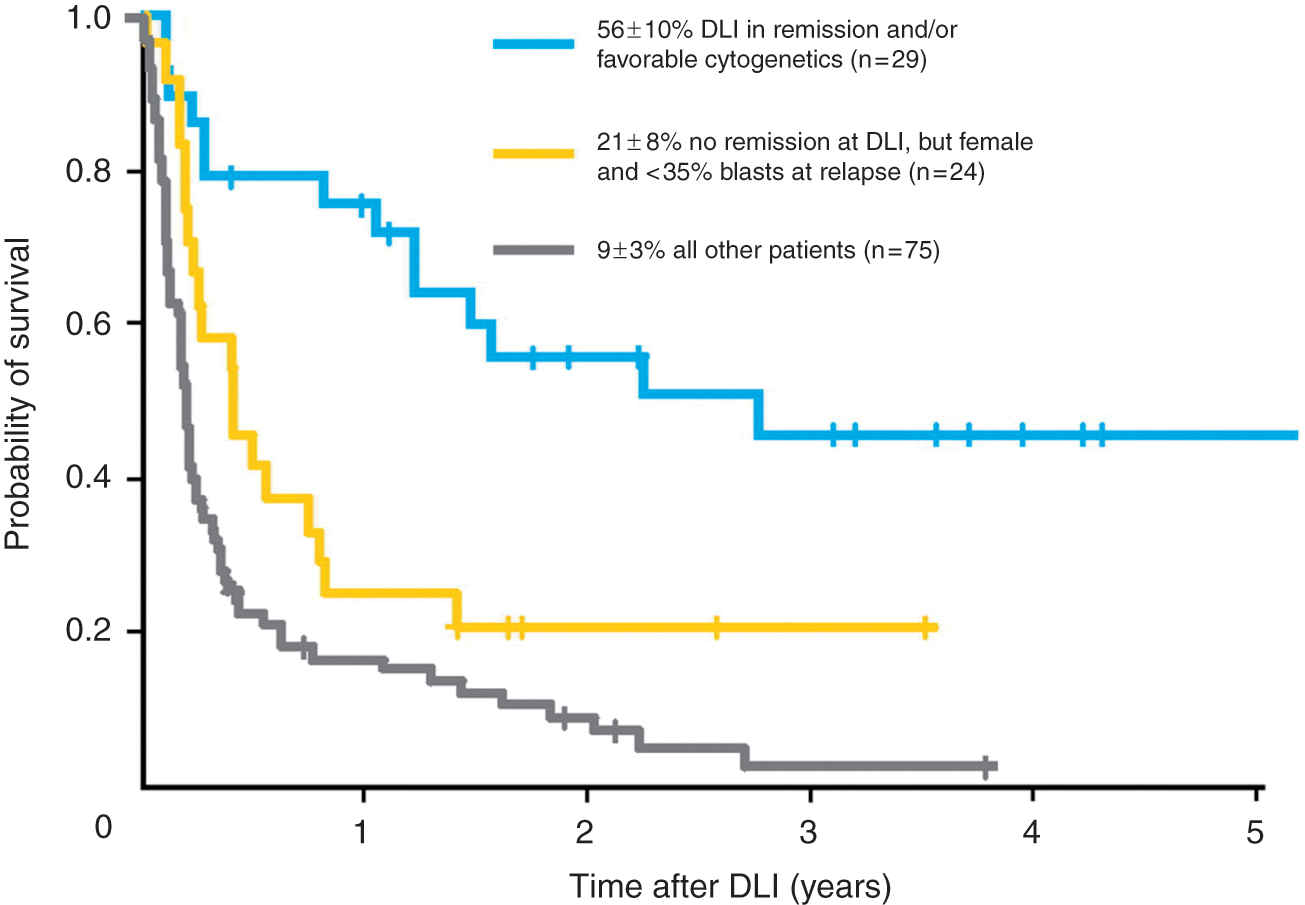
Overall survival in patients with different risk factors for relapse who received donor leukocyte infusion (DLI). (Reprinted with permission from Schmid et al. [2007]).
Experience with DLI for myelodysplasia (MDS) is curiously limited given the increasing number of transplants for MDS. In several series that included only a small number of patients, response to DLI ranged between 14 and 25% (Table 1) [Campregher et al. 2007; Collins et al. 1997; Depil et al. 2004; Kolb et al. 1995]. Response is likely to vary according to how advanced MDS is at the time of relapse. Many reports combine outcomes of patients with MDS with those of AML, and it is important to note that MDS is a heterogeneous disease, making these data difficult to interpret. Further risk stratification and tailored approaches are necessary for this approach to be broadly applicable in MDS. Furthermore, the availability of new treatments for MDS raises the possibility of combination therapy, such as DLI with a methyltransferase inhibitor [Lubbert et al. 2010].
Response rates to donor leukocyte infusion in myelodysplasia; selected studies.
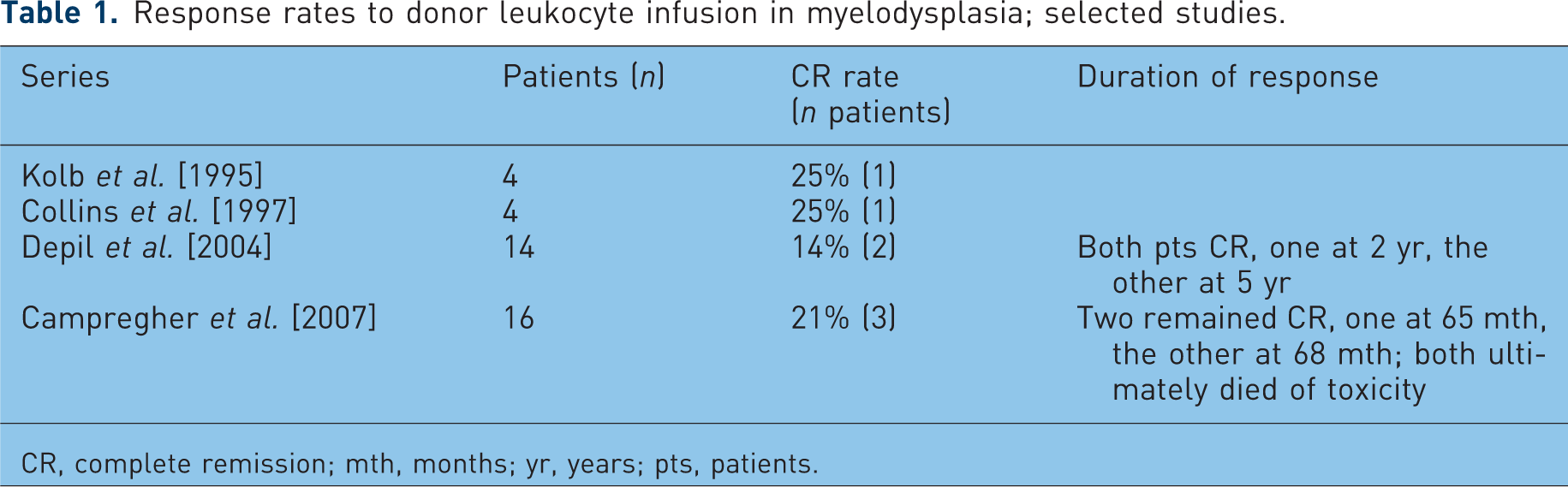
CR, complete remission; mth, months; yr, years; pts, patients.
Despite the fact that one of the first reports of successful DLI was for acute lymphoblastic leukemia (ALL) [Slavin et al. 2002], relapsed ALL has been notoriously refractory to treatment with DLI [Porter et al. 2011]. In patients with ALL treated with DLI alone 0–18% achieved CR, with median survival of 156 days [Collins et al. 1997; Kolb et al. 1995]. In a retrospective study specific to ALL, 3-year overall survival was 13%. Two of 13 patients treated with DLI alone attained CR, as did 5 of 25 (20%) given DLI in a chemotherapy-induced nadir. Only three patients achieved durable remission, remaining in CR for longer than 1 year [Collins et al. 2000]. A small, 10-patient prospective trial for relapsed ALL used cytoreductive therapy before DLI and also showed limited survival; although seven patients achieved a CR, only one a had durable response, remaining alive and in CR beyond 2 years [Choi et al. 2005].
These findings reveal relapsed ALL to be relatively resistant to DLI, but with a compelling and long-lasting GVL effect in certain patients. Some data suggest that DLI is more effective in children with relapsed ALL [Bader et al. 1999] and when used in the setting of minimal residual disease (MRD) [Pulsipher et al. 2009; Bader et al. 2004]. Combining DLI with TKIs for post-transplantation relapse of Philadelphia chromosome-positive ALL may also be a successful approach in certain patients [Tiribelli et al. 2009]. How to define those patients for whom DLI will be successful remains an important but unanswered question, and developing effective approaches for relapsed ALL needs to be a major research initiative.
Multiple myeloma
There is an important graft-versus-myeloma (GVM) effect associated with allogeneic HSCT [Badros et al. 2001; Bjorkstrand et al. 1996; Bruno et al. 2007]. The GVM effect was first directly demonstrated in a patient with relapsed multiple myeloma after allogeneic HSCT who was brought to a durable CR with DLI [Tricot et al. 1996]. Unfortunately, larger studies examining the use of DLI for relapsed multiple myeloma have shown variable success. Of 27 relapsed patients who were treated with DLI (13 of whom received induction chemotherapy), 8 achieved a partial response (PR) and six a CR, for total response rate of 52%. Unfortunately, only five patients (18%) were still in remission after 30 months [Lokhorst et al. 2000]. One multicenter analysis yielded even less encouraging data, with only 2 of 22 patients with multiple myeloma achieving CR with DLI alone. An additional three patients who received pre-DLI chemotherapy each had CR lasting 1–5 months, although the role of chemotherapy in these responses is unclear [Salama et al. 2000].
When used for relapse after nonmyeloablative allogeneic HSCT, DLI (given with induction chemotherapy in 12 of 63 patients) induced CR in 19% of patients and PR in 19%. Those patients with CR had a progression-free survival of 27.8 months, again suggesting that responses to DLI may be durable at least in a subset of patients [Van de Donk et al. 2006]. Immunomodulatory agents used in the treatment of multiple myeloma, such as thalidomide and lenalidomide, have been combined with DLI in the hope of enhancing its immune effect. These agents are thought to increase T-cell and natural killer (NK)-cell activation [Davies et al. 2001]. In 18 patients treated with thalidomide followed by DLI for progressive or residual disease after allogeneic transplantation, 67% responded, with 22% attaining CR [Kroger et al. 2004]. There is also interest in combining DLI with bortezomib on the basis of data suggesting that proteasome inhibition with bortezomib can provide a direct antitumor effect, inhibit alloreactive T cells, and promote myeloma cell killing [Kroger et al. 2004]. Bortezomib can be given safely after allogeneic HSCT [El-Cheikh et al. 2008]; whether a combination of bortezomib and DLI provides improved activity beyond each individual therapy remains to be determined. However, taken together, these results suggest that DLI can create a meaningful GVM effect in some patients, possibly improved by chemotherapy or immunomodulatory drugs, but toxicity and durability remain important concerns.
Non-Hodgkin’s lymphoma, chronic lymphocytic leukemia, and Hodgkin’s lymphoma
Compelling indirect evidence also supports the existence of a graft-versus-lymphoma effect [Ratanatharathorn et al. 1994; Jones et al. 1991], but few studies have examined the role DLI in relapsed lymphoma. Although no responses were seen in initial reports for non-Hodgkin’s lymphoma (NHL) [Collins et al. 1997], the EBMT reported that 6 of 14 patients responded to DLI for relapsed lymphoma [Robinson et al. 2002]. Response rates in other studies, where DLI was often given following T-cell-depleted grafts, vary between 53% and 85% [Porter et al. 2011; Thomson et al. 2010; Bishop et al. 2008; Bloor et al. 2008; Russell et al. 2005, 1996; Mandigers et al. 2003; Marks et al. 2002] (Table 2). Interestingly, in one recent study, 13 of 82 patients relapsed with follicular lymphoma after reduced-intensity conditioned allogeneic HSCT and were treated with DLI; 10 of the 13 patients achieved CR, with nine sustained responses at a median of 44 months, suggesting follicular lymphoma is a potent target for GVL induction [Thomson et al. 2010]. DLI has also been combined with rituximab in a pilot study designed to prevent relapse after reduced-intensity HSCT, and was found to be both safe and effective [Cavattoni et al. 2010]. In the future there may be a role for DLI combined with other monoclonal antibodies with multiple specificities.
Response rates to donor leukocyte infusion in non-Hodgkin’s lymphoma; selected studies.

CR, complete remission; DLI, donor leukocyte infusion; HSCT, allogeneic hematopoietic stem-cell transplantation; mth, months; PR, partial response; pts, patients; RIC, reduced intensity conditioning.
Compelling evidence also suggests an important GVL effect for chronic lymphocytic leukemia (CLL). For instance, both the long-term disease control that has been attained through nonmyeloablative transplantation [Sorror et al. 2008] and the kinetics of disease response following withdrawal of immunosuppression [Ritgen et al. 2004] demonstrate GVL activity in CLL. However, the number of patients treated with DLI for CLL remains small. Response rates vary widely, from 12% to 90%, as summarized in Table 3 [Bloor et al. 2008; Hoogendoorn et al. 2007; Delgado et al. 2006; Russell et al. 2005; Sorror et al. 2005; Khouri et al. 2004; Ritgen et al. 2004; Schetelig et al. 2003; Marks et al. 2002]. These dramatically different response rates are representative of the small sample sizes, diversity of indications for DLI, disease status at the time of infusion, and the use of chemotherapy or monoclonal antibodies with DLI, but support a meaningful response to cellular immune therapy.
Response rates to donor leukocyte infusion in chronic lymphocytic leukemia; selected studies.

CR, complete remission; DLI, donor leukocyte infusion; HSCT, allogeneic hematopoietic stem-cell transplantation; IgH RQ-PCR, immunoglobulin heavy chain real-time quantitative polymerase chain reaction; MRD, minimal residual disease; PR, partial response; pts, patients.
Although Hodgkin’s lymphoma is also susceptible to an important allogeneic graft-versus-lymphoma effect [Porter et al. 2003], most reports of DLI for relapsed Hodgkin’s lymphoma following allogeneic HSCT include only small numbers of patients. Response rates to DLI in these patients have ranged from 15% to 75% [Peggs et al. 2009, 2007, 2005; Armand et al. 2008; Anderlini and Champlin, 2006]. Many responses are durable, however, and while DLI for relapsed Hodgkin’s disease requires further study and optimization, it probably offers the only chance and meaningful disease control for relapse after allogeneic HSCT.
Donor leukocyte infusion from unrelated donors
Most studies of DLI after allogeneic HSCT include recipients of both related and unrelated donor cells. There has been concern that outcomes after unrelated donor DLI (U-DLI) may be different from those after DLI from a matched sibling. For instance, given the increased frequency of minor histocompatibility differences, there may be a higher risk of GVHD. However, it is not known if this might translate into enhanced GVL activity. Therefore it is important to consider recipients of U-DLI separately from recipients of matched sibling DLI. In addition, U-DLI is being used with increasing frequency with the increasing use of unrelated donor HSCT. Direct comparisons between sibling DLI and U-DLI are limited given the small number of cases, the frequently short follow-up period, and the use of both related and unrelated donors in many trials. In early retrospective data, outcomes appear similar to those with sibling donors, although the numbers of patients analyzed were small [Collins et al. 1997; Kolb et al. 1995]. One large retrospective analysis described 58 recipients of U-DLI identified by the National Marrow Donor Program. For those being treated with U-DLI for active disease, CR was attained in 46% of patients with CML, 42% of those with AML, and two of the four with ALL. Similar to large series of related DLI, grade II–IV acute GVHD occurred in 25% of treated patients and chronic GVHD occurred in 41% [Porter et al. 2000]. Another report of patients with CML compared related DLI with U-DLI, and found similar rates of cytogenetic remission (73% and 64%, respectively, p = 0.71). Although the rate of chronic GVHD was similar there was a trend towards more grade II–IV acute GVHD after U-DLI (58%) than after related DLI (39%), which did not reach statistical significance (p = 0.09) [Van Rhee et al. 1998].
These results imply that U-DLI is similar to related DLI and is an appropriate therapy in the setting of relapse following unrelated HSCT. In addition, there is no conclusive evidence suggesting higher toxicity or more potent GVL using U-DLI compared with sibling DLI. Therefore currently available evidence suggests that the dose of donor T cells needed to induce GVL should be similar, regardless of the donor source.
Treatment of nonrelapse complications
The administration of donor T cells can not only induce a potent GVL response but may also be useful in restoring cell-mediated immunity, which is critical to treat nonrelapse complications after transplantation. The best example is the use of DLI to treat post-transplantation Epstein–Barr virus (EBV)-associated B-cell lymphoproliferative disorder (PTLD). PTLD occurs in the setting of unrestrained EBV-driven proliferation of B cells in the absence of effective T-cell regulation; it is more common after using T-cell-depleted grafts and is most often donor derived [Loren et al. 2003; Zutter et al. 1988]. PTLD previously carried a dismal prognosis after allogeneic HSCT [Shapiro et al. 1988]. As withdrawal of immune suppression may be effective for PTLD it was logical to assume that restoring cell-mediated immunity with donor lymphocytes would directly treat PTLD. In fact, DLI has been shown to induce durable responses in most patients with PTLD after allogeneic SCT [Heslop et al. 2010; Papadopoulos et al. 1994; Porter et al. 1994a]. Between the high response rates using DLI, and the availability of rituximab, PTLD is no longer the lethal complication previously described.
DLI for PTLD is still associated with significant toxicity from GVHD. Several investigators have generated and expanded EBV-specific T cells as durable prophylaxis and treatment for EBV-related PTLD after allogeneic HSCT [Heslop et al. 2010; Gustafsson et al. 2000; Rooney et al. 1998]. This exciting work demonstrates that virus-specific (and maybe tumor-specific) T cells can be manufactured and be effective with limited GVHD and other toxicity [Melenhorst et al. 2010].
The impaired viral immunity after transplantation can lead to other life-threatening viral infections; respiratory syncytial virus [Kishi et al. 2000] and adenoviral [Leen et al. 2009; Hromas et al. 1994] infections have been successfully treated with DLI. DLI has also been used to transfer cytomegalovirus (CMV) immunity and prevent viral reactivation with CMV-specific T cells cloned from CMV-seropositive marrow donors [Walter et al. 1995; Riddell et al. 1992], and successfully treat CMV infections unresponsive to antiviral therapy [Peggs et al. 2003; Einsele et al. 2002]. These examples demonstrate the diversity of applications for DLI in the transfer of immunity from donor to host, and its ability to provide not only tumor-directed immunity but also immune responses to common infections seen after HSCT [Fujita et al. 2008].
Toxicity of donor leukocyte infusion
Successful DLI for relapse after HSCT continues to be limited by toxicity from GVHD and marrow aplasia. Both acute and chronic GVHD are common complications of DLI, occurring in 40–60% of patients [Porter and Levine, 2006]. Nevertheless, despite the relatively high dose of cells used in DLI, and lack of GVHD prophylaxis in most cases, the rate of severe acute GVHD (grade III–IV) is only 15–35%, with associated treatment-related mortality of 4–15% (reviewed by Frey and Porter [2008]). Chronic GVHD occurs in 30–60% of DLI recipients. Most initial studies found that occurrence of both acute and chronic GVHD was associated with GVL activity, although a small but significant number of patients had no GVHD and still attained CR [Collins et al. 1997; Kolb et al. 1995].
To limit GVHD while maintaining GVL, Mackinnon and colleagues used low doses of cells as initial DLI for relapsed CML, and then escalated doses until a disease response was seen [Mackinnon et al. 1995]. This approach led to very little acute GVHD. The incidence of chronic GVHD remained significant, although it was associated with continued CRs. The relative safety of this dose escalation strategy has been confirmed by additional studies [Dazzi et al. 2000; Guglielmi et al. 2002; Peggs et al. 2009; Thomson et al. 2010] and can be expected to minimize the toxicity at least of acute GVHD for patients with indolent relapses.
Pancytopenia may occur after DLI [Collins et al. 1997; Kolb et al. 1995], sometimes necessitating the need for transfusions or leading to infectious complications from neutropenia. Typically, pancytopenia reverses without therapy, although sustained marrow aplasia can occur in occasional patients, similar to transfusion-associated GVHD (TA-GVHD) [Anderson and Weinstein, 1990]. Lack of residual donor chimerism can predict aplasia following DLI [Chiorean et al. 2004; Keil et al. 1997]. In some cases marrow aplasia is due to the destruction of host hematopoiesis before or without recovery of residual donor hematopoiesis, and may be the reason pancytopenia is noted frequently after DLI for chronic phase CML [Kolb et al. 1995]. Sustained marrow aplasia may be reversed with the infusion of additional donor stem cells in some patients [Drobyski et al. 1993; Porter et al. 1994b]. Use of G-CSF-stimulated peripheral blood mononuclear cells as the source of DLI has limited the duration of neutropenia and may protect against persistent aplasia [Levine et al. 2002]. Although marrow aplasia and GVHD are significant toxicities, they are often acceptable when compared with the limited success of alternative therapies for relapsed disease following allogeneic transplantation.
Emerging strategies to enhance donor leukocyte infusion
Since the initial success of DLI to treat CML, many efforts have been made to improve the activity of DLI, particularly for diseases less susceptible to GVL induction. Numerous strategies to enhance DLI therapy have been aimed at minimizing GVHD without losing the GVL effect; others have attempted to strengthen the GVL effect by manipulating the donor product.
Reducing graft-versus-host disease
In order to facilitate the GVL effect, DLI is typically given without prophylactic immunosuppression. In patients at high risk of GHVD, such those who receive DLI from haploidentical donors, GVHD prophylaxis has been used. In a retrospective analysis GVHD prophylaxis after haploidentical DLI was found to significantly reduce the incidence of grade III–IV acute GVHD without altering complete remission rates [Huang et al. 2007]. Data on GVHD prophylaxis following DLI from human leukocyte antigen (HLA)-matched donors from the same institution has also been retrospectively described. In 48 of 70 patients who received more than 2 weeks of immunosuppression (cyclosporin or weekly methotrexate) following DLI for either relapse or prophylaxis only 7% developed acute GVHD, compared with 50% of those with no or less than 2 weeks of immunosuppression. Rates of chronic GVHD and relapse were not significantly different in this trial [Huang et al. 2009], but the heterogeneous patient population and retrospective analysis make these data difficult to interpret. Immunosuppression with DLI for patients at high risk of severe GVHD may be a reasonable approach to reduce toxicity of this therapy but may attenuate GVL responses [Imado et al. 2004].
An alternative approach to reduce GVHD has been to lower the dose of donor lymphocytes for the initial infusion and then escalate the dose of cells until complete remission is attained. This approach is based on the assumption that there is a T-cell dose at which GVL is possible but GVHD is not clinically apparent, dependent on an unknown and theoretical effector:target-cell ratio. One study using this strategy in patients with CML resulted in complete remissions in 86% of patients, with minimal acute GVHD [Mackinnon et al. 1995]. A subsequent large retrospective analysis confirmed that a lower initial cell dose reduced GVHD and improved survival [Guglielmi et al. 2002]. This approach also showed that lower doses of cells are required to induce remission in patients with a minimal disease burden, supporting the importance of an effector:target ratio [Mackinnon et al. 1995]. Interestingly this also leads to less GVHD, even in patients eventually receiving higher cumulative doses of cells. This strategy may result in delayed GVL activity and hence is best reserved for indolent malignancies, as the proliferation rate of acute leukemia may be too rapid to tolerate lower doses of cells early in the treatment course.
A more specific method to limit GVHD involves infusion of donor lymphocytes genetically modified with a suicide gene. The herpes simplex virus thymidine kinase (HSV-TK) gene may be transfected into donor cells, making them sensitive to ganciclovir. These cells have been active for PTLD and in those patients that developed GVHD ganciclovir dramatically reduced the number of HSV-TK transfected cells and effectively controlled GVHD [Bonini et al. 1997]. A phase 1–2 study of transfected HSV-TK donor cells following haploidentical HSCT led to successful control of GVHD through induction of the suicide gene in all 10 recipients who developed acute GVHD, while allowing successful immune reconstitution in 22 of 28 treated patients [Ciceri et al. 2009]. Unfortunately, immune responses to transfected cells lead to rapid disappearance of the modified cells [Berger et al. 2006]. Although this technology shows promise for many post-HSCT problems, current methods are technically difficult and time intensive, thus limiting the applicability of this approach for now.
Another method to limit GVHD after DLI would be to deplete GVHD-inducing cells. CD8+ T cells have been implicated in GVHD, and depletion of CD8+ cells in the donor transplant grafts has been associated with less GVHD than in those receiving unmodified grafts, while still retaining GVL effects [Nimer et al. 1994]. In one trial of CD8+ depleted DLI given for relapsed hematologic malignancies, 21 of 37 patients had a CR and nearly 50% of the responding patients had no evidence of GVHD [Alyea et al. 1998]. The use of CD8+ T-cell-depleted DLI for early phase CML also induces durable CRs [Shimoni et al. 2001]. Emerging data from mouse models have demonstrated that the naïve subset of CD8+ T cells leads to more significant GVHD, while the effector memory subsets (TEM) of CD8+ and CD4+ T cells maintain the GVL effect without causing GVHD [Chen et al. 2007; Beilhack et al. 2005; Chen et al. 2004; Zhang et al. 2004; Anderson et al. 2003]. Clinical trials using selected donor TEM cells to treat relapse after allogeneic HSCT are now appropriate and the results will be of great interest [Van den Brink et al. 2010].
Regulatory T cells (Treg) may be promising for controlling GVHD while maintaining activity against tumor cells [Edinger et al. 2003]. A recent study in humans has demonstrated that by altering the conditioning regimen of allogeneic HSCT to favor proliferation of regulatory natural killer T cells (NKT), minimal GVHD (acute GVHD 2–10% and chronic GVHD 26–28%) developed while GVL was maintained [Kohrt et al. 2009], in theory related to a sustained Treg population supported by NKT cells [Pillai et al. 2009]. In the setting of relapse after allogeneic HSCT, delivery of increased numbers of Treg is feasible through the use of low-dose interleukin 2 (IL-2) given with DLI. This regimen used in a small number of patients produced increased numbers of Treg compared with patients who received DLI or IL-2 alone. No patient receiving both DLI and IL-2 developed GVHD [Zorn et al. 2009]. Brunstein and colleagues demonstrated the safety of Treg infusions following double cord blood transplants derived from a third umbilical cord blood source in a recent phase 1 trial. A total of 23 patients received 1–30 × 105/kg Treg at day +1 and, in a smaller subset of patients, at day +15. The rate of grade II–IV acute GVHD was 43%, compared with 61% in their historic controls [Brunstein et al. 2011]. Clinical trials administering Treg for patients receiving allogeneic HSCT are ongoing [Van den Brink et al. 2010].
Enhancing the graft-versus-leukemia effect
Many efforts have attempted to enhance the GVL effect of cellular therapies. Isolation and expansion of functional leukemia-reactive T cells may be the most direct way to induce GVL without GVHD. Early studies showed that it is feasible to isolate cytotoxic T cells (CTL) that demonstrate in vitro antileukemic activity and use them successfully for relapsed leukemia [Falkenburg et al. 1999; Marijt et al. 2007].
In most cases, tumor-specific target antigens have not been identified, limiting the ability to generate specific cellular immunotherapy. Potential targets for GVL induction include minor histocompatibility antigens (mHAgs) differentially expressed on hematopoietic cells [Voogt et al. 1988] and leukemia-specific antigens [Bocchia et al. 1996; Clark et al. 2001]. T cells against mismatched mHAgs that demonstrate activity in vitro against leukemic cells have been created [Marijt et al. 2003; Mutis et al. 1999]. In a recent study, patients with relapsed acute leukemia after allogeneic HCST received infusions of CD8+T-cell clones recognizing mHAgs on recipient hematopoietic cells but not recipient dermal fibroblasts [Warren et al. 2010]. Four of six patients achieved a CR, including three patients with disease refractory to chemotherapy. Although these remissions were not durable and were accompanied by unanticipated pulmonary toxicity in some patients, these findings highlight the feasibility and potential power of carefully selected tumor-specific immunotherapy. Continued challenges include the avoidance of off-target toxicity, the emergence of antigen-loss variants and limited persistence of adoptively transferred cells.
In some cases, potential tumor-associated antigens may be normal cellular antigens that are overexpressed. Proteinase 3 (PR3) is overexpressed in myeloid leukemic cells, and vaccination with the PR1 epitope of PR3 has shown considerable antileukemic activity [Molldrem, 2006; Rezvani et al. 2008]. Wilms’ tumor protein (WT1) is overexpressed on myeloid malignancy cells as well [Rosenfeld et al. 2003], and could serve as a potential target for vaccination strategies or the generation and expansion of tumor-specific DLI products [Keilholz et al. 2009]. Additional antigens considered as targets for immunotherapy have included BCR/ABL [Clark et al. 2001], NY-ESO-1, a cancer–testis antigen commonly expressed on myeloma cells [Atanackovic et al. 2007], and PRAME, an HLA-24-restricted antigen on AML cells [Greiner et al. 2006]. Further specification of CTLs to tumor cells is now being studied with genetically engineered cells with chimeric antigen receptors. Cells have been developed that demonstrate potent and persistent antileukemic properties in murine models [Milone et al. 2009], and hold potential for successful durable responses in humans.
Although feasible, the generation of tumor-specific CTL has proven time consuming and often difficult. An alternative strategy to enhance GVL activity is to use nonspecific ex vivo donor T-cell activation and expansion. Donor T cells may not be appropriately activated in vivo to induce an antitumor response, perhaps as a result of Treg, suppressive cytokines, lack of host antigen-presenting cells to present antigen, lack of costimulatory ligands on tumor cells, insufficient numbers of cytotoxic effector cells, or through other poorly defined mechanisms. To overcome many of these obstacles, T cells can be expanded ex vivo through costimulation in a physiologically appropriate manner by exposure to magnetic beads coated with anti-CD3 and anti-CD28 [Liebowitz et al. 1998; Levine et al. 1997]. In a phase 1 trial, conventional DLI was followed by escalating doses of ex vivo costimulated donor T cells (known as activated DLI or aDLI) in 18 patients with relapsed advanced hematologic malignancies after allogeneic SCT [Porter et al. 2006]. Eight of 17 evaluable patients achieved a CR, including two of four patients with AML, four of seven patients with ALL, and each patient with CLL and NHL (mantle-cell lymphoma). Activated DLI did not result in excessive toxicity: five patients developed grade I–II acute GVHD, two developed grade III acute GVHD, and four developed chronic GVHD. No patient died of complications related to GVHD. Overall, the response rates were impressive in diseases that historically have not responded well to unmanipulated DLI, suggesting that aDLI may offer an advantage for GVL induction. Future studies with aDLI will include further dose escalation, repetitive dosing of aDLI to minimize late recurrences, and attempts at activation and expansion of tumor-specific T cells.
It may also be possible to enhance the antitumor effects of cells other than donor T cells. NK cells have demonstrated potent antitumor activity, and a number of trials have demonstrated the safety and feasibility NK donor cell infusions after haploidentical HSCT [Koehl et al. 2005; Passweg et al. 2004]. Mesenchymal stromal cells (MSC) obtained from donor sources are being used successfully to treat steroid-refractory GVHD following HSCT [Le Blanc et al. 2008]. Building on these and other novel cellular strategies to enhance antitumor immune responses and modulate immune complications of transplantation should improve the safety, specificity, and success of cellular therapy following allogeneic HSCT.
Prophylactic donor leukocyte infusion
It is clear that DLI is often more successful if it is given to patients with MRD, suggesting there may be an important effector:target ratio. This suggests that DLI could be useful in the setting of MRD rather than at florid relapse. One major issue is how best to detect MRD and how to determine the clinical significance of early detection with high sensitivity methods [Kroger et al. 2010]. Numerous methods used to monitor MRD include multiparameter flow cytometry [Baer et al. 2001; Rawstron et al. 2007], real-time quantitative PCR for evidence of mixed chimerism or disease-specific markers, cytogenetics, fluorescence in situ hybridization, high-sensitivity chromosome analyses, and imaging studies (CT, PET, MRI, etc.) for tumor recurrence. The sensitivity of detection of course depends on the molecular method used. Furthermore, finding evidence of MRD with different methods may have different implications. In addition, how relapse is defined on the basis of MRD testing will have major implications for patient care, data interpretation, and future clinical trial design. A detailed review of MRD monitoring, the definition of relapse, and the clinical implications is beyond the scope of this review but has recently been reviewed in detail [Kroger et al. 2010]. Further studies to define the preferred method, optimal timing and frequency of MRD assessment, and the risk of relapse based on MRD data are necessary to determine the best use of DLI before hematologic relapse.
In CML, treating patients in early molecular relapse (defined by PCR techniques detecting recurrent BCR/ABL transcripts) with DLI has been extremely successful [Raiola et al. 2003; Mackinnon et al. 1995]. The use of PCR to detect early relapse of other diseases is much more difficult since most diseases do not express unique chimeric genes that can be targeted by PCR analysis. One example of a disease where PCR monitoring for relapse may be most successful is acute promyelocytic leukemia, where detecting recurrence of the RARa/PML transcript often heralds relapse [Gallagher et al. 2003].
Mixed chimerism is an emerging marker for residual disease and impending relapse in CML [Roth et al. 1990] and ALL, serving as a possible trigger for early use of DLI [Pulsipher et al. 2009; Lutz et al. 2008; Bader et al. 2004]. It is less clear if mixed chimerism is useful to predict relapse in AML and other diseases after transplantation.
Because GVHD is significant after DLI [Frey and Porter, 2008], studies of prophylactic DLI must include a careful assessment of GVHD risk. Timing and dose of DLI are critical. Simply limiting immune suppression after transplantation or adding additional donor T cells at the time of HSCT leads to unacceptable GVHD, at least in patients with advanced malignancies. This suggests that attempts at GVL induction very early in the transplantation course will have limited success [Sullivan et al. 1989a]. Furthermore, giving DLI immediately after lymphodepleting (or cytoreductive) chemotherapy has also led to frequent and severe GVHD, perhaps due to the homeostatic proliferation of T cells that occurs in lymphodepleted states [Miller et al. 2007] or to the proximity of the cytokine-abundant phases that occur after chemotherapy [Johnson et al. 1993; Antin and Ferrara, 1992]. In either case, delaying the administration of donor lymphocytes after transplantation (or after chemotherapy) reduces the severity of GVHD in murine models [Johnson et al. 1993; Slavin et al. 1992], suggesting that prophylactic DLI is feasible if appropriately delayed from transplantation.
Prophylactic DLI may be particularly useful in restoring GVL after T-cell-depleted transplants [Ferra et al. 2001]. T-cell depletion may limit GVHD but leads to a loss of GVL and increases the risk of relapse [Horowitz et al. 1990]. Delayed administration of DLI has been tested and confirms the importance of the timing and dose of donor T cells. In 38 patients transplanted with T-cell-depleted grafts (to prevent GVHD), followed by planned DLI, patients who received a higher dose of T cells on day 30 (1 × 107 CD3+ cells/kg) developed significantly more acute grade II or higher GVHD than those patients receiving a lower dose of T cells at day 30 (2 × 106 CD3+ cells/kg) followed by a second dose at day 45 (5 × 107 CD3+ cells/kg). In standard-risk patients there was 73% disease-free survival, similar to that seen in T-cell-replete transplants, indicating that GVL could be restored with DLI [Barrett et al. 1998]. Other studies have used planned DLI following T-cell-depleted transplants for patients with multiple myeloma. In one study, 14 patients were treated with DLI (1–3 × 107 CD4+ cells/kg) at 6–9 months following T-cell-depleted HSCT. Of the 11 patients with residual disease at the time of DLI, six attained a CR, with many responses still durable at a median of 28 months follow up. Unfortunately, GVHD occurred more commonly than expected, with 50% of patients developing either severe acute or chronic GVHD [Alyea et al. 2001].
We recently completed a trial aimed at restoring GVL activity with ex vivo costimulated (anti-CD3/CD28) DLI given as prophylaxis following in vivo T-cell-depleted (using alemtuzumab) allogeneic HSCT. Two planned doses were given at 4 months (1 × 107 CD3+ cells/kg) and 6 months (1 × 108 CD3+ cells/kg) post HSCT, and preliminary results show this was safe, with minimal acute GVHD [Goldstein et al. 2009]. Prophylactic DLI following T-cell-replete HLA-matched transplants has been studied as well. Sohn and colleagues treated 7 of 17 patients with advanced hematologic malignancies with prophylactic DLI 40–120 days following transplantation at 3.0–9.9 × 107 CD3+ cells/kg; 10 additional patients on the trial could not be treated because of death, relapse, or severe GVHD. Four of the seven treated patients remained alive and free of disease at a median of 597 days posttransplantation, although all with chronic GVHD [Sohn et al. 2002]. Together, these results suggest that although further work is needed to clarify the safest dose and timing, planned DLI may prevent relapse in carefully selected high-risk patients.
Conclusion
The GVL effect is critical to the success of allogeneic HSCT for hematologic malignancies. GVL induction with DLI after allogeneic transplantation is commonly used to treat relapsed disease. While effective and reliable in chronic phase CML, other diseases have shown limited responses to DLI. Predictors of response include not only type of disease, but also the extent of disease, pace of progression, and time to relapse among other factors, highlighting the need for a better understanding of disease-specific relapse and the need for earlier and more potent therapies.
Manipulations of immune effector cells to minimize GVHD and promote GVL are necessary to create more effective approaches for relapse. Numerous strategies are being tested to enhance specificity, maximize GVL, and minimize GVHD after adoptive immunotherapy. A better understanding of these effector cells and target antigens for GVL induction is clearly necessary. In addition, there is an immediate need to better study the epidemiology and natural history of relapse [Pavletic et al. 2010]. As most immune therapy is more successful in cases of MRD, better definitions of relapse, and the systematic study of prophylactic DLI may help design strategies to avoid relapse altogether. Progress in the therapeutic development of cellular immunotherapy will require carefully designed controlled trials and likely will require multinational collaborations [Porter et al. 2011]. Above all, a better understanding of factors that both guide and prevent immune response to tumor cells and efficient methods to harness this activity are necessary.
Footnotes
This work was supported in part by grants from the Leukemia & Lymphoma Society (7000-02) and NIH (K24 CA11787901) (DLP).
The authors declare no conflicts of interest in preparing this article.