
Abstract
Myelofibrosis (MF) is a chronic myeloid neoplasm characterized by either primary myelofibrosis, or secondary MF following essential thrombocythemia or polycythemia vera. Historically, therapy has been symptom directed; however, in 2011, the first janus kinase inhibitor (JAK-i) – ruxolitinib – was approved for treatment. This medication was found to be effective in reduction of symptom burden and spleen size; however, the median duration of response is about 3 years. In addition, many patients are intolerant or develop toxicities to ruxolitinib, including patients with anemia, as well as thrombocytopenia. Therefore, there is a critical need for alternate therapeutic options for patients with MF. Additional JAK-i have been developed over the last 8 years, including fedratinib, momelotinib, and pacritinib. Fedratinib recently received approval for treatment of MF both in the first-line and second-line setting. It has shown efficacy in the first-line setting, as well as in 30% of patients who are refractory/intolerant of ruxolitinib. This review covers the trials that have led to the approval of ruxolitinib as well as fedratinib, as well as reviews of two JAK inhibitors that are still under clinical investigation: momelotinib and pacritinib.
Keywords
Background
Myelofibrosis (MF) is a chronic myeloid neoplasm characterized by anemia, debilitating constitutional symptoms, and splenomegaly.1–3 In the United States (US), approximately 20,000 patients are afflicted with myelofibrosis MF. MF can be de novo, or primary MF (PMF), or secondary following essential thrombocythemia (post-ET MF) or polycythemia vera (post-PV MF).
Treatment for MF historically [prior to the advent of janus kinase inhibitor (JAK) inhibition] included such drugs as hydroxyurea, thalidomide, and interferon alpha, and supportive measures such as erythropoietin simulating agents and prednisone. To address splenomegaly, patients often underwent splenectomy, a procedure that carries significant morbidity, or splenic radiation. With the discovery of the pathologic mutation of JAK2 in 2005 (JAK2 V617F), a new class of drugs developed, JAK inhibitors (JAK-i). JAK are a family of protein-tyrosine kinases that are critical in signaling pathways to promote cell growth. The JAK family includes JAK1, JAK2, JAK3, and TYK2 (tyrosine kinase 2). JAK1/2 and TYK2 are found in many cells throughout the body, and JAK3 appears to be confined to hematopoietic cells. In hematopoietic cells, JAK proteins bind to the juxtamembrane region of specific cytokine receptors and are involved in the generation of thousands of proteins involved in cell growth and differentiation. 4
Ruxolitinib: first in class JAK inhibitor
Ruxolitinib, a JAK1/2 inhibitor, was the first drug developed in this class. It was approved for MF in 2011. This latter approval arose from the positive results of two phase III studies in MF: COMFORT1 5 and COMFORT2. 6 In COMFORT1, ruxolitinib was compared with placebo, the primary endpoint of 35% reduction in spleen volume was met in 41.9% of patients, and maintained for 48 weeks in 67% of those patients. 5 Reduction of symptom burden, as measured by MF-SAF 2.0, was observed in 45.9% of patients, and a mean improvement of 41.8% was appreciated in all patients who received ruxolitinib. 5 The COMFORTII study, which compared ruxolitinib with best available therapy (BAT), showed equal success, with 28% of the ruxolitinib-treated patients experiencing at least 35% spleen volume reduction (SVR), or 50% reduction in palpable splenomegaly at 48 weeks. 6 Myeloproliferative neoplasm (MPN)-specific symptoms were was not assessed in this study, but, using EORTC-30 and FACT-Lym, an improvement in quality of life was appreciated.
Ruxolitinib has been a very successful drug impacting splenomegaly, symptoms, and likely improving survival; however, it is not a cure, and the median time of response is 3.2 years. 7 When patients progress through ruxolitinib, the median survival is 14 months, and may be less in the setting of clonal evolution. 8 In addition, many patients are intolerant of ruxolitinib due to side effects. Therefore, there is a critical need for treatments for patients with MF. To address this need, multiple other JAK-i have been developed, two under development are close to approval, and now a second drug is approved – Fedratinib (Inrebic – Celgene).
Fedratinib: approved fall 2019
Fedratinib, a selective JAK2 inhibitor, was initially shown to have a beneficial impact on the spleen and symptom burden in a phase I study. 9 The maximum tolerated dose was found to be 680 mg daily, and was limited by asymptomatic hyper-amylasemia. 9 A favorable spleen response was noted in 39% and 47% at 6 and 12 months, respectively, and many patients appreciated improvement in their symptoms. 9 Of the patients with symptoms, 75% experienced improvement after 1 month, and 50% had complete resolution. Of the 51 patients who harbored a JAK2V617F mutation, 23 (45%) experienced reduction in their allele burden. 9 With these promising results, a phase III trial was initiated. For a summary of the pertinent details of fedratinib studies, JAKARTA-1 and JAKARTA-2, please see Table 1.
Comparison of JAKARTA-1 and JAKARTA-2 studies.
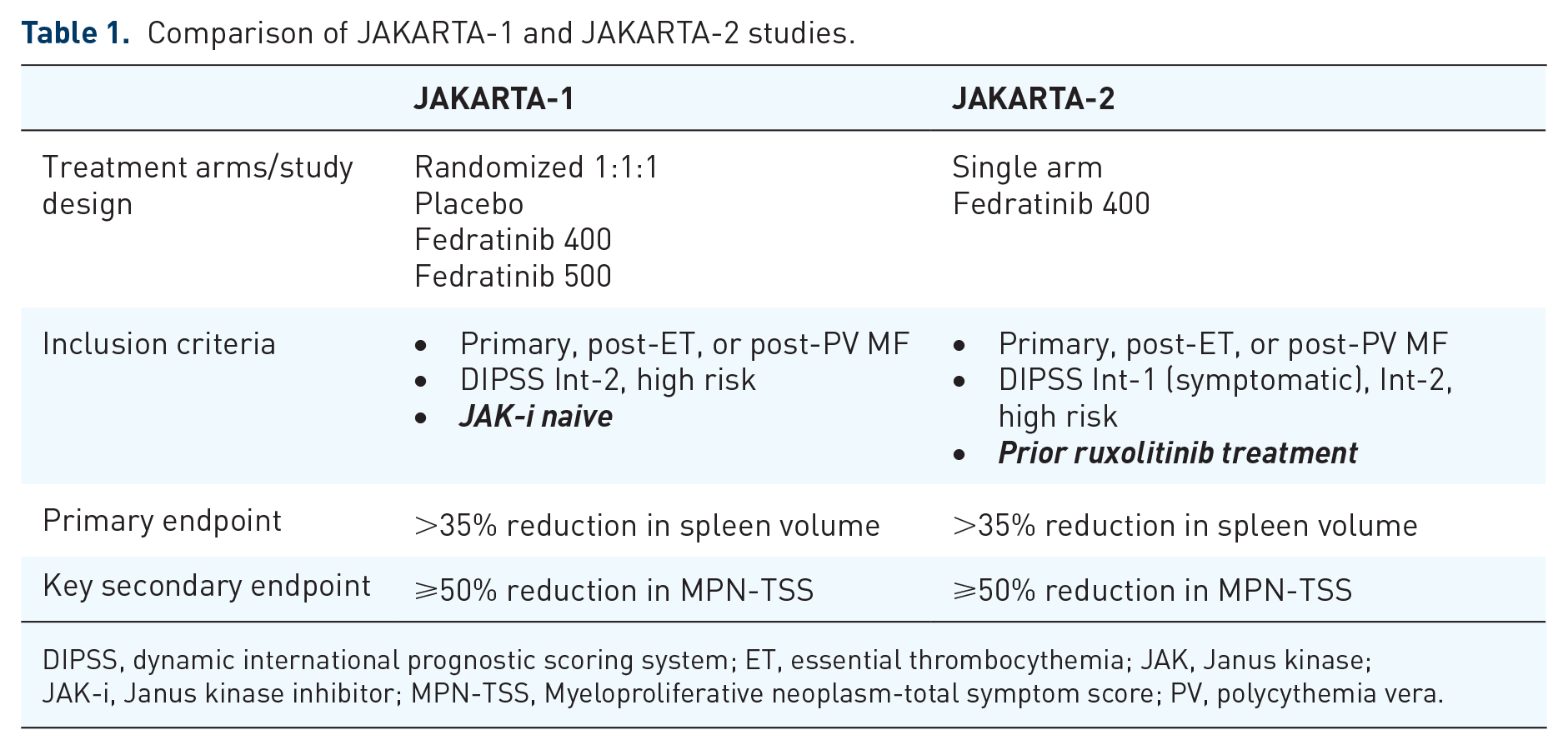
DIPSS, dynamic international prognostic scoring system; ET, essential thrombocythemia; JAK, Janus kinase; JAK-i, Janus kinase inhibitor; MPN-TSS, Myeloproliferative neoplasm-total symptom score; PV, polycythemia vera.
The JAKARTA-1 study was a phase III study conducted in 94 centers worldwide. Patients were randomized to one of three groups: 400 mg daily, 500 mg daily, or placebo. 10 Crossover was allowed after 24 weeks. The primary endpoint was reduction in spleen size by at least 35%, which lasted at least 4 weeks. 10 The secondary endpoint was reduction in symptom burden by 50% based on MPN-symptom assessment form (MPN-SAF) 2.0. A total of 289 patients were enrolled from December 2011 to September 2012, with 96, 97, and 96 patients randomly assigned to fedratinib 400 mg, 500 mg, and placebo, respectively. The spleen response observed at week 24, which was durable 4 weeks later, was in 35 (36%), 39 (40%), and 1 (1%) in the fedratinib 400-mg, 500-mg, and placebo groups, respectively. 10 The symptom response at week 24 was 33 of 91 (36%), 31 of 91 (34%), and 6 of 85 (7%) in the 400-mg, 500-mg, and placebo groups, respectively. Improvement in symptom burden was noted within 4 weeks, and durable until week 24. 10 These responses were irrespective of JAK2 mutation status, disease risk, or MF disease subtype. The most common hematologic toxicity was anemia, which had a nadir at 12–16 weeks. However, after that, many patients experienced an improvement in hemoglobin, and, of the 19 who were transfusion dependent, 15 became transfusion independent. 10 The most common non-hematologic adverse event was gastrointestinal symptoms. 10 Unfortunately, four cases of encephalopathy were noted in the patients who were in the Fedratinib 500 mg arm. 10 These were felt to be consistent with Wernike’s encephalopathy (WE), and the study was discontinued.
JAKARTA-2 was a phase II study conducted simultaneously to JAKARTA-1 to evaluate the efficacy of fedratinib in patients who were intolerant or experienced progression on ruxolitinib. Treatment resistance was defined as failure to respond within 14 days, or progression of disease as reported by the provider. Treatment intolerance was defined as anyone who experienced unacceptable toxicity after being on treatment for at least 14 days. A total of 97 patients were enrolled between 2012 and 2013. In this study, patients were started on 400 mg daily, but could increase to 600 mg daily if they did not experience an adequate response, or be dose reduced to 200 mg daily in the event of toxicity. Of the 83 assessable patients, 55 (66%) were classified as ruxolitinib resistant, and 27 (33%) were classified as ruxolitinib intolerant. There was one patient who discontinued ruxolitinib for unclear reasons. The median duration of exposure was 10.25 months, and 40% had achieved a 50% reduction in spleen size while on ruxolitinib. The primary reason for intolerance was hematologic toxicity. Shortly after completion of accrual, studies using fedratinib were placed on hold due to 8 cases of WE of the 670 patients treated with fedratinib over multiple studies. Therefore, the median number of cycles was 6, ranging from 3.9 to 8.9, which limited the ability to assess efficacy. Nonetheless, of the evaluable patients, 46 of 83 (55%) experienced a spleen response. Of the 97 patients included in the intention-to-treat population, a 50% reduction in spleen size was noted in 33 (34%) patients and 30 (31%) patients after three and six cycles, respectively. Of the 90 patients evaluable for the symptom response, 26 achieved a 50% reduction in MPN-SAF score. The most commonly observed toxicities were anemia, thrombocytopenia, and gastrointestinal disturbances such as nausea, vomiting, and diarrhea. Unfortunately, due to the early termination of the study, the benefit of fedratinib in this population was unable to be fully assessed.
Re-analysis of the JAKARTA- 2 data was done earlier this year, which applied more stringent criteria of ruxolitinib failure. In this new analysis, more specific definitions were applied, including treatment >3 months with regrowth of spleen, or failure of an adequate response specifically defined by less than 10% reduction of SVR or <30% reduction in spleen size. Intolerance was further clarified as patients who were treated with ruxolitinib for at least 28 days and experienced transfusion requirements, grade 3 thrombocytopenia, or bleeding complications. In this patient population, 30% achieved >35% SVR. 11
WE is an acute neuropsychiatric disorder characterized by nystagmus and ophthalmoplegia, mental-status changes, and unsteadiness of stance and gait. 12 This syndrome is caused by exhaustion of thiamine. There is conflicting data regarding the prevalence of WE in patients with myeloproliferative diseases. A group published a population study of 39,761 patients with MPN compared with an age- and gender-matched control population. 13 They found that those with MPN had a higher rate of WE as compared with those without MPN [MPN versus non-MPN: 1.09 versus 0.39/1000 person-years, adjusted hazard ratio (HR) = 2.19, 95% confidence interval (CI) 1.43–3.34]. However, interestingly, in another study of 97 MPN patients in a single center, none of the patients had a thiamine deficiency. 14 Harrison et al. reviewed the entire group of patients treated with fedratinib for MPN or other disorders; 8 patients (of 677) were diagnosed with WE. 15 Of these eight patients, six had MF, one had polycythemia vera, and one had metastatic head and neck cancer. A careful retrospective review was performed with an external expert panel review. In three patients, the data did not fully support the diagnosis of WE. In the five remaining patients, there was one patient who clearly had WE, two patients who had a high suspicion of WE, and two who did not have a clear diagnosis. Of the three who either definitely had WE, or had a high index of suspicion, the patients had severe malnutrition from a variety of causes that likely contributed to the thiamine deficiency. In two of them, symptoms resolved without interruption of medication. With this revised analysis, the incidence of WE was 3–5 patients out of 670, suggesting a prevalence of 0.4–0.7%. Ultimately, after review of all of this data, it was felt that there was not an increased risk of WE in patients who were treated with fedratinib.
Following this, the FREEDOM study was designed, a phase IIIb study evaluating the efficacy of fedratinib in patients who are resistant or intolerant to ruxolitinib based on the more stringent definitions used by Harrison et al. 15 in the secondary analysis of the JAKARTA-2 data. This study is ongoing.
In August 2019, fedratinib received approval for treatment of intermediate and high risk PMF, post-PV MF, and post-ET MF with a platelet count >50 × 109/l. There is a black box warning about WE, and providers must check thiamine prior to initiating therapy.
JAK inhibitors advanced in the pipeline
There are two other new JAK-i which have (1) completed successful phase III trials, and (2) are completing additional steps seeking Food and Drug Administration (FDA) approval: momelotinib and pacritinib. These medications are beneficial to specific groups of patients: momelotinib has mechanisms that make it attractive for patients with anemia, and pacritinib is targeted for patients with low platelets. For a summary of the trials involving ruxolitinib, momelotinib, and pacriticinib, please see Table 2.
Major studies for JAK-i.

BAT, best available treatment; FEDR, Fedratinib; JAK, Janus kinase; JAK-i, Janus kinase inhibitor; MMB, Momelotinib; PAC, Pacritinib; RUX, Ruxolitinib; SVR, spleen volume reduction.
Momelotinib is a JAK1/2 inhibitor, as well as directly inhibiting the bone morphogenic protein receptor kinase activin A receptor, type I (ACVR1)-mediated expression of hepcidin. 22 This not only provides JAK inhibition, but also has a beneficial impact on anemia. Two studies have evaluated the efficacy of momelotinib: SIMPLIFY-1, and SIMPLIFY-2. SIMPLIFY-1 was a study for JAK inhibitor naïve patients, and compared ruxolitinib with momelotinib in patients who were naïve to JAK inhibitor. 18 The primary endpoint was reduction of SVR of 35%, which was achieved in 26.5% (57 of 216) of patients who received momelotinib and 29.0% (63 of 217) of patients who received ruxolitinib. The secondary endpoint of ⩾50% reduction in MPN-total symptom score (MPN-TSS) was achieved in 28% of patients who received momelotinib, and 42.2% of patients who received ruxolitinib, indicating less symptomatic improvement in patients who received momelotinib. Another secondary endpoint was transfusion independence; 65.5% of patients who received momelotinib were transfusion-independent at week 24, whereas only 49.3% of patients who received ruxolitinib were transfusion-independent at this timepoint.
SIMPLIFY-2 was a randomized study of momelotinib versus BAT for patients who had inadequate response to ruxolitinib. This was defined as requiring a blood transfusion, or having a hematologic toxicity that necessitated reducing the dose of ruxolitinib to <20 mg a day. 19 The primary endpoint was reduction in spleen volume by 35%, secondary endpoint was reduction in the symptom score. In this study, there was no significant difference in SVR between momelotinib and BAT (7% versus 6%, respectively). A reduction in TSS of at least 50% was observed in 26% of patients receiving momelotinib compared with 6% of those receiving BAT. It is notable that, of the BAT arm, 89% were on ruxolitinib. 19 Based on the results of SIMPLIFY-2, as well as the fact that in SIMPLIFY-1 there was an inferior improvement in MPN-TSS compared with ruxolitinib, momelotinib was not approved. However, in light of the clear benefits of momelotinib with regards symptoms and spleen response in patients with anemia, and development of transfusion independence, a new phase III study, MOMENTUM, is underway, which compares danazol with momelotinib.
Pacritinib is a selective JAK2 inhibitor that has been shown to reduce spleen size in patients who have anemia and thrombocytopenia. PERSIST-1 was a study that compared pacritinib 400 mg daily with BAT (excluding ruxolitinib) in a 2:1 randomization. There were no specific exclusion criteria based on thrombocytopenia or anemia. The endpoints were designed to be assessed at 24 weeks. The primary endpoint was SVR of ⩾35%, and the secondary endpoint was 50% reduction in MPN-SAF. The study was stopped early due to unexpected poor outcomes in PERSIST-2, so the median time of follow up was 23.2 months; therefore, the analysis was difficult. Of the 327 patients randomized in this study in a 2:1 fashion, 220 were assigned to pacritinib, and 107 to BAT; however, due to the early study closure, only 168 in the pacritinib arm, and 85 in the BAT arm were evaluable. In the intention-to-treat population, 19% in the pacritinib arm and 5% in BAT arm achieved ⩾35% SVR. At week 24, in the intention-to-treat population, a 50% reduction of MPN-SAF was achieved in 19% in the pacritinib arm, and 10% in the BAT arm, a difference that was not statistically significant. 20
The PERSIST-2 study was carried out in patients who had a platelet count of less than 100. Approximately half the patients had been exposed to ruxolitinib. This study compared pacritinib 400 mg daily, pacritinib 200 mg BiD, and BAT (which included ruxolitinib) in patients. Reduction in SVR was appreciated in 18% of patients in the pacritinib arm, versus 3% patients in the BAT arm. Greater than 50% reduction in MPN-SAF was appreciated in 25% versus 14%, which was not clinically significant. A superior response was observed in the arm receiving pacritinib 200 mg twice a day. In February 2016, a clinical hold was placed on pacritinib, after reports of deaths due to bleeding and cardiac events were reported on patients enrolled in the studies. Ultimately, after extensive evaluation, it was felt that these deaths were more related to the underlying illness of the patients rather than the medication itself. Pacritinib was re-evaluated in a phase III dose-finding study (PAC203) comparing pacritinib 100 mg daily, 100 mg twice a day, and 200 mg twice a day; 35% SVR was noted in 9.3%, 1.8%, and 0% and 50% reduction in MPN-SAF was noted in 7.4%, 5.5% and 5.8% of patients receiving 200 mg BID, 100 mg BID, and 100 mg daily, respectively. 23 There is currently an ongoing study called PACIFICA, which compares pacritinib 200 mg BiD with physician’s choice (which may include low-dose ruxolitinib) in patients who have had either no exposure, or minimal exposure (<3 months), to JAK-I. Despite all of the issues surrounding the studies, it is important to note that this medication has resulted in significant SVR in patients who historically have been very difficult to manage based on thrombocytopenia.
Summary
How does this change the landscape of treatment for MF? First, it provides a second option for up-front therapy, although there are no current data comparing ruxolitinib versus fedratinib in a front-line setting. There are fairly equal response rates with regards to spleen size and symptom burden. Grade 3–4 side adverse events such as anemia and thrombocytopenia were quite similar, and there was a little more lymphopenia described in fedratinib (17% in fedratinib versus 7% with ruxolitinib). However, that being said, the durability of the response with fedratinib is not known, as the initial studies required early termination. There are ongoing analyses of subgroups to assess whether there are subpopulations one should consider to begin with fedratinib. In addition, it provides an excellent option for those who have failed ruxolitinib due to significant residual symptoms, problematic splenomegaly (i.e. aligned with the JAKARTA-2 population), etc.
Once the other JAK-i are available, there will be an array of treatment options available to patients regardless of their counts. There will also be excellent alternatives for patients who do not tolerate one of the JAK-i due to side effects.
Future directions
Over the last 10 years, ruxolitinib has been explored in other clinical settings. First, it also has approval for use in polycythemia vera, 24 and is being tested for use in essential thrombocythemia. 25 Ruxolitinib has also been combined with a number of other agents in the treatment of MF. 26 It provides significant symptom improvement, whereas there may be other disease-modifying effects provided by other agents. Moving forward, with the differences in fedratinib versus ruxolitinib, there may be new avenues of treatment with combination therapy. As other JAK-i are approved, this can be expanded further, allowing more patients to benefit from novel treatment strategies. Ruxolitinib has also been evaluated in the pre-stem cell transplant setting, with favorable results.27,28 Ruxolitinib has also been explored for other diagnosis, and has recently received approval for use in graft versus host disease, a complication of allogeneic stem cell transplantation, exploiting the anti-inflammatory effects of the drug. 29 Moving forward, fedratinib, as well as other JAK- i, will also be tested in these settings, expanding therapeutic options for not only patients with MPN, but other indications as well.